Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
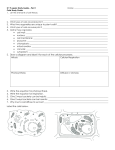
Understanding the “Dark Side” of the Knee: Imaging the Posterolateral Corner Imaging the Injured PLC: Magnetic Resonance Imaging Kirkland W. Davis, MD ; Jon A. Jacobson, MD ; Donna G. Blankenbaker, MD ; Ken L. Schreibman, MD, PhD ; Ben K. Graf, MD 1 2 1 1 3 (1) Department of Radiology, University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin (2) Department of Radiology, University of Michigan Medical School, Ann Arbor, Michigan (3) Department of Orthopedics and Rehabilitation, University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin ABSTRACT Anatomy Purpose: Injuries of the structures of the posterolateral corner (PLC) of the knee can have great significance. However, many radiologists have limited knowledge of the anatomy and clinical significance of the PLC. This poster will illuminate this poorly understood but important region. Many authors divide the major structures of the PLC into dynamic stabilizers and static stabilizers of the knee. The underlined structures below are the classically described components of the PLC and are demonstrated in accompanying figures. Content Organization: Topics reviewed in this poster will include: • Clinical features of PLC injuries, including mechanisms of injury and clinical relevance • Anatomy of the major and minor structures of the PLC • MR and ultrasound examples of the normal anatomy of the PLC • MR examples of PLC injuries • Examples of associated fractures visible on radiographs • Surgical and conservative treatment options Summary: The viewer will • Understand the significance of PLC injuries, including the increased risk of failure of cruciate ligament reconstructions • Know the gross, MR, and ultrasound anatomy of the PLC, including the major (fibular collateral, biceps, popliteus, gastrocnemius, popliteofibular, and capsule) and minor (fabellofibular and arcuate ligaments) components of the PLC • Recognize major injuries of the PLC • Be familiar with current treatment options for PLC injuries INTRODUCTION The posterolateral corner (PLC) of the knee has been called the “Dark side of the knee,” because of the difficulty in diagnosing injuries in this region. There are several important structures that comprise the PLC, and their injury can be important, whether these injuries occur in isolation or with other internal derangement of the knee. However, many radiologists have a limited understanding of the anatomy of this region and the imaging appearance of the normal and injured PLC. This presentation will review the anatomy of the PLC, clinical importance of injuries there, imaging of the normal and injured PLC, and treatment of PLC injuries. Figure 1a: Popliteus; Popliteofibular Ligament The popliteus muscle belly (triangular) and tendon are depicted in orange, with the tendon extending up to insert on the lateral femoral condyle, just inferior to the origin of the fibular collateral ligament. The popliteofibular ligament is depicted in brown, curving down to insert on the fibular styloid just medial to the conjoined tendon insertion. • Dynamic stabilizers: ÌÌ Popliteus muscle-tendon unit (see Figs. 1a, 2): constant àà Originates from posteromedial tibia àà Tendon passes through the popliteal hiatus of the posterior horn lateral meniscus àà Inserts onto sulcus on lateral surface of lateral femoral condyle ÌÌ Biceps femoris tendon (see Figs. 1b, 3): quite variable anatomy, but overall constantly present àà Long head joins conjoined tendon (both anterior and direct arms) àà Short head: ww Direct arm also joins the conjoined tendon ww Anterior arm inserts on superolateral tibia ÌÌ Lateral head of gastrocnemius muscle (see Figs. 1c, 4): constant àà Originates at supracondylar tubercle of distal femur àà Closely applied to joint capsule at PLC • Static stabilizers: ÌÌ Lateral collateral ligament (fibular collateral ligament—FCL; see Figs. 1b, 5): constant àà Originates on lateral margin of lateral femoral condyle àà Runs superficial to popliteus tendon àà Blends with biceps tendon conjoined tendon àà Inserts on lateral fibular head (occasionally with second limb inserting on tibia) ÌÌ Popliteofibular