Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Victor Skumin wikipedia , lookup
Psychiatric and mental health nursing wikipedia , lookup
Generalized anxiety disorder wikipedia , lookup
History of psychiatric institutions wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Conversion disorder wikipedia , lookup
Glossary of psychiatry wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
Abnormal psychology wikipedia , lookup
Psychological evaluation wikipedia , lookup
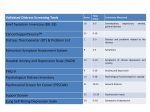
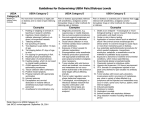
Psychosocial Distress Screening Nina Miller, MSSW, OSW-C Psychosocial Distress Screening Commission on Cancer Standard Standard 3.2 The cancer committee develops and implements a process to integrate and monitor on-site psychosocial distress screening and referral for the provision of psychosocial care. Distress in Cancer NCCN defines distress as a multifactorial unpleasant emotional experience of a psychological, social, and/or spiritual nature that may interfere with the ability to effectively cope with cancer, its physical symptoms and its treatment. Distress extends along a continuum ranging from common normal feelings of vulnerability, sadness, and fears to problems that can become disabling, such as depression, anxiety, panic, social isolation and existential and spiritual crisis. Psychosocial Distress Screening CoC Process Requirements: Timing of Screening - Patients with cancer are offered screening for distress a minimum of one time per patient at a pivotal medical visit to be determined by the program. Methods - The mode of administration (such as patient questionnaire, clinicianadministered questionnaire) is determined by the program. CoC Process Requirements, cont. Tools - Facilities select the tool to be administered to screen for current distress. Preference is given to standardized, validated instruments with established clinical cutoffs. Assessment and Referral – The oncologist, nurse and social worker are to identify and examine the psychological, behavioral and social problems of patients that interfere with their ability to participate fully in their health care and manage their illness and its consequences. • The oncology team (oncologist, nurse, social worker) reviews the distress screening results to determine the need for referrals to interventions e.g. educational programs, support groups, counseling, exercise, relaxation, meditation for expected distress symptoms e.g. sadness, worry, anger, preoccupation with thoughts of illness. • If the distress screening reveals a higher score, the oncology team should complete a clinical assessment with referral to mental health, social work/counseling or chaplaincy. MENTAL HEALTH EVALUATION DIAGNOSIS DISTRESS DEMENTIA BEHAVIORAL PROBLEMS DELIRIUM PSYCHIATRIC HISTORY/MEDS MOOD DISORDER PAIN/SYMPTOM CONTROL SCHIZOPHRENIA/PSYCHOTIC DISORDER BODY IMAGE/SEXUALITY ADJUSTMENT DISORDER IMPAIRED CAPACITY ANXIETY DISORDER SAFETY SUBSTANCE-RELATED DISORDER OR ABUSE PSYCHIATRIC DISORDER PERSONALITY DISORDER Documentation for Survey • Screening, referral or provision of care and follow-up are documented in the patient’s medical record to facilitate integrated, highquality care. • The program completes the Survey Application Record. • The program provides cancer committee minutes along with other sources to document the development and implementation of a process to integrate and monitor distress screening and referral for the provision of psychosocial care. 29-43% distress among sample of 4,500 adults with seven common types of cancer. Zabora et al. Psych-Onc 2001 Consequences of Distress • • • • • • Decreased employment functioning Decreased medical adherence Increased medical costs Increased health risk behaviors Decreased health protection behaviors May interfere with cancer outcomes • Physicians substantially underestimate oncology patients’ psychosocial distress. • Patients are willing to discuss distress but are not likely to initiate the conversation with the physician. • Physician’s often defer to the patients to raise any concerns about distress-related topics. Fallowfield et al. 2001; Keller et al. 2004; Merckaert et al. 2005; Detmar et al JCO 2000 Screening Methods Method Pros Cons Clinicianadministered questions -Immediate interpretation and triage -Time intensive -Patient may not disclose sensitive personal information Patient questionnaire: Paper based -Can be completed at patient convenience, e.g. while waiting for appt. -Provides more privacy than face-to-face questions -Requires real-time review of responses for completeness of responses, elevated distress -Requires patient literacy skills Patient questionnaire: Electronic assessment -Integration with electronic health record possible -Automated scoring and interpretation -Automated triage possible -Requires patient to have Internet access or in-clinic access -Programming for EHR integration costly Distress Screening Tools • • • • • • NCCN Distress Thermometer PHQ-9 PHQ-2 Hospital Anxiety and Depression Scale Brief Symptom Inventory – 18 Beck Depression Inventory Single Item Distress Thermometer Screening Cut-off = 5 Sensitivity Specificity Anxiety .85 .78 Depression .63 .69 Butt et al. JPSM 2007; 35:20-30 • Patient Reported Outcomes Measurement Information System (PROMIS) • NIH-funded network • www.nihPROMIS.org • Brief, precise measures of cancer-related symptoms through computer adaptive testing • Assessment Center provides platform for online administration of PROMIS measures PROMIS Computer Adaptive Testing assesses these domains: • • • • • Depression Anxiety Fatigue Pain Physical function TOTAL LENGTH: 40 items Sample Depression Question Assessment and Messaging at the Robert H. Lurie Comprehensive Cancer Center • New patients receive instructions to activate EHR patient communication portal (Epic MyChart) • Patients access Epic MyChart • MyChart links seamlessly with Assessment Center within organization firewall • Patient completes assessment through Assessment Center (at home or in-clinic) • Provider messages and triage managed through Epic health record integration Social Work Needs Assessment In-Clinic Assessment Provided via iPad Screening Triage Algorithm Depression, Anxiety 1) MD, RN message when symptoms are moderate/severe (70th %ile) 2) Psychology, Social work copied to initiate consult Practical, financial concerns Social worker sent message with list of needs expressed by patient to initiate consult RHLCCC Screening: Patient Feedback • Median age = 61.5 (range 34-73) • Administration 10.7 minutes (range 6-22 minutes) • All patients reported assessment was “easy” or “very easy” • Questions too personal? 100% “Not at all” Did the survey ask questions about aspects of your health and wellbeing that are important to you? 8 7 6 4 2 1 0 Not at all A little bit 2 Somewhat Very much Do you think it's important for your medical team to know your results from these surveys? 7 6 5 4 3 2 1 0 6 4 Not at all A little bit Somewhat Very much Implementing Distress Screening Standard at Your Institution • Determine timing for screening e.g. new patients, at certain points of transition • Determine methods e.g. clinician administered, selfadministered • Tools: Select tool and cut-off based on resources for administration • Determine how you will refer patient for assessment • Establish community, state and national referral sources • Identify psychosocial staff at your institution and/or establish referral agreements with providers external to your organization Thank you