Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
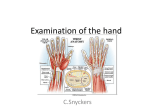
Biomechanics of the Wrist and Hand The wrist is the distal joint of the upper limb and allows the hand which is the effect segment, to assume the optimal position for prehension. Articular complex of the wrist The articular complex of the wrist contain two joints: 1. The radio-carpal joint between the radial head and the proximal row of carpal bones. 2. The mid-carpal joint between the proximal and distal rows of carpal bones. .(figure 1) Radio-carpal joint is an ellipsoidal joint and the carpal aspect presents two convexities transverse convexity and antero-posterior convexity.(figure 2) Figure 1. wrist joint Figure 2. Ellipsoidal joint The ligaments of the radio-carpal joint are the collateral ligaments (lateral and medial) and the anterior ligaments [attached to the anterior edge of the distal surface of the radius and neck of the capitates] and posterior ligament [forms a strap posteriorly]. Action of the ligaments: - During adduction-abduction the medial and lateral ligaments are active. Starting from the rest position . Adduction lateral ligament is stretched, medial slackened Abduction vice versa - During flexion-extension the anterior and posterior ligaments are most active. Flexion posterior ligament stretched Extension anterior ligament stretched Muscles of the wrist Motion Wrist flexion Wrist flexion Assists Wrist flexion Wrist extension Wrist extension Wrist extension Muscle Flexor Carpi Ulnaris Flexor Carpi Radialis Palmaris Longus Extensor Carpi Radialis Longus Extensor Carpi Radialis Brevis Extensor Carpi Ulnaris Wrist ulnar deviation Wrist ulnar deviation Wrist radial deviation Wrist radial deviation Flexor Carpi Ulnaris Extensor Carpi Ulnaris Flexor Carpi Radialis Extensor Carpi Radialis Longus Synergistic and stabilizing action of the muscle of the wrist: 1- Extensor muscles of the wrist act synergistically with the flexors of the fingers. E.g. during extension of the wrist the fingers are automatically flexes and, to extend the fingers in this position, a voluntary movement is required. 2- Flexor muscles of the wrist act synergistically with the extensors of the fingers. When the wrist is flexed, extension of the proximal phalanx follows automatically. Kinematics The articular complex of the wrist has basically two degree of freedom. When these compounded with pronation and supination, i. e. rotation of the forearm around its long axis, the hand can be oriented at any angle to grasp or hold an object. Movement of the wrist occur around two axes: - Transverse axis takes place in the sagittal plane with movement: Flexion the anterior palmar surface of the hand moves towards the anterior aspect of the forearm Extension the posterior dorsal surface of the hand moves towards the posterior aspect of the forearm. (figure 3) Figure 3.transfarce axis - Antero-posterior axis takes place in the frontal plane with movements: Adduction or ulnar deviation: the hand moves toward the axis of the body and its medial (ulnar) border forms an obtuse angle with the medial border of the forearm. Abduction or radial deviation: the hand moves away from the axis of the body and its lateral (radial) border forms an abtuse angle with the lateral border of the forearm. (figure 4) Figure 4. Anteroposterior axis. Range of movement of the wrist, range of abduction does not exceed 15 , of adduction is 45, of flexion is 85, and range of extension is also 85. Movement of circumduction [combination of the movement of flexion, extension, adduction and abduction] takes place in two axes of the wrist. The stabilization function of the ligament Stabilization in the frontal plane In the frontal plane, the ligaments are essential, because the distal surface of the radius faces distally and medially, so that as a whole it can be represented by a plane running obliquely proximo-distally and medio-laterally. Under the pull of longitudinal muscles, the carpus in the neutral position tends to slip proximally and medially.(Figure 5) figure 5. In neutral position When the wrist is adducted to approximately 30, the pull of the muscle now act perpendicular to the plane of the slippage, as a result the carpal bones are pushed back into the cavity and the carpus is stabilized. (figure 6) figure 6. In adduction When the wrist is abducted, the pull of the long muscles accentuates the instability and tends to displaced the carpal bones proximally and medially. (Figure 6) Figure 6. in abduction Stabilization in the sagittal plane In the sagittal plane roughly similar events take place. Because the distal surface of the radius points distally and interiorly (lateral view), the carpal bones tend to slid proximally and interiorly, i.e. in a plane parallel to that of the distal surface of the reduis.(figure 7) figure 7. In neutral When the wrist is flexed 30 to 40, the muscular pull tends to displace the carpal bones in a plane perpendicular to that of the distal surface of the reduis, thus repositioning and stabilizing these bones.