Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
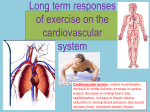
Chapter 13 INJURIES TO THE THORAX AND ABDOMEN Anatomy Review. The thorax and abdomen contain the majority of organs in the body. The area is enclosed by the spinal column, rib cage, and the clavicle, which provide bony protection. There are 12 thoracic vertebrae and 5 lumbar vertebrae located posterior to the abdomen. There are 12 pairs of ribs; the first 7 (sometimes 8) pairs connect directly to the spinal column and sternum and are called true ribs. Pairs 8 through 10 connect via a common coastal cartilage; pairs 11 and 12 do not connect directly to the sternum anteriorly, thus they are called floating ribs. All joints between the ribs and the spinal column are reinforced with ligaments. The area is further strengthened by the anterior longitudinal ligament. A. The major joints of the thorax include the intervertebral joints, the sternocostal and costochondral joints, and the sternoclavicular joints. The sternoclavicular joint is the only bony articulation between the thorax and the arm. B. The muscles of the area include internal and external intercostals, pectoralis major and minor, rectis abdominis, internal/external obliques, the trapezius, rhomboids, latissimus dorsi, and others. Refer to Time Out 13.1 for a list of the main muscles of the thorax and abdomen and their actions and innervations. C. Internal Organs. The two main organs in the thorax are heart and lungs. The heart is situated in an area called the mediastinum. The diaphragm separates the thoracic and abdominal cavities (refer to Figure 13.1 on page 197.) 1. The abdomen can be divided into four quadrants. The lower right contains the appendix and ascending colon; the upper right houses the liver, gallbladder, and right kidney; the upper left contains the stomach, spleen, left kidney, and pancreas; and the lower left houses the descending colon. I. Common Sports Injuries. Sports injuries to the thorax and abdomen are relatively uncommon in children and adolescents, but when they occur, injuries to this area can be very serious. A. External Injuries. 1. Fractures. An athlete may fracture a rib, the sternum, clavicle, or some part of a vertebra. Such injuries should be treated immediately to avoid life-threatening complications such as pneumothorax or hemothorax. In a sternal fracture, an airway obstruction is possible if the manubrium is dislocated and moves posteriorly. If the sternum and ribs separate completely, a flail chest can occur, along with pneumothorax or hemothorax. a. Rib fractures are common in sports. These fractures typically result when two or more players collide and the rib cage is compressed violently. Rib fractures can vary in severity. 1). Signs and symptoms include extreme localized pain that is aggravated by sneezing, coughing, forced inhalation, or sometimes movement. 2) The athlete may grasp the chest wall at the point of injury. 3) Mild swelling may occur at the site, and there may be bony deformity. 4) The athlete may complain of breathing difficulties and take rapid shallow breaths. 5) First aid care includes monitoring the athlete’s vital signs and watching for respiratory distress. 6) Arrange for transport to medical facility. b. The athlete may also experience subluxations and dislocations of thoracic skeletal joints. Costochondral separations involve disunion of the sternum and ribs. 1) Signs and symptoms include the athlete’s report that a snap or pop occurred. 2) A palpable defect may be felt and there may be swelling in the immediate area. 3) Maximum or near-maximum inhalation may be very difficult. 4) The athlete complains of pain and tenderness over the costochondral junction. 5) First aid care involves the immediate application of ice and light compression. Treat for shock if necessary. 6) Arrange for transport to medical facility. B. Breast Injuries. Women experience breast contusions from direct contact in some sports. Sports bras typically do not provide protection from direct contact, but they can provide breast support for women who choose to wear them. Women who don’t properly support their breasts during activity should be aware that stretching breast tissue eventually results in the loss of stability and the breasts’ natural contour. 1. Regardless of gender, nipple irritation caused by clothing that chafes the tissue can be reduced or eliminated by changing tops or wearing a bandage over the nipple during training and competition. C. Internal Injuries. It is not always easy to determine if an internal injury has occurred. 