ligament (PFL; see Fig. 1a, 6): variably present (38-100%, depending on the surgical series, but most authors state it is essentially always present) àà Arises from popliteus tendon àà Inserts medial edge of fibula àà Also called the fibular origin of the popliteus muscle àà Stabilizes external rotation ÌÌ Fabellofibular ligament (FFL; see Figs. 1d, 7): variably present (20-87%) àà Originates at fabella or lateral margin of gastrocnemius àà Inserts on fibular styloid àà Thickening of distal edge of capsular arm of short head of biceps ÌÌ Arcuate ligament (AL; see Figs. 1e, 8): variably present (13-100%) àà Inserts on fibular styloid àà Triangular sheet of fibers àà Lateral limb attaches to post capsule/femur àà Medial limb blends with oblique popliteal ligament/capsule àà Important stabilizer of PLC ÌÌ Lateral capsular ligament (“mid-third” lateral capsular ligament) ÌÌ Posterolateral capsule • Popliteomeniscal fascicles • Posterior horn lateral meniscus • Lateral coronary ligament • Iliotibial band (included in PLC by some authors) Figure 1d: Fabellofibular Ligament When a fabella is present, the fabellofibular ligament, depicted in green, originates on the fabella and inserts on the fibular styloid near the insertion of the popliteofibular ligament. When no fabella is present, the ligament may still exist; the origin in this instance would be the lateral margin of the gastrocnemius muscle/tendon. Figure 1b: Biceps Femoris; Fibular Collateral Ligament The biceps femoris muscle belly (proximal) and tendon are depicted in yellow, with the tendon inserting on the fibular head as part of the conjoined tendon, just lateral to the fibular styloid. The fibular collateral ligament, depicted in pink, originates on the lateral femoral condyle above the popliteus insertion and forms the other half of the conjoined tendon. Figure 1c: Lateral Head of the Gastrocnemius The lateral head of the gastrocnemius muscle belly (distal) and tendon are depicted in blue. The origin is the supracondylar turbercle of the distal femur. The fabella, when present, is a sesamoid within the musculotedinous junction. Figure 2: Normal popliteus tendon Figure 5: Normal Fibular Collateral Ligament Fat-suppressed proton density coronal images demonstrate the normal popliteus muscle and tendon (ellipse, image (a)), tendon passing through the popliteal hiatus (arrow, image (b)), and tendon inserting on the lateral femoral condyle (arrow, image (c)) deep to the fibular collateral ligament. Sagittal proton density images show the popliteus muscle posterior to the lateral tibia (bracket, image (d)) and tendon passing through the popliteal hiatus (arrow, image (e)). Longitudinal grayscale ultrasound demonstrates a normal fibrillar architecture of the popliteus tendon in its mid portion (f) and distally (g). The left arrow on image (f) denotes loss of echoes due to anisotropy. (a) Coronal T1 image shows normal fibular collateral ligament (bracket) originating from the lateral femoral condyle above the popliteus groove and inserting onto the lateral aspect of the fibular head. With the biceps tendon, the FCL forms the conjoined tendon at their insertion. Longitudinal grayscale ultrasound images show normal (b) proximal and (c) distal fibular collateral ligament (arrows) originating from the lateral femoral condyle above the popliteus groove and inserting onto the lateral aspect of the fibular head. On image (b), note the intact popliteus insertion deep to the FCL. All structures from figures a-e combined in appropriate layers. (a, b) Sagittal proton density images demonstrate a normal arcuate ligament (arrows) extending from the from the fibular styloid superiorly along the posterior joint capsule. (c) Sagittal fat-suppressed T2 image in the same patient demonstrates no edema posterior to the capsule in the vicinity of the popliteal hiatus; when edema is present at that site, consider arcuate ligament tear. (d) Coronal T1 image demonstrates both limbs of the arcuate ligament (arrows). This ligament is seldom discernible on MRI. • Isolated injuries of PLC uncommon, but do occur (1/3-1/6 of all PLC injuries said to be isolated). • Mechanisms: ÌÌ Blow to anteromedial knee àà First injures arcuate