Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
XXXX
XXXX
DOB: 03/22/YYYY
DOB: 06/07/YYYY
ZOFRAN CASE REVIEW - INSTRUCTIONS TO FOLLOW
General Instructions:
Brief Summary/Flow of Events:
In the beginning of the chronology, a Brief Summary/Flow of Events outlining the significant medical
events is provided which will give a general picture of the focus points in the case
Patient History:
Details related to the patient’s past history (medical, surgical, social and family history) present in the
medical records
Detailed Medical Chronology:
Information captured “as it is” in the medical records without alteration of the meaning. Type of
information capture (all details/zoom-out model and relevant details/zoom-in model) is as per the
demands of the case which will be elaborated under the ‘Specific Instructions’
Reviewer’s Comments:
Comments on contradicting information and misinterpretations in the medical records, illegible
handwritten notes, missing records, clarifications needed etc. are given in italics and red font color and
will appear as * Reviewer’s Comment
Illegible Dates: Illegible and missing dates are presented as “00/00/0000”(mm/dd/yyyy format)
Illegible Notes: Illegible handwritten notes are left as a blank space “_____” with a note as “Illegible
Notes” in the heading of the particular consultation/report.
Specific Instructions:
1. Ms. XXXX is a 30-year old female (mother of 2 female children) had consumed Zofran for
symptoms of nausea and vomiting during her prenatal period (First through third trimester).
Although we received all of her delivery records including that of first child, we have paid
comprehensive attention of summarization of the records after 09/25/YYYY (prenatal records for
second child starts from this date) in key medical events timeline that has the date of visit, medical
provider name, and reason for the consultation/hospital visit and related page reference and have
hyperlinked the indexed document page references so that the user can click and study the details
of the medical visits
2. For differentiation of records, we have captured the details of mother (Natalie XXXX) in blue
color font and baby (Sophia XXXX) in black color font to establish the cause effect relationship
3. Detailed attention has been paid for all events pertaining to the mother consuming Zofran, so as
to know its impact on the resultant complaints of the cardiovascular problems suffered by the
child.
4. Office visits / procedures impertinent to the Zofran case review have been combined and not
elaborated;
5. Missing records are indicated in the chronology.
6. Providers name which are illegible are captured as snapshot.
7. The PDF reference is given in dark red font when captured within Occurrence column
1 of 87
XXXX
XXXX
DOB: 03/22/YYYY
DOB: 06/07/YYYY
Case Report
Parameter
Name of the mother
who consumed
Zofran
Occurrence
Natalie XXXX
Name of the child
who suffered injury
Sophia XXXX
Evidence for Zofran
intake
Yes
Zofran Use Details
Reason for Use: Hyperemesis
Start Date: 10/14/YYYY
Duration:
Per Pharmacy Records: Not available
Per Medical Records: 10/14/YYYY-06/07/YYYY
BATES Ref
297065_rec fm
ABCHealth
Center 000002
XXXXS_2958
67_rec fm
UCD_00003
297066_rec fm
XYZ
Memorial-Dr.
XX, MD 000022
297066_rec fm
XYZ
Memorial-Dr.
XX, MD 000022,
000021,
000015,
000031
Stop Date: Not known
*Reviewer's comment: Per admission date (for labor) 06/07/YYYY, patient was on
Zofran, however the exact stop date is not known.
Dosage: 4 mg, every 6 hourly as needed
Total Exposure: Not known
Zofran intake
(First/second/third
trimester)
*Reviewer’s comment: Pharmacy records are not available for review to calculate
the total exposure of Zofran during pregnancy.
First through third trimester
Other medications
used for
vomiting/nausea
Emetrol
Drugs taken along
with Zofran
Over-the-counter Prenatal Vitamins (Vitamin B-complex)
Emetrol
2 of 87
297066_rec fm
XYZ
Memorial-Dr.
XX, MD 000022,
000021,
000015,
000031
297066_rec fm
XYZ
Memorial-Dr.
XX, MD 000022
297066_rec fm
XYZ
XXXX
XXXX
DOB: 03/22/YYYY
DOB: 06/07/YYYY
(Metoclopramide,
Doxylamine/Pyridox
ine)
Did the Mother
have any preexisting
conditions, allergies
or contraindications
to Zofran?
Whether the child
was diagnosed with
Adverse Events?
(Cleft palate, Cleft
lip, congenital heart
defects and other
cardiovascular
conditions)
Treatment/manage
ment
(Reconstructive
surgery). Any
complications
Macrobid
No
Yes – Dilated cardiomyopathy with congestive heart failure
Date of Diagnosis: 08/20/YYYY
Hospitalization for the adverse event: Yes
Length of Hospital Stay:
First Hospitalization: XYZ Memorial Hospital - 08/20/YYYY (1 day)
Second Hospitalization: Abc Medical Center – 08/20/YYYY-08/21/YYYY
(2 days)
Third Hospitalization: ABC Children's Hospital – 08/21/YYYY11/04/YYYY (76 days/2 months, 15 days)
Hospitalization #1: 08/20/YYYY: Hospitalized at XYZ Memorial Hospital ER for
acute respiratory distress and sepsis – Transported to Abc Medical Center on the
same day
Hospitalization #2: 08/20/YYYY-08/21/YYYY: Hospitalized at Abc Medical
Center Pediatric Intensive Care Unit for dilated cardiomyopathy and congestive
heart failure – Chest X-ray revealed cardiomegaly – Echocardiogram showed
dilatation - Received Xopenex, Decadron, Ceftriaxone and was placed on NonRebreather (NRB) mask with subsequent saturations of 100% - As her perfusion
remained poor and her respiratory status was worsening, she was intubated with a 3.5
un-cuffed Endotracheal Tube (ETT) with Fentanyl 5 mcg, Versed 0.4 mg, and
Rocuronium 5 mg
Pediatric Cardiology: Echocardiogram showed cardiomyopathy with
severely depressed left ventricular function - Given Dopamine, Epinephrine
and Milrinone – Consider calling Stanford for transport to Cardiac Transport
Clinic
Respiratory: Patient on Synchronized Intermittent Mandatory Ventilation
(SIMV) with Pressure Controlled (PC)
Gastrointestinal: Lactic acidosis – Right Internal Jugular (IJ) placed for
access – Status post Sodium Bicarbonate and Calcium Chloride – Given
Ranitidine
Renal: Poor urine output – Given Lasix
Transported to ABC for dilated cardiomyopathy
Hospitalization #3: 08/21/YYYY-11/04/YYYY: Hospitalized at ABC Children's
Hospital for dilated cardiomyopathy
Cardiovascular: Cardiac failure with compensated cardiogenic shock on
vasopressor support – Tachycardic - Chest X-ray revealed dilated
3 of 87
Memorial-Dr.
