Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
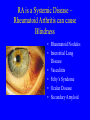
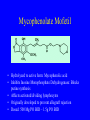
Rheumatology Overview, 2008 Focusing on RA and SLE Jonathan Graf, M.D. Assistant Adjunct Professor of Medicine, UCSF Division of Rheumatology, San Francisco General Hospital Arthritis - Misconceptions • “You’re an Arthritis Doctor. What’s it like taking care of so many old patients” • “Are all of your patients in wheelchairs?” • “Arthritis is not a big deal because it’s not life-threatening” All Arthritis Patients are Old • Many forms of Arthritis • Rheumatoid Arthritis commonly affects young women of childbearing age • Osteoarthritis affects younger people who run, have traumatized their joints, are overweight, etc…. • Gout can affect people of all ages Wheelchairs and Canes • Thanks to recent advances and medical research, not as many face life in a wheelchair • Treatments for many inflammatory arthritic conditions such as Spondylitis and Rheumatoid Arthritis have improved dramatically • Joint replacement surgery has improved outcomes in Osteoarthritis Arthritis is not Life-Threatening • Systemic inflammatory diseases that cause arthritis can affect other organs and lead to lifethreatening complications • Chronic inflammation has now been linked to heart disease • Advanced Osteoarthritis limits mobility and can lead to secondary health problems (obesity, heart problems, etc…) • An in cases that aren’t life-threatening, since when is living in pain not life-altering/life-imparing. Judgement call!! Arthritis All forms of arthritis are not created equal • Inflammatory – – – – RA SLE Crystalline (Gout) Vasculitis • Non-Inflammatory – Osteoarthritis • “Arthritis”-like diseases – Fibromyalgia Inflammatory Arthritis Joint swelling Joint warmth Joint redness Joint pain and stiffness Morning>Afternoon symptoms Worse with rest, better with use (gelling) Can Have Systemic Components Inflammatory Arthritis- A Component of Rheumatic Diseases • Arthritis is a common, unifying feature to a whole host of systemic auto-immune and inflammatory diseases!!! • Characteristic pattern may vary by disease • Crystals and inflammatory reaction – Gout, pseudogout • Rheumatoid Arthritis • Seronegative Spondyloarthropathy – Ankylosing spondylitis – Psoriatic Arthritis – Reactive Arthritis – Inflammatory Bowel Disease Associated Arthritis Inflammatory Arthritis, Diseases • • • • • • • Lupus Scleroderma Myositis Hashimoto’s Thyroiditis Sjogren’s Syndrome Many More!!!!! Arthritis is a common, unifying feature to a whole host of systemic auto-immune diseases!!! Rheumatoid Arthritis • One cause of inflammatory arthritis • Systemic inflammatory disease, primarily involving the synovial membrane of diarthrodial joints • Prevalence in North America between 1-2% • Most prevalent in women of child-bearing age (4th-6th decade) • Can occur in any person at any age ACR Criteria for Diagnosis of RA (4 of 7) • • • • • • • Morning Stiffness>1 hr. duration Arthritis of 3 or more joints Arthritis of the hand joints Symmetric arthritis Rheumatoid nodules Serum rheumatoid factor Radiographic changes RA, Etiology • Probable background genetic susceptibility (multiple genes/risk factors involved) – Concordance rates 15-30% identical twins – 2.5-3.0 times more prevalent in Women>Men • Likely environmental triggers in people with genetic susceptibility – Disease of the New World, ? 16th C. Ohio river valley – Not seen until late 18th century in Europe Genetic Risk Factors • • • • Family history Female Sex Specific genes: HLA-DR4 Specific region in HLA DRB1 gene confers increased risk of RA and severity Non Genetic Risk Factors • ? Bacterial or Viral Agent – Parvovirus, Hepatitis, Lyme, and Rubella • ?Environmental Triggers – Tobacco, Caffeine RA, Clinical Features How to Differentiate from other Osteoarthritis • Symmetric polyarthritis • Usually small-medium joints are involved • Generally chronic disease (20% acute onset) • Often leads to erosive, deforming, and disabling disease • 20% have extra- articular manifestations Ethical Question: Does a disease have to be “life-threatening” for it to be considered important?..... The ravages of a chronic destructive arthritis. How does this person walk???? RA is a Systemic Disease – Rheumatoid Arthritis can cause Blindness • Rheumatoid Nodules • Interstitial Lung Disease • Vasculitits • Felty’s Syndome • Ocular Disease • Secondary Amyloid Rheumatoid Nodules RA – Vasculitis. Rheumatoid Arthritis can be life-threatening RA – Synovitis: This is what an inflammatory arthritis looks like. 81 YO female with Rheumatoid Arthritis RA – R>L Knee Synovitis: 81 YO Female Patient RA – Rheumatoid Nodules Normal Joint Histology • Synovial lining 1-2 layers of synoviocytes • Sub-lining layer of loose connective tissue and blood vessels RA Joint Pathology • Inflammation, capillary leak, fibrin deposition • Synovial Hyperplasia • Cellular infiltrate – Macrophages – Lymphocytes – Can resemble lymphoid tissue in 1/3 RA Pathology • Synovium becomes laden with macrophages, fibroblasts, and multinucleated giant cells (resemble osteoclasts) • Synovial membrane (pannus) expands, actively invades and erodes surrounding bone and cartilage Rheumatoid Arthritis • Disability costs are high, both in terms of direct and indirect medical costs – 35% of patients with 10 years disease duration are work-disabled – Decline from 50% rate reported in 1987 Arthritis Rheum. 2008 Mar 27;59(4):474-480 RA: Chronic Joint Destruction and Disability – What We Try to Prevent Ra: Traditional Treatment Paradigm • Pyramid of therapy – Start conservatively – Gradually ascend the pyramid in order of potency and toxicity of therapy – Only the most severely affected patients receive immuno-supressive, DMARDs – DMARD therapy begun only after period of significant delay Re-Thinking the RA Treatment Pyramid • Emphasizes earlier diagnosis and initiation of therapy with disease modifying anti-rheumatic drugs Early RA: The Window of Opportunity to Intervene The Window of Opportunity Eventually Closes for Many…. • Chronic disease progression leads to permanent joint deformity, destruction, and disability • Empirically, RA is a different disease the longer disease activity progresses without effective control – More difficult to suppress activity and treat – More extra-articular disease? ACR RA Practice Guidelines 2002 • Most patients with Rheumatoid Arthritis should be evaluated expeditiously • Treatment with DMARD instituted within 3 months of diagnosis • Goals are to prevent or control joint damage, prevent loss of function, and decrease pain RA Pharmacologic Therapy: DMARDs • • • • • • • • Methotrexate Leflunomide (Arava) Sulfasalazine Azathioprine Mycophenolate Mofetil “Corticosteroids” “Hydroxychloroquine” “Minocycline” Methotrexate • Cornerstone DMARD, now 1st line therapy, alone or in combination for mod.-severe RA • Blocks Dihydrofolate reductase • Inhibits production of tetrahydrofolate, a single carbon donor • Leads to diminished production of purines and inhibits DNA synthesis (although there are other mechanisms likely involved) • Reduces proliferative potential of replicating immune and inflammatory cells Methotrexate • Long-term benefits in symptom improvement & retardation of joint damage • Long term – well tolerated with acceptable safety profile (no ETOH) • Available as IM/liquid/tablet preparations • Starting dose 7.5 mg/WEEK – up to 25 mg/wk • Renally cleared – be careful and adjust dose Methotrexate Adverse Events • • • • • • • • GI - Mucositis, diarrhea, abdominal pain Hematologic - Cytopenias, macrocytosis Hepatic- Transaminitis, fibrosis, and cirrhosis Pulmonary - Hypersensitivity pneumonitis, pulmonary fibrosis Infections Neoplasia - reversible lymphoproliferative disorder, lymphoma, and leukemia Accelerated nodulosis and vascultitis Reproductive – abortifacient and teratogen – Must use birth control and d/c drug 2-6 months before planned pregnancy Combination DMARD Therapies: Some Step Up, Others Step Down • Methotrexate +SSZ +Plaquenil +/- Prednisone • Arava + SSZ + Plaquenil +/- Prednisone • Methotrexate X Arava ----- Generally not done • More and more, combination therapies of DMARDs and Biologic medications being used earlier in the course of treatment Why Move Towards Combination Regimens with Biologics?? The Current Pyramid Paradigm • Early initiation and titration of DMARD • If incomplete response to DMARD alone, after reasonable titration, addition of biologic recommended Biologic Therapies • What is meant by the term Biologic Therapy? • Double meaning: – Organic compounds made by living cells • As opposed to products from a chemistry lab – Modify biologic responses • Antibody-antigen interactions • Cytokine-receptor