ligament complex àà With further rotation PCL injured ÌÌ Hyperextension with or without contact ÌÌ Noncontact varus injury • Typically high-energy injuries, especially in football, soccer, motor vehicle vs. pedestrians, falls • PLC injuries commonly accompanied by ACL or PCL injuries • 10-15% have common peroneal nerve injuries. • Popliteus injuries have a high association with ACL tears. Imaging the Injured PLC: Radiographs • Usually normal • Lateral joint space widening • Fractures are uncommonly seen, but can be important clues: ÌÌ Fibular head avulsion fracture = “arcuate fracture/sign” (see Fig. 9) àà Small avulsion of styloid or medial fibular edema arcuate or popliteofibular ligament injury àà Larger avulsion or diffuse edema FCL/biceps injury àà Highly associated with PCL ruptures ÌÌ Avulsion of Gerdy’s tubercle ÌÌ Segond fracture (see Fig. 10) àà > 90% associated with ACL rupture àà Also can be sign of PLC injury ÌÌ Fracture of the anteromedial tibial rim (see Fig. 11) • Varus stress view wide joint space laterally (see Fig. 12) Coronal fat-suppressed proton density images demonstrate disruption of some of the fibers of the biceps (red arrow, image (a)), while others remain intact (arrow, image (b)), indicating partial tear. However, there is a complete tear of the fibular collateral ligament (blue arrow). 15a 2a FEM 2b TIB 5b 8b 5c Figure 6: Normal Popliteofibular Ligament (a) Coronal fat-suppressed proton density image demonstrates a normal popliteofibular ligament (arrow) extending from the from the popliteus musculotendinous junction and inserting onto the fibular styloid. (b) Sagittal fat-suppressed T2 image demonstrates the popliteofibular ligament near its insertion (arrow). (c) Coronal T1 image in a different patient depicts the popliteofibular ligament inserting on the fibular styloid (arrow). (d) Longitudinal grayscale ultrasound image demonstrates a normal popliteofibular ligament (arrows) extending from the from the popliteus musculotendinous junction and inserting onto the fibular styloid. 2d 2c LCL 8d 8c TIB Physical Exam Figure 9: Arcuate Sign • Especially in the acute setting, physical examination of the knee can be difficult and discerning all elements of instability is a challenge, even for skilled examiners. • Posterolateral instability may be misperceived as PCL instability alone. • Specific tests: ÌÌ Dial test (tibial external rotation): prone increased external rotation at 30° but not 90° isolated injury of PLC; increased external rotation at both angles both PLC and PCL injuries. Side-to-side difference of 10° or more suggestive of injury. ÌÌ Posterolateral drawer test ÌÌ Varus stress test at 0° and 30° ÌÌ Reverse pivot shift ÌÌ Assessment for varus thrust gait ÌÌ External rotation recurvatum test The structures of the PLC can also be discussed relative to their layers as follows: 2e 6a 6b TIB 2g FIB Figure 3: Normal Biceps Femoris Tendon 3a POP 6c Figure 16: Normal PFL • Superficial layer (I): ÌÌ Iliotibial band ÌÌ Biceps tendon • Middle layer (II): ÌÌ Retinaculum, patellofemoral ligament • Deep layer: ÌÌ Fibular collateral ligament ÌÌ Popliteus tendon ÌÌ Popliteofibular ligament ÌÌ Arcuate ligament ÌÌ Fabellofibular ligament Figure 13: Imaging the PLC 3b Clinical Significance 7a 7b 7c • The elements of the posterolateral corner function to: ÌÌ Prevent posterior translation of the tibia ÌÌ Prevent varus angulation of the knee ÌÌ Prevent external rotation of the tibia • In the setting of a cruciate ligament reconstruction, leaving posterolateral corner injuries untreated risks failure of the cruciate procedure. ÌÌ Anterior cruciate ligament (ACL) grafts rupture. ÌÌ Posterior cruciate ligament (PCL) grafts become lax. • FCL and deep ligament complex primarily responsible for preventing varus and external rotation of the tibia. • Posterolateral injuries may lead to posterolateral rotatory instability and gait abnormalities, even without the usual concomitant injuries to the cruciates and menisci. • When overlooked, PLC injuries may cause chronic instability and pain; osteoarthrosis may be the final result. • Early repair of torn PLC structures improves outcomes (see below). • Must have high index of suspicion clinically and