XX, MD 000023,
000022,
000015
297066_rec fm
XYZ
Memorial-Dr.
XX, MD 000188
XXXXS_2958
67_rec fm
UCD_00108,
00350, 00251,
XXXXS_2971
60_rec fm
ABC Children's
Hospital_0002
0-00023,
00030-00036
XXXXS_2958
67_rec fm
UCD_00350,
00256-00262,
00251-00252,
XXXXS_2971
60_rec fm
ABC Children's
Hospital_0128
3-01285,
00020-00023,
01392-01393,
01277-01282,
00079-00082,
XXXXS_2961
50_rec fm
Stanford
Hospitals &
Clinics_00012,
XXXXS_2971
60_rec fm
ABC Children's
Hospital_0007
5-00078,
00072-00074,
01351-01352,
00068-00071,
00063-00067,
XXXX
XXXX
DOB: 03/22/YYYY
DOB: 06/07/YYYY
cardiomegaly and bilateral pleural effusions – Echocardiogram revealed
Patent Foramen Ovale (PFO) versus small secundum Atrial Septal Defect
(ASD), severely dilated Left Ventricle (LV) and severely decreased LV
systolic function – Right ventricular endomyocardial biopsy revealed
hypertrophy and fibrosis compatible with Dilated Cardiomyopathy (DCM) Supported with Dopamine, Epinephrine and Milrinone – Received Packed
Red Blood Cells (PRBCs) on 09/26/YYYY with little improvement –
Reconstructive Surgery: On 10/05/YYYY, underwent orthotopic heart
transplantation and median sternotomy and cardiopulmonary bypass
for end-stage dilated cardiomyopathy – Pathology report of native heart
revealed end-stage dilated cardiomyopathy - Started on Extended Release
Basiliximab on Postoperative Day (POD) #1 - Repeat echocardiogram on
POD #2 showed a better filled Right Ventricle (RV) with good systolic
function - Evaluation of her Superior Vena Cava (SVC) showed turbulent
flow by color doppler and slight gradient at the anastomosis sight - There
was also clot noted around the Right Atrium (RA)/SVC - The clot might be
contributory to the elevated CVP by pressing on the RA Immunosuppression regimen includes Cyclosporine, CellCept, and
Prednisolone - Last echocardiogram on 10/28/YYYY was normal - Right
ventricle endomyocardial biopsy dated 10/29/YYYY revealed no evidence
of acute cellular rejection (Grade 0) - Started on Diltiazem 2.7 mg NG twice
daily for coronary artery protection and Amlodipine 0.6 mg daily for goal
systolic BPs 90-100, which she has maintained
Respiratory: Acute respiratory failure due to pulmonary edema from left
atrial hypertension - Remains intubated and mechanically ventilated on
moderate settings – Chest X-ray showed moderated cardiomegaly with
central pulmonary edema - Following extubation on 09/01/YYYY she had
progressive respiratory failure with tachycardia, agitation and deteriorating
cardiac output and so re-intubated without difficulty- Remains intubated
after heart transplantation
Gastrointestinal: None Per Oral (NPO) – Supported with Total Parenteral
Nutrition (TPN) - Started patient’s enteral feeds after heart transplantation
on POD # 2 initially Nasogastric (NG) but on POD # 4 after an emesis
advanced her tube to Naso-Jejunal (NJ) - Receives Xopenex nebulization
and nasal suction every 4th hourly and Chest Physiotherapy (CPT) every 6th
hourly - Occupational Therapy had been working with her for PC feeding
trials and oral stimulation
Renal: Mild renal insufficiency with cardiogenic shock that has been
normalized afterwards – On scheduled doses of Lasix
Neurology: Developed a dependence on opioids and Benzodiazepines Restarted on Morphine and Versed infusions after her failed extubation - On
09/28/YYYY her Methadone and Ativan was changed to alternating every 4
hour dosing with a decrease in her needed require - Has been transitioned
from continuous infusions of Morphine and Versed to enteral Methadone
and Ativan on 10/12/YYYY
Heme: Risk for thrombus formation due to her depressed LV function and
cavitation seen on Echocardiogram - Initially maintained on a prophylactic
Heparin infusion of 10 units/kg/hour and Aspirin (ASA) - On 09/19/YYYY
she was transitioned to prophylactic Lovenox
Infectious Disease (ID): Had fever with elevated WBC and C-Reactive
4 of 87
00059-00062,
00086-00087,
XXXXS_2961
50_rec fm
Stanford
Hospitals &
Clinics_0003300034,
XXXXS_2971
60_rec fm
ABC Children's
Hospital_0005
4-00058,
00050-00053,
00007-00010,
00003-00006,
00083-00085,
XXXXS_2961
50_rec fm
Stanford
Hospitals &
Clinics_0004400045,
XXXXS_2971
60_rec fm
ABC Children's
Hospital_0129
9-01300,
01295-01296,
00030-00036
XXXX
XXXX
Follow-up visits for
treatment/managem
ent of
injury/Additional
surgeries
DOB: 03/22/YYYY
DOB: 06/07/YYYY
Protein (CRP) following on 09/12/YYYY - Received a 3 day course of
Vancomycin and Zosyn – Status post heart transplant, she continues on
Valcyte, Bactrim, Voriconazole and Nystatin for prophylaxis against
opportunistic infection
Pediatric Otolaryngology: Status post heart transplant with prolonged
intubation and subsequent hoarseness and significant supraglottic edema on
examination, likely secondary to local trauma due to intubation and airway
manipulation - Proton Pump Inhibitor (PPI) for better reflux prophylaxis,
Decadron 1/2 mg/kg every 8 hourly for 24-48 hours at discretion of primary
team to decrease edema and racemic Epinephrine– On 10/28/YYYY,
underwent micro-direct laryngoscopy and bronchoscopy for supraglottic
edema and stridor – Underwent Physical Therapy (PT) and Occupational
Therapy (OT) for recurrent stridor secondary to subglottic stenosis
Discharged on 11/04/YYYY to home with Peripherally Inserted Central Catheter
(PICC) for weekly lab draws, NG feeds and supplies.