interactions (both ends) • Cell signaling proteins, inhibitors, or ligands Families of Biologic Therapies • Anti-Tnf medications – Etanercept (cytokine receptor fusion protein) – Infliximab (anti-cytokine antibody) – Adalimumab (anti-cytokine antibody) • B-cell depleting agents (monoclonal antibody) – Rituximab • T-cell costimulation inhibitors (receptor-ligand ) – Abatacept • Il-1 Inhibitors (Il-1 cytokine receptor decoy) – Anakinra Anti-TNF Family of Biologics Anti-Tnf medications Etanercept (cytokine receptor fusion protein) Infliximab (anti-cytokine antibody) Adalimumab (anti-cytokine antibody) TNF Effects: The Good and the Bad • Good: TNFa and TNFb regulate biological functions necessary for normal inflammatory and immune responses. – TMF-a absolutely essential for granulomatous host defenses against intracellular bacteria – MTb, fungal infections, listeria • Bad: TNF-a binds membrane-bound TNF receptors and mediates pro-inflammatory processes implicated in inflammatory arthritis. Man-Made Advances in TNF Biology • The family of anti-TNF therapies – Etanercept (Enbrel) – Infliximab (Remicade) – Adalimumab (Humira) Etanerceot Infliximab Adalimumab Etanercept • Etanercept recombinant, dimeric fusion protein • Consists of the soluble human p75 tumor necrosis factor (TNF) receptor coupled to the Fc fragment of human IgG1 lacking the CH1 domain. • Binds soluble TNF-a and TNF-b and prevents activation of TNF-Rs Infliximab • Infliximab is a “humanized” monoclonal antibody • TNF binding region derived from mouse antiTNF monoclonal antibody • Attached to constant region of human IgG1 kappa antibody. • Chimeric molecule not 100% human Adalumimab • Adalimumab is a recombinant, fully human monoclonal IgG1 kappa antibody. • All monoclonal anti-TNFs bind membrane bound and soluble TNF (May have added benefit leading to clearance or apoptosis of cells expressing surface TNF) • All monoclonals bind only TNF-alpha (not TNF-b) – May explain differential effects of anti-TNF medications in IBD The Anti-TNF Clan • Differences between agents: Enbrel Ab Form. Human T½ N Injection Y S Remicade Y Infusion N L Humira Y Injection Y L Contraindications • History of latent tuberculosis unless/until they have completed an adequate courses of prophylactic therapy (Duration up for debate) • Active acute or chronic infections (HCV may become exception) • Active or suspected malignancies. • Hypersensitivity to an anti-TNF agent or mouse product (infliximab) • Anti-TNF agents in the setting of hepatic disease or renal failure has not been studied. • Anti-TNFs are generally contraindicated in patients with moderate or severe congestive heart failure (some have black box warning) • History of demyelinating disease Anti-TNFs: Like all success stories, there are always complications • Increased risk of infections! (OR of 2.0 for serious infection in large meta analysis published in JAMA 2006) • Increased malignancy risk: Always thought of as a theoretical risk, now controversial evidence that RA patients may be at increased risk of lymphoma and/or solid tumors • May worsen symptoms of congestive heart failure. Anti-TNF Therapy: Allergic and Idiopathic Reactions • Dermatologic reactions – – – – Localized: Mild-moderate injection site reactions erythema, pruritis, pain, and/or swelling reactions are commonly self-limiting early in the course of therapy. FDA has recent case reports of Steven’s Johnson and TEN with all three • Infusion reactions, especially with infliximab – within 1-2 hours after receiving the therapy – fever, chills, urticaria, and cardio-pulmonary symptoms – antibody mediated serum-sickness type of syndrome also reported that’s separate than from typical infusion reaction Systemic Lupus Erythematosis • Systemic Disorder, involving multiple organs in multiple ways • Women:Men = 9:1 • African American/Caribbean in US/UK: Dz. is 3 times more common • Peak Age of Onset 20’s & 30’s • Incidence has tripled since 1970’s to 5.56/100,000 population SLE: ACR Criteria: 4 of 11 Criteria without better explanation (Not diagnostic) • • • • • • • Malar Rash Discoid Rash Photosensitivity Oral Ulcers Arthritis Serositis Renal Disorder SLE Criteria Cont. • • • • Hematologic Disorder Immunologic Disorder ANA Neurologic Disorder Malar Rash • Fixed malar distribution of erythema, flat or raised Discoid Rash • Erythematous raised patches with