Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Photoreceptor cell wikipedia , lookup
Fundus photography wikipedia , lookup
Eyeglass prescription wikipedia , lookup
Keratoconus wikipedia , lookup
Visual impairment wikipedia , lookup
Dry eye syndrome wikipedia , lookup
Idiopathic intracranial hypertension wikipedia , lookup
Macular degeneration wikipedia , lookup
Vision therapy wikipedia , lookup
Retinal waves wikipedia , lookup
Corneal transplantation wikipedia , lookup
Blast-related ocular trauma wikipedia , lookup
Mitochondrial optic neuropathies wikipedia , lookup
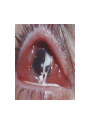
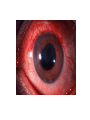
The Eye Ocular Pursuit “Eye wanna win” but “There is no eye in team” History • Trauma – Consider unrecognized trauma- awoke with symptoms • • • • • • Pain? Itch? FB sensation? Visual acuity changes, halos Contact lenses- ? Overwear Sick contacts/Viral symptoms Prior surgery or eye disorders Systemic disease Eye exam (the basics. From a non-ophthalmologist who isn’t particularly good at examining eyes.) if you can read this last line I’ll eat my shoe right here and now. Eye exam • • • • • • • • • • • Visual acuity Visual fields Pupil shape and reactivity Lid closure Foreign bodies Ciliary flare Foggy cornea (edema) Corneal infiltrate Fluorescein- corneal defects, Sidel’s sign Anterior chamber cells Intraocular pressure Visual Acuity • • • • Snellen Chart Use corrective lenses (or pinhole) Examine each eye separately If can’t read largest letter, go to finger counting • If can’t count fingers, check motion perception • If no motion perception, go to light perception Abbreviations which will impress your chart reader • OS – Left eye • OD – Right eye • OU – Both eyes • VA – Visual acuity Ocular Pursuit Question #2 • What does the latin abbreviation OS stand for? More Abbreviations • • • • • • • • • • L/L/L – Lids, lashes, lacrimal C/S – Conjunctiva and Sclera K – Cornea AC – Anterior Chamber I – Iris L – Lense AV – Anterior Vitreous CF – Count Fingers HM – Hand motion LP – Light perception Match the nerve with the extraocular muscle! • Extraocular Muscle • Cranial Nerve • • • • • • • VI Superior Oblique Superior Rectus Lateral Rectus Medial Rectus Inferior rectus Inferior oblique • III • IV Pupillary Reactions • Patient looks in the distance • Hold light in front of eye #1 for 3-5 seconds, then swing to the other eye • Should get initial constriction, then dilation Anterior – posterior • Lids, lashes • Conjunctiva, sclera, cornea • Evert eyelids • Anterior chamber • Retina Intraocular Pressure Measurement • Tonopen – need to calibrate first • Normal measurements 10 – 21 mmHg Approach to Ophthalmic Emergencies • Diagnostic Category – trauma, vascular, infectious, inflammatory, chemical exposure • Location - extraocular and periorbital, conjunctiva, sclera, cornea, anterior chamber, lens, posterior chamber, retina, vascular • Symptom Symptom approach • • • • • • 1. Vision loss Painless Painful 2. Eye pain 3. Red eye and discharge 4. Double vision Painless Vision Loss • • • • • • Retinal Detachment Central Retinal Artery Occlusion Central Retinal Vein Occlusion Vitreous hemorrhage Occipital lobe TIA/CVA Toxins (Methanol) Central Retinal Artery Occlusion • Anatomy • Internal Carotid Artery – – Ophthalmic Artery » Central Retinal Artery CRAO History • Sudden, painless, monocular blindness • Most of the visual field - worse in the central visual field Causes • Emboli – most common • Vasculitidies (temporal arteritis) • Trauma EMERGENCY!!! Yes. True. But… • Loss of vision may be irreversible within 90 minutes. Needs emergent ophthalmology referral. • Unfortunately… not much evidence for any therapeutic interventions. Studies tend to be small, not one center, without significant change in long term vision. Therapies (you can try) • Hemodilution – bolus 1-2 liters of normal saline • Ocular massage – closed lids – 10 -15 seconds – sudden release of pressure • Rebreathing CO2 – paper bag strategy • Intra-arterial thrombolysis • Anterior Chamber paracentesis – tetracaine – 30 guage needle – aspirate 0.1 ml. Bottom line… • Call the opthalmologist immediately if you suspect this diagnosis. • Post CRAO immediate window – treat like TIA – need to look at risk factors (HTN, dyslipidemia, diabetes, smoking), carotid doppler U/S, look for Atrial fibrillation. Central Retinal Vein Occlusion • Again, sudden, painless, monocular vision loss • More common than CRAO (CRVO prevalence ~ 1%, compared to ~ 1/10000 for CRAO) • Ischemic and non-ischemic variants Central Retinal Vein Occlusion Branch Retinal Vein Occlusion More treatments that may (or may not) be helpful • Aspirin • Intravitreal t-PA • Surgical options • Treat underlying disease Which of the following ocular problems is most commonly associated with a patient report of “curtain-like” vision loss? • • • • A. Vitreous hemorrhage B. Retinal detachment C. Optic neuritis D. Central retinal artery occlusion Retinal Detachment Retinal Detachment • Acute or subacute monocular vision loss • Floaters • Peripheral vision loss • Patients might describe “curtain like” visual loss Retinal Detachment • • • • • • • • • • • Occurs in 1/300 over the course of a lifetime Risk factors: Age Previous cataract surgery Focal retinal atrophy Myopia Trauma Diabetic retinopathy, Family