radiologically 26b Figure 22: Fibular Collateral Ligament Tear Longitudinal grayscale ultrasound of the FCL demonstrates a normal fibrillar pattern in the distal fibers (arrow) but a focal disruption at its origin (ellipse) at the lateral femur, indicated by focal hypoechogenicity. Longitudinal grayscale ultrasound demonstrates no recognizable FCL, biceps tendon, or PFL. Instead, there is only an irregular hypoechoic region replacing them. The adjacent hyperechoic structures near the bones may be shredded ligament fibers. Figure 17: PLC Edema Suggests Injury Some authors recommend performing a coronal oblique proton density sequence, with images angled to parallel the popliteus tendon as it passes through the hiatus, as depicted by the red lines on the scout sagittal proton density image. However, most centers do not add this sequence to their routine knee MRI protocols. 17a (a) Axial fat-suppressed T2 image depicts the extensive edema surrounding the PLC (bracket), indicative of a significant injury to the region. (b) Fat-suppressed sagittal T2 image depicts a high grade tear of the gastrocnemius (arrow), while the coronal fatsuppressed proton density image (c) depicts complete tears of the FCL and popliteus tendon (arrows). Figure 10: Segond Fracture (a) AP radiograph demonstrates the classic Segond fracture (arrow). This is an avulsion of the lateral tibial rim at the attachment of the lateral capsular ligament. While these fractures are highly associated with anterior cruciate ligament ruptures and meniscal tears, injuries of the PLC are also common with this fracture. (b) Lateral radiograph shows a large effusion (arrow) in this patient with significant internal derangement. (c) Coronal fat-suppressed proton density image confirms the Segond fracture (arrow). (d) Sagittal fat-suppressed T2 image confirms the expected ACL rupture (arrow), with loss of continuity of fibers proximally, abnormal orientation of distal fibers, and extensive edema. (e) Coronal fat-suppressed proton density image shows the stump of the ruptured popliteus tendon (red arrow) and the wavy, torn fibular collateral ligament (blue arrow). (f) Coronal fat-suppressed proton density image depicts the torn popliteofibular ligament (arrow). 9b 9c Figure 11: Anteromedial Tibial Fracture (a) Lateral radiograph of the knee demonstrates fragments from an anteromedial tibial rim fracture (arrow) in this patient with multiple injuries including PLC injury. (b) Fat-suppressed axial T2 MR image shows the anteromedial tibial rim fracture (red arrow) and significant edema surrounding the posterolateral corner (blue arrow). (Images courtesy of D. Lee Bennett, MD, Iowa City, IA) (a) Sagittal fat-suppressed T2 image demonstrates ACL rupture (arrow), with the fibers following an abnormal course. (b) On the sagittal proton density image, there is a horizontal tear of the medial meniscus (arrow). (c) Coronal fat-suppressed proton density image demonstrates edema surrounding an otherwise intact popliteofibular ligament (arrow). Sagittal fat-suppressed T2 images demonstrate partial disruption of the popliteus muscle belly (arrow, image (d)) indicating a partial tear; and edema in the expected vicinity of the arcuate ligament (arrow, image (e)), suggesting injury to that structure. 17b Femur FIB Conclusion: Key Points 17c Figure 20: Fabellofibular Ligament Tear Figure 18: Arcuate Ligament Injury Fat-suppressed (a) sagittal and (b) axial T2 images in a patient with a flipped torn meniscus demonstrate prominent focal edema posterior to the joint capsule in the vicinity of the popliteal hiatus, which suggests arcuate ligament tear (arrows). 11b 11a 14b Severe knee injury. (a) Fat-suppressed sagittal T2 image demonstrates complete disruption of the fabellofibular ligament (arrow). (b) Fat-suppressed coronal proton density image demonstrates numerous injuries, including a high grade tear of the popliteus at its femoral attachment (arrow). Recommended articles in bold 18b (a) Fat-suppressed sagittal T2 image shows edema within and disorganization of ACL fibers (arrow), indicating rupture. (b) Fat-suppressed coronal proton density image shows complete disruption of the biceps tendon and FCL (ellipse). (a) AP radiograph of the knee performed without stress shows a wide lateral joint space (arrow). (b) Coronal fat-suppressed proton density image depicts severe disruption of the posterolateral corner (ellipse). Fat-suppressed coronal proton density images of multiple injuries of the posterolateral corner. There is a complete rupture of the FCL (red arrow) and a partial rupture of the biceps (blue arrow, image (a)), and a high grade partial tear of the popliteofibular ligament (arrow, image (b)), indicated by swelling and increased signal but not complete disruption of fibers. 