11/09/YYYY: Complains of slight cough and positional stridor – Tachycardic rate to
166 while calm – Lipitor 1 mg initiated to protect against graft coronary artery
disease
11/16/YYYY: Overall vague discomfort ongoing, worse in the mornings – Improved
with Tylenol – Echocardiogram revealed hyperdynamic LV systolic function, trivial
pulmonary valve stenosis and fractional shortening of 39% - Recommended to
consider EKG and Holter monitor
11/20/YYYY: Elevated heart rate of 162 - EKG revealed an sinus tachycardia –
Holter monitor was placed
11/23/YYYY: Occasional positional stridor – Echocardiogram revealed trace
tricuspid valve regurgitation – Holter monitor showed tachycardia throughout day –
Voriconazole discontinued
11/28/YYYY: Received CytoGam infusion – Cardiac biopsy showed no evidence of
allograft rejection – Heart rate of 135 while calm
12/28/YYYY: Tachycardic rate – Echocardiogram revealed qualitatively
hypertrophied LV with normal systolic function and fractional shortening of 55% Aspirin discontinued
02/01/YYYY-04/12/YYYY: Tachycardic rate - Echocardiogram revealed normal
ventricular function with no pericardial effusion
07/03/YYYY: No symptoms from a cardiovascular perspective – Echocardiogram
showed normal cardiac function – Cardiac biopsy showed grade 1A for mild acute
rejection
01/07/YYYY: Echocardiogram revealed trace to mild pulmonary valve insufficiency
and normal LV systolic function – Cardiac biopsy showed no evidence of acute
rejection
05/21/YYYY: Echocardiogram revealed trivial tricuspid valve regurgitation
inadequate to estimate RV systolic pressure, trace pulmonary valve insufficiency and
5 of 87
XXXX
XXXX
DOB: 03/22/YYYY
DOB: 06/07/YYYY
mild flow acceleration across the superior vena cava with a mean gradient of 4
mmHg - Cardiac biopsy showed no evidence of acute rejection
11/11/YYYY: Complains of diarrhea with fever - Echocardiogram revealed the
cardiac function to be in normal limits – Fractional shortening of 41%
BATES Ref: XXXXS_296150_296154_rec fm XXYY Valley Health CTR_0024000244, 00235-00239, 00232-00234, 00238-00239, 00221-00225, 00226-00231,
00200-00204, 00191-00194, 00125-00129, 00095-00098, 00087-00090, 0007800082
Condition of the
patient per last
available medical
record
Per last available Cardiology visit dated 10/06/YYYY; Patient is doing well status
post heart transplant – No signs or symptoms suggestive of allograft rejection - Has
quiet precordium with normal S1 and S2 and no murmurs – Breath sounds also
normal with no respiratory distress – Echocardiogram showed trace pulmonary valve
regurgitation – Decreased hemoglobin, hematocrit and Cyclosporine levels –
Recommended to increase Cyclosporine to 55 mg twice daily - Planned for cardiac
biopsy in 3 months
*Reviewer's comment: Cardiology visits after 10/06/YYYY are not available for
review to know further progress of the patient.
6 of 87
XXXXS_2961
50_296154_rec
fm XXYY
Valley Health
CTR_0015000155
XXXX
XXXX
DOB: 03/22/YYYY
DOB: 06/07/YYYY
Brief Summary/Flow of Events
Zofran Intake – Duration: 10/14/YYYY to 06/07/YYYY
09/25/YYYY-06/03/YYYY: Multiple prenatal visits for nausea and vomiting - Diagnosed with
hyperemesis - Prescribed Zofran 4 mg, Emetrol and Prenatal Vitamins – She was on Zofran from
10/14/YYYY to 06/07/YYYY
Hospitalization for Labor and Delivery of Sophia XXXX
06/07/YYYY-06/08/YYYY: Admitted for labor – Viable infant girl delivered via Normal
Spontaneous Vaginal Delivery (NSVD) on 06/07/YYYY – Postoperative had mild anemia of
blood loss – Discharged home on 06/08/YYYY with Vicodin, Docusate Sodium and prenatal
vitamins
Sophia XXXX’ Infant Physical Record –Well Child
06/23/YYYY-08/10/YYYY: Infant physical record shows well child – Normal heart without
abnormality
Emergency Hospitalization @ XYZ Memorial Hospital ER
Hospital #1: 08/20/YYYY: Hospitalized at XYZ Memorial Hospital ER for acute respiratory
distress and sepsis – Transported to Abc Medical Center on the same day
Case Transitioned to Abc Medical Center
Hospital #2: 08/20/YYYY-08/21/YYYY: Hospitalized at Abc Medical Center Pediatric
Intensive Care Unit for dilated cardiomyopathy and congestive heart failure – Echocardiogram
showed cardiomyopathy with severely depressed left ventricular function - Given Dopamine,
Epinephrine and Milrinone – On Synchronized Intermittent Mandatory Ventilation (SIMV) with
Pressure Controlled (PC) - Lactic acidosis – Right Internal Jugular (IJ) placed for access - Poor
urine output – Given Lasix- Transported to ABC for dilated cardiomyopathy
Third Extended Hospitalization for Over 2 Months @ ABC Children's Hospital
Hospital #3: 08/21/YYYY-11/04/YYYY: Hospitalized at ABC Children's Hospital for dilated
cardiomyopathy - Cardiac failure with compensated cardiogenic shock on vasopressor support –
Tachycardic - Chest X-ray revealed dilated cardiomegaly and bilateral pleural effusions –
Echocardiogram revealed Patent Foramen Ovale (PFO) versus small secundum Atrial Septal
Defect (ASD), severely dilated Left Ventricle (LV) and severely decreased LV systolic function –
Right ventricular endomyocardial biopsy revealed hypertrophy and fibrosis compatible with
Dilated Cardiomyopathy (DCM) - Supported with Dopamine, Epinephrine and Milrinone – Mild
renal insufficiency with cardiogenic shock that has been normalized - None Per Oral (NPO) –
Supported with Total Parenteral Nutrition (TPN) - Developed a dependence on opioids and
7 of 87
XXXX
XXXX
DOB: 03/22/YYYY
DOB: 06/07/YYYY
Benzodiazepines - Received Packed Red Blood Cells (PRBCs) on 09/26/YYYY with little
improvement – On 10/05/YYYY, underwent orthotopic heart transplantation and median
sternotomy and cardiopulmonary bypass for end-stage dilated cardiomyopathy – Pathology
report of native heart revealed end-stage dilated cardiomyopathy - Started on Extended Release
Basiliximab on Postoperative Day (POD) #1 - Repeat echocardiogram on POD #2 showed a
better filled Right Ventricle (RV) with good systolic function - Started patient’s enteral feeds
after heart transplantation on POD # 2 initially Nasogastric (NG) but on POD # 4 after an emesis
advanced her tube to Naso-Jejunal (NJ) - Evaluation of her Superior Vena Cava (SVC) showed
turbulent flow by color doppler and slight gradient at the anastomosis sight - There was also clot
noted around the Right Atrium (RA)/SVC - The clot might be contributory to the elevated CVP
by pressing on the RA - Immunosuppression regimen includes Cyclosporine, CellCept, and
Prednisolone - Last echocardiogram on 10/28/YYYY was normal - Underwent micro-direct
laryngoscopy and bronchoscopy for supraglottic edema and stridor - Right ventricle
endomyocardial biopsy dated 10/29/YYYY revealed no evidence of acute cellular rejection
(Grade 0) - Started on Diltiazem 2.7 mg NG twice daily for coronary artery protection and
Amlodipine 0.6 mg daily for goal systolic BPs 90-100, which she has maintained - Discharged on
11/04/YYYY to home with Peripherally Inserted Central Catheter (PICC) for weekly lab draws,
NG feeds and supplies
Multiple Follow-up Visits for Cardiac Problems
11/09/YYYY-10/06/YYYY: Multiple visits for positional stridor, tachycardic rate, vague
discomfort, CytoGam infusion, cardiac biopsy and diarrhea with fever - EKG revealed sinus
tachycardia – Holter monitor showed tachycardia throughout day – Echocardiogram dated
10/06/YYYY showed trace pulmonary valve regurgitation - Cardiac biopsy showed no evidence
of acute rejection
8 of 87
XXXX
XXXX
DOB: 03/22/YYYY
DOB: 06/07/YYYY
Missing Medical Record:
What Records
are Needed
Complete Set of
Pharmacy
Records
Is Record Missing
Confirmatory or
Probable?