(figure 8) figure 8. In flexion During extension, the tendency for the carpal bones to be displaced proximally and anteriorly is reinforced. (Figure 9) figure 9. In extension The full brunt is borne by the two redio-triquetral bands of the anterior and posterior ligaments of the radio-carpal joint. As they run obliquely proximally and laterally, they keep the carpal bone in position and prevent their medial displacement. (Figure 5) Abnormal Movement Anatomical damage is most often caused by abduction and extension often in combination. Abduction past the locked position caused two types of damage: - Fracture of the distal end of the radius: as the scaphoid is presses against the lateral buttress of the distal reduis - Fracture of the scaphoid : surprised in extention and allows its full length to hit the lateral buttress of the distal end of the radius. The radial styloid strikes the lateral surface of the scaphoid, which fractures as a result of shearing force. Extension , when exaggerated, most often causes a Colles’ fracture. More rarly it causes damage to ligaments with primary rupture of the lunato-capitate ligament and secondarily: - Perilunate dislocation : The lunate maintains its normal articulation with the radius, but the capitate articular surface is dislocated from the lunate, normally dorsally. - Anterior dislocation of the lunate: when the head of the capitates moves proximally towards the radius and displaces the lunate anteriorly into the carpal tunnel with compression of the median nerve. Another common injuries [wrist/ hand] Metacarpal (boxer’s) fracture and mallet or drop finger deformity resulting from injury at distal interphalangeal joints among foot ball receivers and baseball catchers. Forced abduction of the thumb leading to ulnar collateral ligament injury often results from wresting, football, hocky, and skiing. De Quervains disease (tendanitis of the extensor pollicis brevis and the abductor pollicis longus), common in golfers [ right handed tends to injury in left wrist] Carpal tunnel syndrome, carpal tunnel is a passage between the carpal bone and the flexor retineculum on the palmar side. Cause is unknown or from repeated forceful wrist flexion , usual onset is swelling caused by acute or chronic trauma leading to compress the median nerve. Symptoms like numbness along the median nerve, clumsiness of the figure function, and eventually weakness and atrophy of the muscles supplied by the median nerve. The Hand The hand of the man is remarkable instrument, capable of performing countless action, owing to its essential function: prehension. From the functional viewpoint the hand is effector organ of the upper limb, which supports it mechanically and allows it to adopt the optimal position for any given action. Functional position of the hand Wrist extended 20 degrees ulnarly deviated 10 degrees Digits 2 through 5 MP joints flexed 45degrees PIP joints flexed 30-45 degrees DIP joints flexed 10-20 degrees Thumb first CMC joint partially abducted and opposed MP joint flexed 10 degrees IP joint flexed 5 degrees. (figure 10) Figure 10. Functional position Types of grasp Two types of grasp are differentiated according to the position and mobility of the thumb's CMC and MP joints. 1. POWER grasp (The adductor pollicis stabilizes an object against the palm; the hand's position is static.) cylindrical grip (fist grasp is a small diameter cylindrical grasp) spherical grip hook grip (MP extended with flattening of transverse arch; the person may or may include the thumb in this grasp) lateral prehension (this can be a power grip if the thumb is adducted, a precision grip if the thumb is abducted). 2. PRECISION (Muscles are active that abduct or oppose the thumb; the hand's position is dynamic.) palmar prehension (pulp to pulp), includes 'chuck' or tripod grips tip-to-tip (with FDP active to maintain DIP flex) lateral prehension (pad-to-side; key grip) Muscles of the Hand Muscle Action abductor digiti minimi (hand) abducts the 5th digit abductor pollicis brevis abducts thumb adductor pollicis adducts the thumb extensor pollicis brevis extends the thumb at the metacarpophalangeal joint flexor digiti minimi brevis (hand) flexes the carpometacarpal and metacarpophalangeal joints of the 5th digit flexor pollicis brevis flexes the carpometacarpal and metacarpophalangeal joints of the thumb flexor pollicis longus flexes the metacarpophalangeal and interphalangeal joints of the thumb interosseous, dorsal (hand) flex the metacarpophalangeal joint, extend the proximal and distal interphalangeal joints of digits 2-4, abduct digits 2-4 (abduction of digits in the hand is defined as movement away from the midline of the 3rd digit) interosseous, palmar flexes the metacarpophalangeal, extends proximal and distal interphalangeal joints and adducts digits 1, 2, 4, & 5 (adduction of the digits of the hand is in reference to the midline of the 3rd digit) lumbrical (hand) flex the metacarpophalangeal joints, extend the proximal and distal interphalangeal joints of digits 2-5 opponens digiti minimi opposes the 5th digit opponens pollicis opposes the thumb palmaris brevis draws the skin of the ulnar side of the hand toward the center of the palm Mechanism for finger flexion Range of motion in PIP joints is greater than 90, in MP 135, and DP is slightly less than 90. Plane of movement of the of flexion of the last four figure worth discussing. The index is flexed in a strictly saggital plane toward the base of the thenar eminence. The axes of the fingers during flexion all converge to a point corresponding to the ‘radial pulse’. This can only occur if the other fingers are flexed not in a saggital plane like the index, but increasingly oblique plane. The little finger shows maximal obliquity of its plane of flexion, the significance of this oblique lies in the fact that it allows the more medial fingers to oppose the thumb like the index. (figure 11) figure 11. Finger flexion Mechanism for finger extension We can extend the PIP and DIP joints without extending the MP joints. But we can't extend the PIP joint without extending the DIP joint at the same time. Flexing only the DIP joint without also flexing the PIP joint is difficult. Full (active or passive) flexion of the PIP joint prevents active extension of the DIP joint. Tendinous structures comprise the extensor mechanism: 1. The extensor digitorum comunis EDC tendon attaches by a tendinous slip to the proximal phalanx, through which it extends the MP joint. 