Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
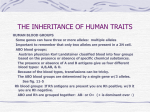
Name: RFLPs and Sickle Cell Anemia Background Information: Linda Fulcher and her husband Glenn were a bit nervous as they met with Beth Greendale, the genetic counselor at Children’s Hospital. The Fulchers, a young black couple from Miami, have been married for three years, and now they wanted to start a family. Like most young people, the Fulchers were healthy. They assumed that any children they might have would be healthy, too. But when they heard at their church about the screening program for sickle cell trait, they thought they should look into it. They found that about 1 in 625 black children in the United States are born with sickle cell anemia each year. When Beth Greendale gave her presentation to the church group as part of the screening program, she said that sickle cell anemia is caused by a problem with hemoglobin, the protein that carries oxygen in the blood. As a result of the abnormal hemoglobin, the blood cells take on a sickle shape, as shown in figure 1. As you can see, the cells are long and rigid, instead of round and flexible. People who have the disorder experience severe pain in their long bones and joints and are susceptible to infections. Some do not live beyond childhood. With good medical care, however, affected persons can live reasonably normal lives into adulthood. Sickle cell anemia, Beth said, is a co-dominant trait. That means affected individuals have two abnormal genes, one from each parent. Some people are said to be carriers and have the sickle trait. They have one normal allele and one affected but the trait. They have some sickle cells, but not enough to affect their lifestyle. Figure 1: Sickle and normal blood cells Question 1. If two people with the sickle trait reproduce, what is the probability that they will have a child with sickle cell anemia? Beth had explained that each major ethnic group seems to have one genetic disorder that occurs more frequently in that population. Blacks, who trace their ancestry to Africa, are at increased risk for sickle cell anemia. Linda and Glenn decided to have themselves tested for the sickle cell trait. When the results showed that they both had the sickle cell trait, they called Beth at the genetic counseling clinic at Children’s Hospital to talk about family planning. Beth told them that there is a very accurate prenatal test that can determine whether the developing fetus has sickle cell anemia, sickle trait, or normal hemoglobin. Linda and Glenn listened as Beth introduced them to RFLPs. Red blood cells are filled with a protein called hemoglobin. Hemoglobin carries oxygen to cells that are actively working. In the late 1940’s, Dr. Linus Pauling suggested that sickle cell anemia might be caused by an abnormality in hemoglobin. A person with sickle cell anemia has a low red blood count (anemia). Many years of research revealed that the DNA that codes for the hemoglobin molecule has a mutation in individuals who have sickle hemoglobin. The mutation changes one amino acid (glutamic acid) in normal hemoglobin to a different amino acid (valine) in sickle hemoglobin. That change gives the red blood cells a different shape, which causes the problems seen in affected individuals. Procedure: 1. Table 1 shows bases that are part of the DNA sequence for normal hemoglobin and sickle hemoglobin. Complete the table, by using the codon table from your text book (included as table 2). DNA Normal hemoglobin DNA GGT CTC CTC Sickle hemoglobin GGT CAC CTC Table 1: Hemoglobin proteins Table 2: Codons in mRNA MRNA codons Proteins Question 2. What are the differences in the genetic code and the result of that difference? 2. Strands A and B represent two single strands of DNA. Using the strips of paper, colour in each square according to the information below. Assign a colour to represent each of the four bases (adenine, thymine, cytosine, guanine). Include this key in your lab. Strand A AGGTCTCCTCTAATTGGTCTCCTTAGGTCTCCTTA Strand B AGGTCTCCTCTAATTGGTCACCTTAGGTCTCCTTA 3. The restriction enzyme MstII recognizes the DNA sequence GGTCTCC and cuts the DNA cut between the first T and the first C of that sequence, reading from left to right. Either mark the cuts on your paper strips or cut the strips at the proper spot(s). Glue the strips at the in the space on the last page (leave room to answer the question on that page!). Question 3: What will be the length of the fragments (haw many bases) if strand A is cut with MstII? What will be the length of the fragments in strand B? Question 4: How could you use MstII to distinguish between normal hemoglobin from sickle hemoglobin? Question 5: Assume that Ms. Fulcher undergoes prenatal testing. The genetic counselor shows Ms.Fulcher and her husband the results of the DNA test. In each case, give the diagnosis for the developing fetus a) fragment sizes = 4, 14, 10, 7 b) fragment sizes = 4, 14, 10, 24, 7 c) fragment sizes = 4, 24, 7 Question 6: Mutations among different ethnic groups are usually present due to their usefulness to a population. There is a very good reason why people of African descent are more likely to have the sickle trait or sickle cell anemia. Find out why and how this trait is beneficial. Strand A Strand B Strand A Strand B Strand A Strand B