1. Heart Injuries. Sudden death among athletes is more often the result of an impact to the heart than any other factor. Although it is not a common occurrence, heart contusions can occur any time the heart is compressed between the sternum and spinal column by a violent external force such as being hit by a baseball or hockey puck. If the impact occurs when the contracting heart is in the repolarization phase, the athlete can experience ventricular fibrillation leading to death (commotio cordis). a. Use of an automated external defibrillator (AED) device is the most practical way to save the lives of people experiencing commotio cordis. This device is shown in Figure 13.3 on page 200. b. A blunt trauma to the chest can also cause aortic rupture, injure the pericardium or coronary arteries, or cause valvular damage. Aortic injury is often fatal and must be given immediate attention. 1) Closely observe any athlete with a chest injury for breathing problems, fainting, decreases in heart rate and blood pressure, and complaints of severe chest pains. c. Protective equipment is required in certain sports to prevent injury to the heart, lungs, and chest. Chest protectors are made of materials that are much better at attenuating the shock from a high velocity ball. d. For sports that do not require chest protection, the athletes should be trained in techniques that protect the chest during specific situations. e. Certified athletic trainers with CPR/AED training should be prepared to provide immediate care for an athlete with a significant chest injury. The athletic trainer should have an AED or an Emergency Action Plan available for this situation. 2. Lung Injuries. Athletes may experience pulmonary contusion as a complication of a rib fracture, contusion, or some other type of lung injury. a. A fractured rib can puncture the pleural sac, allowing air to enter the pleural cavity, which can cause a lung collapse (pneumothorax). 1) Spontaneous pneumothorax can occur without a preceding trauma; this condition has been reported among runners and weight lifters. b. Signs and symptoms of cardiac or pulmonary contusion and/or a pneumothorax include severe pain in the chest, sometimes radiating to the thoracic spine. 1) The athlete typically experiences breathing problems—either shortness of breath or painful breathing accompanied by short shallow breaths. The chest wall lacks movement during breathing. 2) The athlete may have a nonproductive cough and may have tachycardia. c. First aid care includes treating for shock, continuous monitoring of vital signs, and arranging for transport to a medical facility. 3. Liver. The liver is susceptible to blunt trauma, especially if the athlete has hepatitis or the organ is enlarged. However, the liver is fairly safe from sports injuries. 4. Kidneys. The kidneys are located on either side of the posterior abdomen and are susceptible to blunt trauma or extreme heat. An athlete who has experienced a hit in the lower back or exercised in the heat should be watched for blood in urine (hematuria) and referred to a physician. The athlete’s exercise regimen must often be modified until the urine is clear of blood. 5. Spleen. The spleen is susceptible to blunt trauma and internal disorders. An athlete who sustains a hard hit to the abdomen over the spleen can experience a lacerated spleen. Nevertheless, the organ can splint or patch itself after an injury, but if the patch is disrupted by even a small amount of trauma, the bleeding can resume and may result in death. a. An athlete who is hit hard in the upper left quadrant and later complains of pain in abdomen and/or left shoulder and upper third of the left arm (sometimes right shoulder) is exhibiting Kehr’s sign. The athlete must be referred to a physician immediately. b. Mononucleosis often causes spleen enlargement that makes the organ susceptible to injury during sports participation. An athlete who suffers from this infection needs to restrict his or her activity until a physician permits the athlete to resume participation. 6. Bladder. The bladder is not commonly injured in athletic competition. If the athlete receives a direct blow to the bladder resulting in an injury, the signs are pain in the area and possibly blood in the urine. Avoiding injury can be accomplished by emptying the bladder before practice or competition. 7. Abdominal Pain. Abdominal pain can occur before, during, and after competition. If an athlete experiences chronic pain in the same location, he or she should see a physician immediately. a. Abdominal pain is often referred pain. For example, an athlete who complains of chronic low back pain, may actually have a duodenal ulcer. b. Exercise-related transient abdominal pain (ETAP) is often called a “side ache.” Although the cause is unknown, the pain may be the result of ischemia in the diaphragm or an acute increase of venous return from the lower extremities to the liver. This increase in blood flow stretches the vein near the liver and causes a pain response to the brain. 