Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
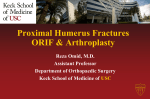
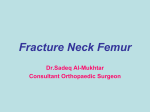
CASE REPORT: GREATER TUBEROSITY FRACTURE IN A CYCLIST. A mountainbiker fell onto the shoulder during a downhill descent and presented to his sports physician with a tender proximal humerus. There was point tenderness over the tuberosity. Shoulder movement was limited and painful. The differential diagnosis included rotator cuff tear, fracture and traumatic bursitis. The patient progressed to radiology for standard X-rays, which could not demonstrate a fracture. An MRI was performed to assess the rotator cuff. The MRI showed and undisplaced fracture of the greater tuberosity. No tear of the cuff was noted. Fig.1.Coronal MRI right shoulder. STIR sequence shows fracture of the greater tuberosity with associated bone marrow oedema. Fig.2.Coronal MRI shoulder. T1 sequence shows fracture optimally. The patient was immobilized with a shoulder sling. The recovery period was uncomplicated and full recovery was obtained. Discussion The standard X-ray anterior-posterior view with external rotation detects fractures of the greater tuberosity optimally.(1) Anterior dislocation of the shoulder is associated with fracture of the greater tuberosity.(3) When a radiograph is normal or equivocal, but the clinical question of a fracture remains, MR imaging may be the key in the diagnosis. In the past, continued evaluation would be accomplished with bone scanning, requiring hospital admission and a potential delay in diagnosis and treatment. However, MR imaging is far more sensitive in this setting and is now the recommended method of evaluation.The diagnosis can be made on a single T1-weighted coronal study. There may be accompanying injuries or abnormalities such as muscle tears, however, and a oedema –sensitive STIR study may add useful information. (2). Neer classifies upper humeral fractures into 4 segments : (i) those involving the anatomic neck of the humerus, (ii) those involving the greater tuberosity, (iii) those involving the lesser tuberosity, and (iv) those involving the shaft or surgical neck of the humerus. Fractures of the greater tuberosity are classified as onepart fractures (7) A one-part fracture has either no displacement or angulation of any of the segments, or displacement and angulation are minimal. Displacement is defined by fracture segment of greater than 1 cm or angulation of more than 45 degrees. A two-part fracture involves displacement of one segment. A three-part fracture involves displacement of two segments with an associated uninpacted surgical neck fracture with rotatory displacement. A four-part fracture is characterized by displacement of all four segments.(7) Eight percent of proximal humeral fractures have minimal or no displacement and are held together by the rotator cuff, capsule and periosteum.(7) MR imaging is particularly useful in identifying one-part or non-displaced fractures not detected on conventional radiographs.(2,7) A recent radiological study (non-arthrogram MRI) noted no associated rotator cuff pathology on MRI in patients presenting with radiographically occult one-part fractures of the greater tuberosity.(5) Another MR-based study (using MR arthrography), however, showed a high association between clinical traumatic rotator cuff tears and greater tuberosity fractures. It was noted that in the under 40 year age group fractures of the greater tuberosity were more prevalent (8) A recent arthroscopic study performed showed that all fractures of the greater tuberosity had partial thickness articular surface tears of the rotator cuff. Arthroscopic repair was advocated. Most of the athletes returned to the previous level of activity. Athletes involved in overhead sports had limited recovery.(4) The results of a recent preliminary study suggest that the patients presenting with a one-part fracture of the greater tuberosity of the proximal humerus should be evaluated individually.(6) In most patients in whom the displacement of the fragment is less than 5 mm, good results can be obtained with non-operative treatment . If the displacement of the fragment is more than 5 mm in young active patients, and more than 3 mm in individuals (especially athletes and heavy laborers) involved in overhead activity , the fragment should be mobilized, repaired, and fixed into its original bed or slightly inferolaterally.(6) REFERENCES: 1. Anderson IF, Read JW, Steinweg J. Atlas of Imaging in Sports Medicine . Sydney: McGraw-Hill Companies, Inc., 1998 : 107. 2. Andrews C. Evaluation of the Marrow Space in the Adult Hip. Radiographics October 2000,Vol.20:33-34 3. Ilahi OA. Irreducible anterior shoulder dislocation with fracture of the greater tuberosity.Am J Orthop. 1998 Aug;27(8):576-8. 4.Kim SH, Ha KI. Arthroscopic treatment of symptomatic shoulders with minimally displaced greater tuberosity fracture.Arthroscopy. 2000 Oct; 16(7):695700. 5. Mason BJ, Kier R, Bindleglass DF. Occult fractures of the greater tuberosity of the humerus: radiographic and MR imaging findings.AJR Am J Roentgenol. 1999 Feb;172(2):469-73. 6. Park TS, Choi IY, Kim YH, Park MR, Shon JH, Kim SI. A new suggestion for the treatment of minimally displaced fractures of the greater tuberosity of the proximal humerus. Bull Hosp Jt Dis 1997;56(3):171-6 7. Stoller DW, Wolf EM .MRI in Orthopaedics and Sports Medicine, 2nd Edition :Philadelphia, Lippincott-Raven Publishers, 1997: 728-730. 8. Zanetti M, Weishaupt D, Jost B, Gerber C, Hodler J. MR imaging for traumatic tears of the rotator cuff: high prevalence of greater tuberosity fractures and subscapularis tendon tears.AJR Am J Roentgenol. 1999 Feb; 172(2):463-467.