history of retinal detachment Uveitis Prematurity If you suspect it… • Immediate ophthalmology consultation • Surgical options • Laser treatment of tears – Vitreous Hemorrhage • History – painless, monocular vision loss • Patients may describe “haze”, “smoke”, “streaks” Vitreous Hemorrhage • Causes: • Diabetic retinopathy • Posterior vitreous detachment • Trauma (shaken baby) Vitreous Hemorrhage • Consult ophthalmology: • Will look for any retinal tears which could be mended • Coag studies • Avoid exertional activities which could increase IOP Doctor… • My eye hurts! • And I can’t see out of it! Optic Neuritis Physical exam • Pain with eye movements • Afferent pupillary defect • May see optic disc swelling on fundoscopy Optic Neuritis • Inflammatory demyelination of the optic nerve • Most common in 20-40 year old women • Association with multiple sclerosis Imaging • MRI: • Optic nerve inflammation • Periventricular white matter lesions somewhat predictive of MS Treatment • Generally improves spontaneously over days – weeks • ?Steroids – may decrease progression to MS – talk to Neurology Which of the following is one of the diagnostic criteria for temporal arteritis? • • • • A. Bounding temporal artery pulse B. Erythrocyte sedimentation rate of > 20 C. New headache D. Age > 70 Temporal Arteritis • Medium/large vessel vasculitis • Carotid artery branches • Disease of the elderly Physical Exam • Palpate – firm, tender temporal artery • Joint pain with movement • Visual acuity Diagnosis • Age > 50 • New Headache • Abnormalities of the temporal artery (tender, pulseless) • ESR > 50 • Positive biopsy • 3/5 positive findings give sensitivity of 93% and specificity of 91% Treatment • Consult Ophtho and/or Rheumatology • High dose steroids Amaurosis Fugax • Transient monocular vision loss (minutes) • TIA of the eye • Neurology consult Name the phenomenon demonstrated in this picture Cortical Blindness • Think about it in the patient with vision loss and the absence of eye pathology • Occipital lobe insults, vertebrobasilar infarcts • Usual stroke treatment Question – name 3 causes of this condition Lateral Canthotomy/Cantholysis • Procedure to decompress a compartment syndrome of the orbit Retro-orbital hematoma Primary Indications • Decreased visual acuity • Intraocular pressure > 40 mmHg • Proptosis Contraindication • Globe rupture The things you’ll need to do your very own lateral canthotomy/cantholysis • • • • • 1. Lidocaine with epinephrine 2. Syringe with 25-gauge needle 3. Hemostat or needle driver 4. Iris or suture scissors 5. Forceps Step 1 • Prep skin • Anaesthetize – lido with epi into lateral canthus Step 2 • Apply needle driver or hemostat from lateral canthus to bony orbit to devascularize the area for 30 – 90 seconds. Step 3 • Remove the hemostat and cut the demarcated area 1 – 2 cm laterally Step 4 • Use the forceps to pull down the lower eyelid until you can see the inferior lateral canthal tendon • Cut through it Step 5 • Reassess IOP • If still greater than 40 mmHg haven’t provided adequate pressure relief: • Expose the superior lateral canthus and cut this too. Congratulations! What is the mechanism of action for fomepizole (4-MP) in the treatment of acute methanol toxicity? • • • • • • • A. Active diuresis of methanol through the kidney B. Enhanced hepatic conversion of the toxic methanol molecule through CYP 450 3A C. Competitive elimination with bile D. Competitive inhibition of alcohol dehydrogenase E. Inhibits blood flow through affected organs by the angiotensin pathway Examination of a ruptured globe with fluorescein may demonstrate displacement of the fluorescein due to aqueous humor flow. This has been named the: • • • • A. Seidel test. B. Adie’s pupil. C. Gunn’s phenomenon. D. Hoover’s test. Intraocular pressures associated with acute angle glaucoma tend to be: • • • • A. > 7 mmHg. B. > 14 mmHg. C. > 21 mmHg. D. > 28 mmHg. Chemical burns to the eye are true ophthalmologic emergencies. Generally speaking, which class of chemicals typically causes more damage? • • • • A. Acids B. Bases C. No difference D. pH 7.4 What is the hallmark finding of vertebrobasilar syndrome? • • • • • A. Crossed neurologic deficits B. Unsteady gait C. Afferent pupilary defect D. Bitemporal hemianopsia E. “Cherry red” macula Name that Finding/Disease! Epidemic keratoconjunctivitis Nodular episcleritis Scleritis Acute Angle-Closure Glaucoma Acute angle closure glaucoma • Acute angle closure glaucoma has at least 2 of the following • symptoms: • • ocular pain • • nausea/vomiting • • history of intermittent blurring of vision with halos • And at least 3 of the following signs: • • IOP > 21 mmHg • • conjunctival injection • • corneal epithelial edema • • mid-dilated nonreactive pupil • • shallow chamber in the presence of occlusion References • Basic Ophthalmology – 7th edition. Cynthia Bradford. American Academy of Opthalmology. • Med Clin N Am 90 (2006) 305–328 • Emerg Med Clin N Am 26 (2008) 233–238 • Ophthal Plast Reconstr Surg. 1994 Jun;10(2):137-41. Efficacy of lateral canthotomy and cantholysis in orbital hemorrhage • CJEM 2002;4(1):49-52 • Cochrane Database Syst Rev. 2009 Jan 21;(1):CD001989. Interventions for acute non-arteritic central retinal artery occlusion. • Emergency Medicine Reports. Volume 29, Number 17. August 4, 2008.