Hospital/
Medical Provider
Date/Time
Period
Why we need the
records?
Unknown
10/14/YYY
Y06/07/YYY
Y
To substantiate the
intake of Zofran
Confirmatory
Hint/Clue that
records are
missing
Zofran use
mentioned in
medical records
Maternal History (BATES Ref: 297066_rec fm XYZ Memorial-Dr. XX, MD - 000188,
297065_rec fm ABCHealth Center - 000022, 000008)
Past Medical History: Persistent nausea and vomiting and back pain.
Surgical History: Intrauterine Device (IUD) placement.
Family History: Non-contributory.
Social History: Never a smoker.
Allergy: Septra.
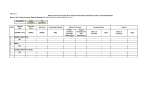
Detailed Chronology
DATE
PROVIDER
01/22/YYY Multiple
YProviders
05/07/YYY
Y
OCCURRENCE/TREATMENT
Preliminary Note: Mrs. Natalie XXXX is a 30-year old female with a significant
past medical history of persistent nausea and vomiting and back pain, consumed
Zofran for her nausea/vomiting symptoms during first and second pregnancies.
Upon review of medical records, we note the second child was diagnosed with
dilated cardiomyopathy suffering multiple related significant complications which
have been elaborated in the chronology and subsequently underwent orthotopic
heart transplant.
Prenatal Records of First Child
Multiple prenatal visit for morning sickness: (First Child)
@ 01/22/YYYY: Patient has had constant morning sickness. Took 2 prescriptions
of Zofran in first trimester, until last month. Tried on Vitamin B6 to date. Got
dehydrated enough to have a syncopal episode. Diagnosed with prolonged morning
sickness. Prescribed Vitamin B6 50 mg. (BATES Ref: 297066_rec fm XYZ
Memorial-Dr. XX, MD - 000080)
@ 02/20/YYYY: Patient felt weak, so mother advised her to take increased iron.
Morning sickness decreased. Baby active. Occasional dizziness. (BATES Ref:
297066_rec fm XYZ Memorial-Dr. XX, MD - 000079)
@ 03/27/YYYY: Patient noted severe pain in right flank this morning. (BATES Ref:
297066_rec fm XYZ Memorial-Dr. XX, MD - 000078)
9 of 87
BATES Ref
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
@ 05/07/YYYY: Patient has had occasional contractions. Increased pressure in
pelvis. (BATES Ref: 297066_rec fm XYZ Memorial-Dr. XX, MD - 000076)
BATES Ref
BATES Ref: 297066_rec fm XYZ Memorial-Dr. XX, MD - 000080, 000079, 000078,
000077, 000072, 000076
05/12/YYY XYZ
YMemorial
05/14/YYY Hospital
Y
*Reviewer's comment: Only significant details are elaborated from above visits.
Hospitalization records for delivery of First Child
Hospitalization for delivery:
@ 05/12/YYYY: Patient complains of uterine contractions every 4 minutes –
stronger and painful. (BATES Ref: 297066_rec fm XYZ Memorial-Dr. XX, MD 000068)
@ 05/13/YYYY: Vacuum assisted vaginal delivery under epidural anesthesia.
Delivered a normal female baby. (BATES Ref: 297066_rec fm XYZ Memorial-Dr.
XX, MD - 000101)
@ 05/14/YYYY: Patient is postpartum day #1. Discharged home with prescriptions
for Colace. (BATES Ref: 297066_rec fm XYZ Memorial-Dr. XX, MD - 000086)
BATES Ref: 297066_rec fm XYZ Memorial-Dr. XX, MD - 000068, 000070, 000083,
000088-00089, 000101, 000075, 000086
05/12/YYY XYZ
YMemorial
05/14/YYY Hospital
Y
Hospitalization records: Consent forms, acknowledgment form, laboratory
reports, patient education, orders, medical questionnaire, flow sheets, delivery
record, newborn identification, assessment, medical bills:
BATES Ref: 297066_rec fm XYZ Memorial-Dr. XX, MD - 000105-00106,
297066_rec fm XYZ Memorial-Dr. XX, MD - 000125-00128, 297066_rec fm XYZ
Memorial-Dr. XX, MD - 000131-00133, 297066_rec fm XYZ Memorial-Dr. XX, MD
- 000084-00085, 297066_rec fm XYZ Memorial-Dr. XX, MD - 000090-00102,
297066_rec fm XYZ Memorial-Dr. XX, MD - 000111-00113, 297066_rec fm XYZ
Memorial-Dr. XX, MD - 000123-00124, 297066_rec fm XYZ Memorial-Dr. XX, MD
- 000129-00130, 297066_rec fm XYZ Memorial-Dr. XX, MD - 000066-00067
01/24/2009
XYZ
Memorial
Hospital
Tom Xxxx,
M.D.