keratotic scaling and follicular plugging; some atrophic scarring in chronic lesions Photosensitivity • Skin rash as an unusual reaction sunlight, by patient history or physical examination Oral Ulcers • Oral or nasopharyngeal ulcers, usually painless, observed by a physician Arthritis • Non-erosive arthritis involving two or more peripheral joints, characterized by tenderness, swelling, or effusion Other SLE Criteria • Serositis – Pleuritis (convincing history of pleuritic pain or rub heard by a physician or evidence of pleural effusion – Pericarditis (documented by EKG, rub, or evidence of pericardial effusion) • Renal Disorder (can lead to renal failure) – Persistent proteinuria >0.5g/day (or>3+) – Cellular casts of any type (glomerulonephritis) Hematologic Abnormalities • Hemolytic anemia (usually coomb’s positive) • Leukopenia (WBC < 4,000 on at least 2 occasions) • Lymphopenia (<1500 on 2 or more occasions) • Thrombocytopenia (PLT<100,000 on 2 or more occasions) Immunologic Disorder One of the Following • Anti-dsDNA • Anti-Smith • Positive findings of anti-phospholipid Abs – Abnormal level of either IgG or IgM CLIP Abs – Positive test for Lupus Anticoagulant (RVVT) – False positive RPR/VDRL > 6months neg. FTA Positive ANA • An abnormal titer of ANA in the absence of drugs known to be associated with “druginduced lupus syndrome” Neurologic Disorder • Classically defined only as: – Seizures (in the absence of other causes) – Psychosis (in the absence of other causes) • Other CNS manifestations – Headaches – Cognitive dysfunction Organ System Involvement in Flares of SLE, Hopkins Cohort:1991 • • • • • • • • Constitutional Musculo-skeletal Dermatologic Renal Neurologic Hematologic Serositis Pulmonary 66% 58% 47% 22% 21% 17% 12% 7% Permanent Organ Damage in SLE, Hopkins Cohort: 1991 • • • • • • • • • • • Musculo-skeletal Neuro-psychiatric Ocular Renal Pulmonary Cardiovascular GI Skin Peripheral Vascular 5.5% Malignancy Premature Gonadal Failure 25.2% 15% 12.6% 11.7% 10.4% 10.1% 7.4% 7.4% 2.5% 1.2% Cyclophosphamide • Pulse IV therapy mainstay for Diffuse Proliferative GN secondary to SLE • Less-studied, but significant therapy for severe systemic manifestations – CNS vasculitis – Transverse Myelitis – Pulmonary capillaritis/ diffuse alveolar hemorrhage/severe interstitial pneumonitis Cyclophosphamide Therapy: Glomerulonephritis • 0.5 – 1.0 g/m2 dosed monthly for 6 months • 1 mg/kg/day concomitant prednisone Rx. • Dosed every 3 months for next 18 months • 5-year renal survival rates: 60-90% • Frequent monitoring – Cell counts nadir 10-14 days post therapy – Urinalysis: Hemorrhagic cystitis Annals of Internal Medicine, 2001 Cyclophosphamide: Side Effects • Short-Term – Nausea, alopecia – Immunosupression, opportunistic infections – Cytopenias • Medium-Term – Hemorrhagic Cystitis • Long Term – Transitional Cell Carcinoma – Hematologic malignancies – Infertility • Non-responders (to follow) • Relapses: Re-treat or try alternative therapies Minimizing Toxicity: Other options? • Lower, more frequent dosing of Cytoxan • Shorter courses of induction therapy followed by maintenance therapy – Azathioprine – Mycophenolate Mofetil • Induction therapy with MMF Mycophenolate Mofetil • Hydrolyzed to active form: Mycophenolic acid • Inhibits Inosine Monophosphate Dehydrogenase: Blocks purine synthesis • Affects activated/dividing lymphocytes • Originally developed to prevent allograft rejection • Dosed: 500 Mg PO BID – 1.5g PO BID Potential Novel Therapies • Anti B-cell therapies • Anti-T-cell therapies – Co-stimulatory signal blockade • Vaccination Strategies • Marrow Ablation - Transplant B-cell Depleting Therapies: Rituximab • Attractive for diseases characterized by aberrant, pathologic auto-antibody formation (SLE, APLA, ITP) • CD20 expressed almost exclusively on Bcells • CD20 not expressed on Plasma cells • Anti-CD20 Antibody binds B-cells and depletes B-cells through unclear mechanism(s) – Apoptosis, reticulo-endothelial system clearence, etc… Rituximab • (Rituximab) approved to deplete B-cell lymphomas • Phase I/II open label, dose-escalation study of 18 patients with non-threatening SLE • B-cell depletion correlated with improvement in rash, arthralgias, fatigue • Case reports of use in severe, refractory disease with some possible utility The Sun is Rising for Patients with Rheumatic Diseases: The Future is Bright