1) Warming up before exercise can reduce the incidence of side ache. c. Appendicitis is another reason for abdominal pain. Any athlete who has generalized abdominal pain or very severe pain in the lower right quadrant, nausea, vomiting, and fever should be referred to a physician immediately. d. It is important to review each athlete’s medical history very closely to determine if a cardiac or respiratory problem may be exacerbated by athletic participation. e. Preexisting conditions may disqualify an athlete from participation in certain activities that stress the affected system. f. Conditions that may disqualify an athlete from competition include: hypertrophic cardiomyopathy (HCM), heart murmurs, cystic fibrosis, or chronic obstructive pulmonary disorder (COPD). REVIEW QUESTIONS 1. True or False: Men and women have the same number of ribs. Answer: True. There are 12 pairs of ribs in both males and females. Page: 196 2. Explain the difference between true ribs and floating ribs. Answer: The first 7 (sometimes 8) pairs of ribs are connected to the spinal column posteriorly and the sternum anteriorly; therefore, they are known as true ribs. Ribs 11 and 12 do not connect to the sternum anteriorly; thus they are called floating ribs. Page: 196 3. List the five main joints of the thorax. Answer: 1.) Intervertebral joints 2.) Vertebral and rib joints 3.) The sternocostal joints 4.) The costochondral joints 5.) The sternoclavicular joints Page: 196 4. With what necessary function do the intercostal muscles assist in the thorax? Answer: They function primarily to lift the rib cage and assist with breathing. Page: 196 5. True or False: Both lungs are the same size and configuration. Answer: False. The right lung has 3 lobes, and the left lung has 2, which makes the right one a little larger and heavier. Page: 193 6. What is the name of the enclosed space where each lung is located? Answer: Each lung is encased in a separate and closed space called the pleural sac. Page: 197 7. True or False: The diaphragm separates the heart and lungs from the abdominal viscera. Answer: True. The diaphragm separates the thoracic and abdominal cavities. Page: 197 8. Explain the difference between a pneumothorax and a hemothorax. Answer: A pneumothorax is the presence of air in the pleural cavity; a hemothorax is the presence of blood in the pleural cavity. Page: 200 9. List the signs and symptoms of a costochondral separation. Answer: 1.) The athlete will report that a pop or snap occurred. 2.) A palpable defect may be felt because deformity may or may not be present; in addition, there may be swelling in the immediate area. 3.) Maximum or near-maximum inhalation may be very difficult. 4.) Localized pain and tenderness over the area of the costochondral junction. Page: 198 10. What is the best indicator of kidney damage or disorder? Answer: Hematuria Page: 201 11. True or False: The spleen is able to splint itself if injured by blunt trauma. Answer: True. The spleen has the capacity to splint or patch itself at the site of the injury because of its reservoir of red blood cells. Page: 201 12. Name the infection, prevalent among college-aged students, that causes the spleen to enlarge, requiring athletes to reduce physical activity until the spleen is once again normal. Answer: Mononucleosis Page: 201 13. What is a major cause of damage to the liver among collegiate athletes? Answer: Trauma Page: 201 14. List four functions of the kidneys. Answer: Maintain proper levels of waste, gas, salt and water and other chemicals in the blood stream. Page: 201 15. When pain occurs in the abdomen, what are some of the locations that the abdominal pain can be referred to? Answer: Shoulder tip pain (referred from diaphragm); epigastric pain (referred from esophageal problems); low back pain (referred from stomach problems); pelvic area pain (referred from lower back pain). Page: 202 16. Explain the best way to prevent bladder injury among athletes. Answer: Avoiding injury to the bladder is best accomplished by emptying it before practice or competition. Page: 202 17. What are the two main organs in the thorax? Answer: The lungs and the heart Page: 197 18. What is the responsibility of the diaphragm? Answer: The diaphragm separates the thoracic and abdominal cavities. It is considered the main muscle of respiration. Page: 197 19. Define commotio cordis. Answer: When an athlete is hit in the chest and the impact is timed exactly with the repolarization phase of the contracting heart, it is possible for the athlete to experience ventricular fibrillation leading to death. Page: 199-200 20. List some of the preexisting conditions of the chest that may disqualify an athlete from participation. Answer: Hypertrophic cardiomyopathy, heart murmurs and arrhythmias, significantly decreased lung function from disease or disorder such as cystic fibrosis, or chronic obstructive pulmonary disease. Page: 202