*Reviewer's comment: Hospitalization records have been combined and not
elaborated.
Emergency Room (ER) record for back pain and vomiting:
Patient who has a lengthy history of persistent nausea and vomiting and back pain.
She has had this ever since she was pregnant a couple of years ago. She has seen a
Gastroenterologist who placed her on Lexapro and Amitriptyline for irritable bowel.
Initially this seemed to work for the first six months, but over the past several
months she has been having recurring problems.
She has been having persistent vomiting for the past several days and worsening
mid to lower back pain. She believes the pain brings on the vomiting. She has been
treated with Norco with good success in the past through the pain, which has helped
10 of 87
297066_rec
fm XYZ
MemorialDr. XX, MD
- 000186,
297066_rec
fm XYZ
MemorialDr. XX, MD
- 00018800189,
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
the vomiting. She has been unable to keep any fluids down since yesterday and
presented today in marked distress. She has had some diarrhea as well.
Current medications: Lexapro 10 mg daily and Amitriptyline 10 mg daily. She did
have an Intra-Uterine Device (IUD) placed a few months ago and has had some
irregular bleeding, but it has not necessarily been associated with current problems.
She has had some lower pelvic pain, which she attributes to the IUD.
BATES Ref
297066_rec
fm XYZ
MemorialDr. XX, MD
- 00019000191
Physical examination:
Cardiac exam reveals a regular rate and rhythm without murmur or ectopy. She has
diffuse mid to lower paraspinous back pain. Abdomen is nondistended and soft and
diffusely tender, more so on the lower areas diffusely.
Assessment:
Recurrent nausea and vomiting associated with back pain, unknown
etiology
History of irritable bowel possibly related to above
09/25/YYY Multiple
YProviders
06/03/YYY
Y
Plan: Intravenous (IV) normal saline times 2 liters. Zofran 4 mg, Reglan 10 mg,
Pepcid 20 mg, and Ativan 1 mg IVP with resolution of nausea and vomiting. She
continued with pain. Morphine 4 mg IV pushed and given with good results and
pain decreased at 3/10. She is discharged with Compazine 25 mg every six hours as
needed for vomiting and Norco as needed for pain.
Prenatal Records of Second Child
*Reviewer's comment: From the below mentioned visits, elaborated details only on
Zofran intake details while other insignificant details are not elaborated.
Multiple prenatal visits for hyperemesis: (Second Child)
@ 09/25/YYYY: Patient had one positive pregnancy test at home. She has felt
fatigued and is mildly nauseated. She has had multiple abscesses in her groin area.
Diagnosed with pregnancy. Teratogens reviewed. Initiate prenatal vitamins.
(BATES Ref: 297066_rec fm XYZ Memorial-Dr. XX, MD - 000023)
@ 10/14/YYYY: Patient feels sick. She complains of hyperemesis. Similar problem
with first pregnancy. Unknown weight loss. Used Zofran throughout last pregnancy.
Last Menstrual Period (LMP): 09/03/YYYY. Assessment: Pregnancy, hyperemesis.
Plan: Prescribed Zofran 4 mg Orally Disintegrating Tablet (ODT). Suggested Over
The Counter (OTC) Vitamin B complex, Emetrol. Follow-up in 4 weeks. (BATES
Ref: 297066_rec fm XYZ Memorial-Dr. XX, MD - 000022)
*Reviewer's comment: Per the above visit dated 10/14/YYYY, we note patient was
prescribed with Zofran 4 mg. Hence, we consider this as start date of Zofran.
@ 11/10/YYYY: Patient has had problems with hyperemesis. She has been taking
Zofran daily. She tried Emetrol, which she drew up. She takes small sips of water
and small bites of food. She states overall that is improving. She has also been
constipated and I (Tom Xxxx, M.D.) suggested stool softeners and continue on
Metamucil and high fiber diet. Assessment: Intrauterine pregnancy at 10 weeks
gestation, hyperemesis. Plan: Continue Zofran, prenatal vitamins.
Addendum: Patient’s Aspartate Transaminase (AST) and Alanine Transaminase
11 of 87
297066_rec
fm XYZ
MemorialDr. XX, MD
- 000023,
000022,
000021,
000020,
000019,
000018,
000017,
000016,
297065_rec
fm
ABCHealth
Center 000029,
297066_rec
fm XYZ
MemorialDr. XX, MD
- 000015,
000014,
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
(ALT) levels mildly increased (Original lab reports not available for review). Will
follow. (BATES Ref: 297066_rec fm XYZ Memorial-Dr. XX, MD - 000021)
*Reviewer's comment: Per this visit dated 11/10/YYYY, patient was advised to
continue with Zofran.
@ 12/08/YYYY: Patient reports less nausea and vomiting. She is having some
problems with right inguinal recurrent abscesses and anxiety. Assessment:
Hyperemesis, hydradenitis. Plan: Follow-up in 4 weeks. (BATES Ref: 297066_rec
fm XYZ Memorial-Dr. XX, MD - 000020)
@ 01/05/YYYY: Patient has morning nausea and vomiting only. Assessment:
Hyperemesis improved. Plan: Continue on prenatal vitamins. Follow-up in 4 weeks.
(BATES Ref: 297066_rec fm XYZ Memorial-Dr. XX, MD - 000019)
@ 02/02/YYYY: Patient continues with significant nausea and vomiting daily.
Intermittently taking vitamins. Assessment: Hyperemesis. Follow-up in 4 weeks.
(BATES Ref: 297066_rec fm XYZ Memorial-Dr. XX, MD - 000018)
@ 03/10/YYYY: Patient reports less nausea and vomiting. Hyperemesis improving.
Follow-up in 4 weeks. (BATES Ref: 297066_rec fm XYZ Memorial-Dr. XX, MD 000017)
@ 04/06/YYYY: Patient complains of intermittent nausea and vomiting overall.
Improved taking prenatal vitamins. Follow-up in 2 weeks. (BATES Ref: 297066_rec
fm XYZ Memorial-Dr. XX, MD - 000016)
@ 04/19/YYYY: Patient complains of persistent nausea and vomiting with some
lower abdominal cramping yesterday. It is better today. She has had hyperemesis
throughout her pregnancy. She is not getting relief from fairly regular use of Zofran.
