Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
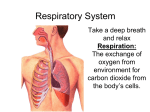
Physiology of breathyng. General functions of respiratory system The respiratory system comprises of the nose, mouth, throat, larynx, trachea, bronchi and lungs. The function of the respiratory system is to facilitate gaseous exchange to take place in the lungs and tissue cells of the body. Oxygen is required by cells in the body to allow various metabolic reactions to take place and to produce energy and is therefore essential to life. The respiratory system may be defined as the organs and tissues through which air is passed into and out of the body to allow the necessary gaseous exchanges to take place. Oral and nasal cavity Functions of air conductive pathway Lungs External and internal respiration External respiration is the means by which oxygen from the air passes into the blood stream for transportation to the tissue cells and carbon dioxide is collected and transferred back to the lungs and expelled from the body. Internal respiration involves the vital chemical activities which take place in every living cell requiring oxygen and glycogen to combine and release energy, water and carbon dioxide. The normal rate of inspiration and expiration, the respiration rate, is about 16 times a minute in an adult. Biomechanism of breathing Breathing is an active process - requiring the contraction of skeletal muscles. The primary muscles of respiration include the external intercostal muscles (located between the ribs) and the diaphragm (a sheet of muscle located between the thoracic & abdominal cavities). The external intercostals plus the diaphragm contract to bring about inspiration: Contraction of external intercostal muscles > elevation of ribs & sternum > increased front- to-back dimension of thoracic cavity > lowers air pressure in lungs > air moves into lungs Contraction of diaphragm > diaphragm moves downward > increases vertical dimension of thoracic cavity > lowers air pressure in lungs > air moves into lungs: To exhale: relaxation of external intercostal muscles & diaphragm > return of diaphragm, ribs, & sternum to resting position > restores thoracic cavity to preinspiratory volume > increases pressure in lungs > air is exhaled Effect of Rib and Sternum Movement on Thoracic Volume Effect of Rib and Diaphragm Movement on Thoracic Volume Pressure in lungs As the external intercostals & diaphragm contract, the lungs expand. The expansion of the lungs causes the pressure in the lungs (and alveoli) to become slightly negative relative to atmospheric pressure. As a result, air moves from an area of higher pressure (the air) to an area of lower pressure (our lungs & alveoli). During expiration, the respiration muscles relax & lung volume descreases. This causes pressure in the lungs (and alveoli) to become slight positive relative to atmospheric pressure. As a result, air leaves the lungs. Surface tension in lungs The walls of alveoli are coated with a thin film of water & this creates a potential problem. Water molecules, including those on the alveolar walls, are more attracted to each other than to air, and this attraction creates a force called surface tension. This surface tension increases as water molecules come closer together, which is what happens when we exhale & our alveoli become smaller (like air leaving a balloon). Potentially, surface tension could cause alveoli to collapse and, in addition, would make it more difficult to 're-expand' the alveoli (when you inhaled). Both of these would represent serious problems: if alveoli collapsed they'd contain no air & no oxygen to diffuse into the blood &, if 're-expansion' was more difficult, inhalation would be very, very difficult if not impossible. Fortunately, our alveoli do not collapse & inhalation is relatively easy because the lungs produce a substance called surfactant that reduces surface tension. Pressure in the lungs and intrapleural pressure Intrapleural pressure is always lower than the alveolar one: First: chest is a sealed container. Second, the lungs are characterized by elastic tension, which is due to these factors: 1. presence of ellastic fibers, which make 1 / 3 of elastic tention; 2. surface tension of the liquid layer on the inner surface of alveoli, which makes 2 / 3 of the elastic tension of the lungs. Thirdly, “negative” pressure in the pleural cavity is maintained by the large absorbtion capacity of pleural leaves. Spirometer, Lung Volumes, and Lung Capacities Spirometry Cardiopulmonary circulation Proprioreceptive control of breathing. Intercostal muscles, and diaphragm in a less extent, contain a large number of muscle fibers. Proprioreceptors become active during passive stretching of muscles, isometric contraction and the isolated contraction of intrafusal muscle bobbins. Receptors send signals to the corresponding segments of the spinal cord. Lack of contraction effort of inspiratory or expiratory muscles increases the impulsation from muscle bobbins, that increases gamma-motoneuron and then alphamotoneuron activity, in the means of dosing muscular effort. Receptors of the chest joints send impulses to the cerebral cortex. These impulses are the only source of information about the movements of the chest and respiratory volumes. Arterial chemoreceptors Location of the carotid and aortic bodies. Note that each carotid body is quite close to a carotid sinus, the major arterial baroreceptor. Both right and left common carotid bifurcations contain a carotid sinus and a carotid body. Summary of factors that stimulate ventilation during exercise