1. Bahk MS, Cosgarea AJ. Physical Examination and Imaging of the Lateral Collateral Ligament and Posterolateral Corner of the Knee. Sports Med Arthrosc Rev 2006; 14:12-19. 2. Baker CL, Norwood LA, Hughston JC. Acute Combined Posterior Cruciate and Posterolateral Instability of the Knee. Am J Sports Med 1984; 12:204-208. 3. Bennett DL, George MJ, El-Khoury GY, et al. Anterior Rim Tibial Plateau Fractures and Posterolateral Corner Knee Injury. Emerg Radiol 2003; 10:76-83. 4. Bolog N, Hodler J. MR Imaging of the Posterolateral Corner of the Knee. Skeletal Radiol 2007; online published March, 2007. 5. Covey DC. Injuries of the Posterolateral Corner of the Knee. JBJS 2001; 83-A:106-118. 6. Davies H, Unwin A, Aichroth P. The Posterolateral corner of the Knee: Anatomy, Biomechanics and Management of Injuries. Injury 2004; 35:68-75. 7. De Maeseneer M, Shahabpour M, Vanderdood K, et al. Posterolateral Supporting Structures of the Knee: Findings on Anatomic Dissection, Anatomic Slices, and MR Images. Eur Radiol 2001; 11:2170-2177. 8. Diamantopoulos A, Tokis A, Tzurbakis M, et al. The Posterolateral Corner of the Knee: Evaluation Under Microsurgical Dissection. Arthroscopy 2005; 21:826-833. 9. Ellingson CI, Kurtz CA, Sekiya JK. Nonsurgical Management of Lateral Side Injuries of the Knee. Sports Med Arthrosc Rev 2006; 14:20-22. 10.Harish S, O’Donnell P, Connell D, et al. Imaging of the Posterolateral Corner of the Knee. Clin Radiol 2006; 61:457-466. 11.Huang GS, Yu JS, Munshi M, et al. Avulsion Fracture of the Head of the Fibula (the “Arcuate” Sign): MR Imaging Findings Predictive of Injuries to the Posterolateral Ligaments and Posterior Cruciate Ligament. AJR 2003; 180:381-387. 12.Juhng SK, Lee JK, Choi SS, et al. MR Evaluation of the “Arcuate” Sign of Posterolateral Knee Instability. AJR 2002; 178:583-588. 13.Kim YC, Chung IH, Yoo WK, et al. Anatomy and magnetic Resonance Imaging of the Posterolateral Structures of the Knee. Clin Anat 1997; 10:397-404. 14.LaPrade RF, Wentorf F. Diagnosis and Treatment of Posterolateral Knee Injuries. Clin Orthop Relat Research 2002; 402:110-121. 15.LaPrade RF, Gilbert TJ, Bollom TS, et al. The Magnetic Resonance Imaging Appearance of Individual Structures of the Posterolateral Knee. Am J Sports Med 2000; 28:191-199. 16.Lee J, Papkonstantinou O, Brookenthal KR, et al. Arcuate Sign of Posterolateral Knee Injuries: Anatomic, Radiographic, and MR Imaging Data Related to Patterns of Injury. Skeletal Radiol 2003; 32:619-627. 17.Malone WJ, Koulouris G. MRI of the Posterolateral Corner of the Knee: Normal Appearance and Patterns of Injury. Semin Musculoskel Radiol 2006; 10:220-228. 18.McGuire DA, Wolchok JC. Posterolateral Corner Reconstruction. Arthrosc 2003; 19:790-793. 19.Miller TT, Gladden P, Staron RB, et al. Posterolateral Stabilizers of the Knee: Anatomy and Injuries Assessed with MR Imaging. AJR 1997; 169:1641-1647. 20.Munshi M, Pretterklieber ML, Kwak S, et al. MR Imaging, MR Arthrography, and Specimen Correlation of the Posterolateral Corner of the Knee: An Anatomic Study. AJR 2003; 180:1095-1101. 21.Sekiya JK, Jacobson JA, Wojtys EM. Sonographic Imaging of the Posterolateral Structures of the Knee: Findings in Human Cadavers. Arthroscopy 2002; 18:872-881. 22.Stannard JP, Brown SL, Robinson JT, et al. Reconstruction of the Posterolateral Corner of the Knee. Arthrosc 2005; 21:1051-1059. 23.Theodorou DJ, Theodorou SJ, Fithian DC, et al. Posterolateral Complex Knee Injuries: Magnetic Resonance Imaging with Surgical Correlation. Acta Radiologica 2005; 3:297-305. 24.White LM, Miniaci A. Cruciate and Posterolateral Corner Injuries in the Athlete: Clinical and Magnetic Resonance Imaging Features. Sem Musculoskel Radiol 2004; 8:111-131. 