She thinks she may have bladder infection. Fetal heart tones are 148 with positive
fetal movements. Urinalysis reveals 10-20 White Blood Cells (WBCs) with bacteria
and few epithelial cells. Assessment: Intrauterine pregnancy 32 and 4/7 weeks’
gestation, hyperemesis and Urinary Tract Infection (UTI). Plan: Macrobid 100 mg
twice daily. May continue with Zofran. Follow-up in 2 weeks. (BATES Ref:
297066_rec fm XYZ Memorial-Dr. XX, MD - 000015)
*Reviewer's comment: Upon through review of follow-up visits from 12/08/YYYY
through 04/19/YYYY, although we note no mention about Zofran. However, per this
visit it has been mentioned as “May continue with Zofran”. Therefore, we assume
patient was on Zofran throughout this period for hyperemesis.
@ 05/06/YYYY: Patient is doing well. Less nausea and vomiting. Finished
Macrobid. Urinalysis negative for leukocytes. Follow-up in 1 week. (BATES Ref:
297066_rec fm XYZ Memorial-Dr. XX, MD - 000014)
@ 05/18/YYYY-06/03/YYYY: Doing well. (BATES Ref: 297066_rec fm XYZ
Memorial-Dr. XX, MD - 000013, 000012, 297065_rec fm ABCHealth Center 000028)
Hospitalization for Delivery of Second Child
12 of 87
BATES Ref
000013,
000007,
000012,
297065_rec
fm
ABCHealth
Center 000028
XXXX
XXXX
DATE
PROVIDER
06/07/YYY XYZ
YMemorial
06/08/YYY Hospital
Y
06/07/YYY XYZ
Y
Memorial
Hospital
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
*Reviewer's comment: Per the hospital admission record dated 06/07/YYYY, we
note Zofran listed under current medications list. Thereof which we establish that
patient had taken Zofran since 10/14/YYYY (first prescribed) through 06/07/YYYY
(Labor admission).
Hospitalization for delivery:
@ 06/07/YYYY: Patient admitted for labor. Current medications include Zofran 4
mg every 6 hourly as needed for nausea/vomiting and Prenatal Vitamins. She began
with strong uterine contractions at midnight increasing frequency and intensity.
Second stage controlled delivery – Viable infant girl delivered via Normal
Spontaneous Vaginal Delivery (NSVD). (BATES Ref: 297066_rec fm XYZ
Memorial-Dr. XX, MD - 000034, 000037, 000038)
@ 06/08/YYYY: Patient is doing very well with minimal pain and minimal
bleeding. Assessment: Status post NSVD, mild anemia of blood loss. Plan:
Discharge home with oral Vicodin, Docusate Sodium and prenatal vitamins.
(BATES Ref: 297066_rec fm XYZ Memorial-Dr. XX, MD - 000032, 000028)
Delivery Record:
Gravida
Para
SAB
Health problems
Pregnancy
Labor
Delivery
3rd Stage
Type
Male/Female
Weight
Length
Chest
HC
Mother Delivery Record
3
1
1
Hyperemesis, depression and hidradenitis
Normal
1st stage – 3 hours
2nd stage – 15 minutes
3rd stage – 5 minutes
Bow rupture – Spontaneous
Onset of labor – 06/07/YYYY @1200 AM
Date and Time 06/07/YYYY @ 0311 AM
Position at complete dilation – LOA
At Delivery – LOA
Estimated Blood Loss (EBL) – 100
Oxytocics Pitocin 10 UIM
Rotation – None
Delivery – Spontaneous
Anesthesia – None given
Date and Time – 06/07/YYYY @ 0316 AM
Placenta Delivery – Intact, spontaneous 3
vessels
Baby
Term
Female
6# 10 oz
18½
13
13
13 of 87
BATES Ref
297066_rec
fm XYZ
MemorialDr. XX, MD
- 000006,
000031,
000034,
000037,
000038,
000032,
000028
297066_rec
fm XYZ
MemorialDr. XX, MD
- 000038
XXXX
XXXX
DATE
PROVIDER
06/07/YYY XYZ
YMemorial
06/08/YYY Hospital
Y
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
1 minute – 8
Apgars
5 minutes – 9
Bulb
Resuscitation
Hospitalization records: Admission record, patient’s information, orders,
checklist, prescription records, Nursing plan of care, consent and acknowledgement
forms, medical bills, medication sheets, laboratory reports, postpartum flow sheets,
patient education:
BATES Ref
BATES Ref: 297066_rec fm XYZ Memorial-Dr. XX, MD - 000003-00006, 00002900031, 000039-00045, 000059-00062, 000036, 000046-00058, 000063
06/23/YYY Tom Xxxx,
Y
M.D.
*Reviewer's comment: Hospitalization records have been combined and not
elaborated.
Well Child Examination Report of Sophia XXXX
Infant physical record:
Birth weight: 6 lbs, 11 oz; Height: 18 inches.
Developmental: Startles, raises head, fixes eyes on face.
Physical examination:
Vital signs: Heart rate – 128; Respiratory rate - 40
Heart: Normal without abnormality.
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00184
Assessment: Well child.
08/10/YYY Tom Xxxx,
Y
M.D.
Plan: Follow-up at 2 months old.
Infant physical record:
History: Breast feeding.
Weight: 9 lbs, 10 oz; Height: 21.5 inches.
Physical examination:
Vital signs: Heart rate – 148; Respiratory rate - 44
Heart: Normal.
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00183
Assessment: Well child.
08/20/YYY XYZ
Y
Memorial
Hospital
Plan: Follow-up in 4 months old.
Emergency (ER) Admission @ XYZ Memorial Hospital For Acute Respiratory
Distress
Transport Report:
Diagnosis:
Acute respiratory distress
Sepsis
Transport vital signs:
14 of 87
XXXXS_29
5867_rec fm
UCD_00350
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Blood Pressure (BP) – 91/73; Pulse – 191; Respiratory rate – 78
BATES Ref
Name of referring Medical Facility: XYZ Medical Hospital Emergency Room
(ER)
Name of receiving Medical Facility: University of California (UC) Davis Medical
Center
08/20/YYY Abc Medical
Y
Center
Xx, R.N.
*Reviewer's comment: Per transport report, patient was transferred from XYZ
Medical Hospital ER, but the corresponding ER records are not available for
review to note the exact condition of the child when brought to ER.
Emergency Admission in Abc Medical Center for Dilated Cardiomyopathy
@ 04:05 PM: Nursing notes: (Illegible notes)
Referring Hospital: XYZ Memorial Hospital (Records from XYZ Memorial
Hospital are not available for review).