2. The central tendon (or "slip") proceeds dorsally to attach to base of middle phalanx, where tension can extend the PIP joint. 3. The lateral bands proceed on either side of dorsal midline and rejoin before attaching to the distal phalanx. Tension in the lateral bands extends the DIP joint. 4. The extensor hood surrounds the MP joint laterally, medially, and dorsally, and receives tendinous fibers from the lumbricales and interossei. (figure 11) Figure12. Tendanitous structure Although the extensor mechanism's fibres are tendinous, and therefore incapable of producing active force, they still transmit force to their attachments. Force develops in the extensor mechanism in two ways: 1. Many of the hand's intrinsic muscles attach to the extensor mechanism. Activity in any of these muscles produces force that the extensor mechanism communicates to its distal attachments. 2. The extensor mechanism develops passive tension whenever it is elongated. Hand movements that passively elongate either the extensor mechanism or a structure that attaches to the extensor mechanism produce force in the extensor mechanism itself. The extensor mechanism's fibers have lines of application that are always dorsal to the lateral axes of the PIP and DIP joints. Therefore, 1. activity in the intrinsic muscles that attach to the extensor mechanism always produces DIP and PIP extension. 2. Passive flexion of the MP joint elongates the extensor mechanism and extends the PIP and DIP joints. The fibrous lines of application in the hood and lateral bands pass very near the MP joint's lateral axis. Whether these structures move the MP joint in the sagittal plane depends on whether the MP joint is already flexed or extended. in MP extension: Action in the extensor digitorum extends the MP joint, and also pulls the extensor mechanism (including the hood) proximally. In this position, the interosseous muscles' lines of application are very close to the MP joint's lateral axis. With such small moment arms, these muscles have little effect on MP joint movement in the sagittal plane. However, they still produce MP abduction/adduction when the MP joint is extended The Thumb The thumb plays a unique role in the function of the hand. Thumb movement include extension (position of reference), flexion, adduction, abduction and opposition. It has five degree of freedom, three for coincidence of the point of contact, and two for full coincidence of the planes of the pulps. Opposition is the essential movement of the thumb and brings the pulp of the thumb into contact with that of any finger, made of three components: anteposition, flexion and pronation of the oseoarticular column of the thumb. Stability of the metacarpophalengeal joint of the thumb depends not only on the articular surface but also on its muscular cuff. Abnormal position of the hand and fingers These can result from either underactivity or overactivity of the muscles described. The following condition cause abnormal position of the fingers: a) Tearing of the extensor expansion b) Rupture of the extensor tendon just proximal to its insertion into 3rd phalanx. c) Rupture of the extensor tendon just proximal to metacarophalengeal joint. d) Rupture or paralysis of flexor digitorum sublimis . e) Rupture or paralysis of flexor digitorum profundus tendon. f) Paralysis of the interossei. Other abnormal deformeties Dupuytern’s contracture [shortening of the pretendinous fibers of the central palmar aponeurosis, the finger are irreducibly flexed] Volkmann’s contracture [ ischaemic contracture of the flexor muscles, finger assume hook-like position] Massive ulnar drift [ fingers markedly deviated medially, mainly seen in rheumatoid arthritis] CLINICAL APPEARANCE OF PERIPHERAL NERVE INJURIES IN THE HAND 1. Median: Often due to carpal tunnel sd. Wasting of thenar eminence. Decreased thumb function, especially opposition. Thumb moves into plane of palm. 2. Ulnar: Damage to ulnar nerve can occur with trauma to elbow region. Ulnar neuropathy is a frequent complication of diabetes mellitus Wasting of web space and interosseous spaces. Affects strength of intrinsic muscles of hand, so person can't hold a piece of paper between extended but adducted fingers Affects adductor pollicis and ulnar head of FPB. A person who lacks strength in these muscles cannot grasp with the thumb unless he or she flexes the IP joint by substituting with the flexor pollicis longus. Paralysis of the ulnar nerve produces “claw hand” 3. Radial: Associated with gunshot or stab wounds, fracture of humerus, "Saturday night palsy." person demonstrates a "dropped wrist," and cannot reposition thumb. lack of wrist extension may cause hand grip to be weak. Reference Kapandji, I A. (1982). The Physiology of the Joints. New York: Churchill Livingstone.