25.Yoon KH, Bae DK, Ha JH, et al. Anatomic Reconstructive Surgery for Posterolateral Instability of the Knee. Arthrosc 2006; 22:159-165. 26.Yu JS, Salonen DC, Hodler J, et al. Posterolateral Aspect of the Knee: Improved MR Imaging with a Coronal Oblique Technique. Radiology 1996; 198:199-20 25b 10d 14d 14e 19a 10e 10f 25a Figure 21: Complex PLC Injury Figure 19: ACL Rupture and PLC Injury 10c 20a 20b 14c Figure 12: Lateral Joint Widening • Anterior medial tibial rim fractures should focus attention on the posterolateral corner. • Segond fractures and avulsions of the fibular head should also prompt a search for PLC injuries, as well as cruciate ligament tears. • Tears of the popliteus muscle-tendon unit are usually associated with tears of the anterior cruciate ligament. • Don’t overcall edema along the FCL. As with the MCL, edema by itself is common about the FCL with various knee abnormalities and is not diagnostic of a sprain. Longitudinal grayscale ultrasound (a) without stress and (b) with valgus stress demonstrate no recognizable FCL or popliteus. With valgus stress, the gap between the femur (“F”) and tibia (“T”) increases prominently, indicating instability of the posterolateral corner. m = meniscus. Selected References 18a 10b • Injury of the major structures of the PLC should be evident at MRI and ultrasound. • Individual assessment of the popliteofibular, fabellofibular, and arcuate ligaments is not always possible; nevertheless, abnormalities of these structures should be sought. • Physical exam, surgical findings, and clinical outcome will be the final determinants of the significance of radiologic findings suggesting PLC injury. • In the absence of other diagnoses, the patient with an injured knee who has edema about the posterolateral corner should raise suspicion of a PLC injury—this should be suggested to the referring clinician. • Focal edema at/posterior to the capsule just behind the region of the popliteal hiatus may be due to a tear of the arcuate ligament. Figure 25: PLC Instability 14a 10a 26d 26c TIB 6d (a, b) Coronal fat-suppressed proton density images demonstrate a normal fabellofibular ligament (arrows) extending from the from the fabella to the fibular styloid. (c) Coronal T1 image in a different patient depicts the fabellofibular ligament inserting on the fibular styloid (arrow). (a) AP radiograph of a recently dislocated knee with PLC injury in addition to other ligament injuries shows an anteromedial tibial rim fracture (arrow) and lateral joint space widening. (b) Coronal fat-suppressed proton density MR image confirms complete disruption of the posterolateral corner. (c) Lateral and (d) AP views of the knee after reconstruction of the fibular collateral ligament and popliteus tendon with an Achilles allograft. Note tunnels in both the femur and tibia as well as suture anchors and screw with washer for reattachment. 26a Coronal T1 image demonstrates the normal popliteofibular ligament curving down from the popliteus musculotendinous junction to insert on the fibular styloid (arrow). Figure 7: Normal Fabellofibular Ligament Sagittal proton density images demonstrate the origin of the lateral head of the gastrocnemius muscle (arrows). The medial portion of the origin (a) typically is more muscular, and the lateral aspect (b) is more tendinous. 4b FIB Figure 14: Complex Injury Including PLC TIB Figure 4: Normal Gastrocnemius 4a (a) AP radiograph demonstrates a minimally displaced fracture of the fibular head, sometimes referred to as the arcuate sign. This is somewhat of a misnomer, as the fracture is more often associated with avulsion of the attachment of the conjoined tendon and less commonly the arcuate ligament attachment. (b, c) Coronal fat-suppressed proton density images confirm the fracture at the insertion of the conjoined tendon, indicating this to be a significant posterolateral corner injury. There is extensive surrounding edema. The popliteofibular ligament also is involved (arrow) and if this patient has an arcuate ligament it would also be attached to the avulsed fragment. Anatomy: Layers TIB Longitudinal grayscale ultrasound demonstrates ill-defined, swollen, hypoechoic torn FCL and popliteus proximally (ellipse). Red arrow demarcates a markedly hypoechoic and irregular, torn proximal popliteofibular ligament, with the blue arrow demonstrating this structure to be more normal distally near its insertion on the fibula. 