Receiving Hospital: Abc Medical Center Pediatric Intensive Care Unit (PICU)
XXXXS_29
5867_rec fm
UCD_00346
-00349
Xxx, R.N.
Patient presented to ER today with increased work of breathing, grunting. Received
immunizations 10 days ago and had fever for 3 days, recovered but continued to
have difficulty breathing, sick looking
Physical examination:
Cardiovascular: Pale, afebrile, mottled capillary refill 8 seconds, sinus
tachycardia. Brachial and femoral pulses weak.
Respiratory: Lungs with inspiratory wheezes.
Hospital medications: Xopenex, Decadron, Rocephin, Albuterol.
Impression: Acute respiratory distress.
08/20/YYY Abc Health
Y
System
Theresa
XXXXXX,
M.D.
Sophine
Xxxxx, M.D.
Transport: Patient transported to Pediatric Intensive Care Unit.
@ 04:30 PM: Pediatric Intensive Care Unit (ICU) admission for acute
respiratory distress:
Patient is a previously healthy 2 month old baby girl who presented to an Outside
Hospital (OSH) in respiratory distress and after an episode of apnea. 4 days Prior to
Arrival (PTA) she developed dry non-productive cough, worsening fussiness
mother thought was due to belly pain, and became pale. Father states she “hasn’t
been herself” and her symptoms worsened until the day of admission. Mother
thought her lungs sounds wet and that she sounded congested, but there was no
improvement with bulb suctioning of nose.
On the day PTA she had poor appetite, and on the day of admission she was not
interesting in eating at all. On the day of admission mother was holding patient
when the baby became pale and was not breathing. She turned her face-down and
patted her on the back to stimulate her to breathe. After some time (Sounds like <
30s) the baby took a labored breath, and then started having large emesis of curdled
milk and clear fluid. At that point they took her to the Emergency Department (ED).
She did have her 2 month vaccinations 10 days PTA and for about 3 days after she
15 of 87
XXXXS_29
5867_rec fm
UCD_00256
-00262,
XXXXS_29
5867_rec fm
UCD_00003
-00006
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
had temperatures of 100 (Ear thermometer), swollen legs at site of injections, and
fussiness.
At the OSH ED: She was found to be listless, in respiratory distress grunting with
retractions (Intercostal, subcostal, and sternal), tachypneic into 50s and tachycardic
into 170s. Initial labs were within normal limits, and rapid Respiratory Syncytial
Virus (RSV) was negative. Chest X-ray (CXR) was concerning for cardiomegaly.
She received Xopenex, oral Decadron, and Ceftriaxone (CTX) x 1 Intramuscularly
(IM), and was placed on Non-Rebreather (NRB) mask with subsequent saturations
of 100%. When our transport team arrived she was pale with capillary refill of 6-8
seconds and weak pulses in all four extremities, and with decreased breath sounds
and inspiratory wheezes. They obtained Intravenous (IV) access, and Venous Blood
Gas (VBG) at that time was pH 7.27 with base excess of 7, lactate 5.1.
She received racemic Epinephrine, and two Normal Saline (NS) boluses of 20
ml/kg with improvement in her capillary refill to 4-5 s, pulse of 178, Blood Pressure
(BP) of 86/61, and Respiratory Rate (RR) worsening into high 60s. 4 point BP was
within normal limits and equal. As her perfusion remained poor and her respiratory
status was worsening, she was intubated with a 3.5 un-cuffed Endotracheal Tube
(ETT) with Fentanyl 5 mcg, Versed 0.4 mg, and Rocuronium 5 mg. She was placed
on ventilation settings of Pressure Controlled (PC) ventilation: PC 25, Positive EndExpiratory Pressure (PEEP) 5, and rate of 30. VBG was drawn from a scalp IV with
a pH of 6.95 and base excess of 24, which was felt to be contaminant due to an
ionized calcium of 0.8 and Hb of 4.8 (Drastically different than previous labs). She
was started on Dopamine at 10 mcg/kg/min, given Sodium Bicarbonate (NaHCO3)
4 mEq, and calcium gluconate 100 mg/kg with improvement in pulse to 160 and
blood pressure of 100/83. At some point she received a 3rd NS bolus of 20 ml/kg.
Home medications: Tylenol as needed for discomfort.
Family history: Distant male family member with Myocardial Infarction (MI) at
age 30, death from cardiac causes at age 40. Mother, father and sister healthy.
Review of systems:
General: 1 week PTA, feeling poorly, not sleeping well, fatigued.
Ear, Nose and Throat (ENT): Congested
Cardiovascular: Unknown
Respiratory: Cough and trouble breathing
Gastrointestinal: Lost appetite and vomiting
Genitourinary: Decreased urine output
Heme: Pale
Physical examination:
General: Pale, sedated, intubated.
Head, Eyes, Ears, Nose and Throat (HEENT): Anterior fontanelle flan and
sunken.
Heart: Tachycardic in 180s, regular rhythm, no murmur, gallop most prominent
over apex of heart.
Lungs: Mechanical ventilation, clear to auscultation bilaterally.
Abdomen: Distended but compressible, liver edges down 3 cm, spleen not
16 of 87
BATES Ref
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
palpable.
Extremities: Cool, capillary refill 4-5 sec, no edema, central and distal pulses
intermittently palpable, and then weak, then absent.
Neuro: Sedated, moves all extremities, opens eyes spontaneously, normal tone.
Labs:
Hemoglobin – 10.4
Hematocrit – 31.6
Mean Corpuscular Volume – 89.1
Blood Urea Nitrogen (BUN) – 10
Creatinine – 0.5
Glucose – 155
AST – 69
ALT – 60
Alkaline Phosphatase (ALP) – 370
Chest X-ray: Shows cardiomegaly.
Echocardiogram: Shows diffuse dilatation.
Assessment: 2 month old female with an episode of apnea at home and worsening
fussiness, presenting in respiratory distress requiring intubation, here with possible
cardiomegaly, gallop on exam, and poor perfusion concerning for cardiac disease.
Patient’s presentation most concerning for underlying cardiac disease (Congenital
versus acquired) given her cardiac exam, concerning echocardiogram, signs of
Congestive Heart Failure (CHF), lack of fever and labs reassuring for infection, and
signs of end-organ damage from poor perfusion (Metabolic acidosis, high lactates,
poor urine output). Suspect myocarditis given diffuse dilatation of heart without
congenital anomalies, etiology is unclear.