9a 2f FIB Figure 23: Popliteofibular Ligament Tear • Nonoperative: poor results in patients with grade 3 injuries (complete tears) of the major structures • Operative: ÌÌ Improved results if perform in first 3 weeks; after this, scar tissue develops, peroneal nerve injuries are more likely ÌÌ Fix cruciate injuries first. ÌÌ Direct repair of PLC structures with suture or suture anchors; or grafting with hamstring tendons, biceps tendon, iliotibial band, or allograft (see Fig. 26) ÌÌ Chronic injuries: controversial as to best approach àà Anatomic reconstruction àà Stabilizing (tightening) procedures—e.g. sling procedure àà Valgus tibial osteotomy may help as a start, unloading the PLC. ÌÌ Arthroscopy will not see the FCL, fabellofibular, arcuate, and popliteofibular ligaments, which are extracapsular. àà Clinical and radiological signs of PLC injuries needed to direct open repair. • Critical structures to repair are the FCL, popliteus tendon, and popliteofibular ligament. Figure 26: PLC Repair Figure 24: Complex Ligament Tear FEM (a) Coronal T1 image shows normal biceps femoris tendon (bracket) at its insertion on the fibula, lateral to the fibular styloid. The biceps inserts in concert with the fibular collateral ligament as the conjoined tendon. (b) Longitudinal grayscale ultrasound image shows normal biceps femoris tendon (arrows) extending to its insertion on the fibula (FIB), lateral to the fibular styloid. • Normal tendons and ligaments demonstrate a fibrillar, hyperechoic architecture. • Tendon and ligament injuries can be demonstrated with ultrasound (see Figs. 22-24): ÌÌ Strains and sprains may demonstrate hypoechoic fluid surrounding the tendon/ligament or focal hypoechoic areas within the structure. ÌÌ Partial tears demonstrate disruption of a portion of the fibers. ÌÌ Complete tears demonstrate loss of continuity of all fibers of the tendon or ligament. • Ultrasound allows the potential for showing dynamic gapping if stress is placed across the tendon/ligament (see Fig. 25). • These techniques require experience with musculoskeletal ultrasound and confidence in the anatomy. Treatment TIB POP 8a Imaging the Injured PLC: Ultrasound 15b FIB Arcuate Ligament Figure 1f Figure 8: Normal Arcuate Ligament 5a Figure 1e: The arcuate ligament, depicted in pink, originates on the fibula. The lateral limb extends superiorly and inserts onto the joint capsule/lateral femoral condyle. The medial limb passes obliquely in a superior and medial direction and inserts on the oblique popliteal ligament of Winslow and the joint capsule. Injuries • Yu et al. advocate using a coronal oblique sequence in the plane of the intra-articular popliteus tendon to facilitate detection of the finer PLC structures (see Fig. 13). • Grading of injuries: I: feathery edema around/within muscle, tendon, or ligament. This is a strain or sprain (see Fig 14). II: partial tear—edema with some continuous fibers. The ligament/tendon may be abnormally thin or thick (see Fig. 15). III: complete tear: these are the ones that need to be fixed (see Fig. 15, 20, 21). • PFL best seen on coronal images attaching to medial fibular styloid (see Fig. 16). • Extensive edema around the PLC is worrisome for injury to one or more of the PLC components. Even if no discrete tear is seen, PLC injury should be suggested (see Fig. 17). • Arcuate ligament: can’t be seen reliably: it’s quite thin and hugs the capsule. • Edema behind the capsule in the region of the popliteal hiatus: suggestive of arcuate ligament injury (see Fig. 18) • PCL, ACL, medial collateral ligament (MCL), and meniscal injuries are commonly associated with injuries of the posterolateral corner and should be sought (see Fig 19). Figure 15: Biceps and FCL Injuries 12a 12b 21a 19b 21b Corresponding Author: Kirkland Davis, MD University of Wisconsin—Madison E3/311 CSC 600 Highland Avenue Madison, WI 53792–3252 Ph: 608.265.4482 Fax: 608.263.0876 Email: [email protected]