Have spoken with Dr. Choy from Pediatric Cardiology who plans to review
echocardiogram remotely and will make recommendations. We may need to contact
Stanford to prepare for transport to Pediatric Heart Transplant Center. In the
meantime will continue patient on inotropic support, continue mechanical
ventilation, and follow gases to correct metabolic acidosis, as well as follow up
urine and ETT aspirate cultures and continuing Ceftriaxone.
Differential diagnosis: Respiratory etiology versus congenital cardiac disease
versus infection
Plan:
Cardiovascular:
Dopamine 12 mcg/kg/min, titrate to effect
Epinephrine at 0.5 mcg/kg/min, titrate to effect
Milrinone 0.5 mcg/kg/min
Pediatric Cardiology consult, aware of patient
Follow up final echocardiogram read
Consider calling Stanford for transport to Cardiac Transplant Unit
Unable to place art line due to weak/absent pulses
17 of 87
BATES Ref
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
08/20/YYY Abc Health
Y
System
OCCURRENCE/TREATMENT
Respiratory:
Ventilator: Synchronized Intermittent Mandatory Ventilation (SIMV) with
Pressure Controlled (PC): Rate 38, PC 20, PEEP 5
Upsized ETT to 3.5 micro-cuff, placement confirmed by chest X-ray
Arterial Blood Gases (ABG) lytes, Venous Blood Gases (VBG) lytes as
needed
End-Tidal (ET) Carbon-dioxide monitoring
Continuous pulse oximetry
Gastrointestinal: Lactic acidosis
Right Internal Jugular (IJ) placed for access, placement confirmed by CXR
D5 0.45 NS at 12 ml/hour
Lactic acid as needed
Status post Sodium Bicarbonate (NaHCO3), Calcium Chloride
Ranitidine 5 mg IV every 12 hrs
Infectious Disease:
Ceftriaxone 50 mg/kg IV q 24 hours
Follow up urine culture, respiratory culture
Heme: Stable
Renal: Poor urine output
Giving Lasix 1 mg/kg IV x 1, may need scheduled
Follow urine output closely
Foley in
Neuro:
Fentanyl 1-5 mcg/kg/hr, titrate for sedation
Versed 50-250 mcg/kg/hr, titrate for sedation
Vecuronium 0.1 mg/kg as needed for dangerous movement
X-ray of chest:
Indication: Dilated cardiomyopathy with very poor ejection fraction.
Rebecca
XXX-YYY,
M.D.
08/20/YYY University Of
Y
California
08/21/YYY Abc Health
Y
System
Impression: Cardiomegaly with mild congestive heart failure and small bilateral
pleural effusions.
@ 11:58 PM: EKG report:
Impression: Supraventricular tachycardia.
@ 01:12 AM: Endotracheal intubation procedure note:
Pre and postprocedure diagnosis: Respiratory distress
Theresa
XXXXXX,
M.D.
Procedure: Endotracheal intubation
Sedation and muscle relaxant: Vecuronium and Fentanyl.
Indication: Hypoxemia
Detailed procedure: Patient with 3.5 un-cuffed Endotracheal Tube (ETT) in place,
however unable to adequately ventilate due to large leak around tube. ETT changed
to 3.5 micro-cuffed without event. Cords visualized, bilateral Breath Sounds (BS),
18 of 87
BATES Ref
XXXXS_29
5867_rec fm
UCD_00108
XXXXS_29
5867_rec fm
UCD_00367
XXXXS_29
5867_rec fm
UCD_00255
-00256
XXXX
XXXX
DATE
PROVIDER
08/21/YYY Abc Health
Y
System
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
positive color change and post-procedure chest X-ray ordered.
@ 01:15 AM: Central venous catheter placement report:
Pre and postprocedure diagnosis: Respiratory distress
Theresa
XXXXXX,
M.D.
BATES Ref
XXXXS_29
5867_rec fm
UCD_00254
-00255
Procedure: Central venous catheter placement
Anesthesia: General anesthesia
08/21/YYY Abc Health
Y
System
Post-procedure chest X-ray read – central placement of Right Internal Jugular (RIJ)
tip.
X-ray of chest:
Indication: Dilated cardiomyopathy
Rebecca
XXX-YYY,
M.D.
08/21/YYY Abc Health
Y
System
Impression:
No significant change in congestive heart failure. Low endotracheal tube.
X-ray of chest:
Indication: Dilated cardiomyopathy
Rebecca
XXX-YYY,
M.D.
08/21/YYY University Of
Y
California
Impression:
Interval improvement in pulmonary edema and vascular congestion and
cardiomegaly persists.
Left lower lobe atelectasis
Improved endotracheal tube
@ 02:15 AM: Pediatric transthoracic echocardiogram report:
Indications: Congestive heart failure
Michael Choy,
M.D.
08/21/YYY Lora
Y
Knippers,
L.C.S.W.
08/20/YYY University Of
YCalifornia
08/21/YYY
Y
XXXXS_29
5867_rec fm
UCD_00104
XXXXS_29
5867_rec fm
UCD_00101
XXXXS_29
5867_rec fm
UCD_00368
-00369
Interpretation: LV fractional shortening is 8% and Simpson’s biplane ejection
fraction is 19%.
Summary: Dilated cardiomyopathy with severely depressed Left Ventricular (LV)
function.
@ 05:57 AM: Crisis Services Critical Care note:
Assessment: Parents just received news that their infant daughter may need a heart
transplant.
Plan: Social Services will be offered as needed. Will refer to Pediatric Social
Worker. Patient may be transferred to Stanford Children’s Hospital.
Hospitalization records: Orders, medication administration records, vitals record,
Nursing notes:
*Reviewer's comment: Hospitalization records have been combined and not
elaborated.
19 of 87
XXXXS_29
5867_rec fm
UCD_00252
-00253
XXXXS_29
5867_rec fm
UCD_00111
-00250,
0027100342,
00364-
XXXX
XXXX
DATE
PROVIDER
08/21/YYY University Of
Y
California
Heather
Xxxxxxx R.N.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
@ 08:13 AM: Nursing progress notes:
Assisted with transfer of patient. She is a 2 month old with dilated cardiomyopathy.
Patient intubated and vented. She is on multiple vasopressors and Fentanyl GTT for
sedation via Internal Jugular (IJ) in right neck. She is with foley to gravity. Patient
transported to Stanford, Lucile Packard. She is transferred at 08:11 AM via Isolette
on gurney.
BATES Ref
00366,
0035500359,
00363
XXXXS_29
5867_rec fm
UCD_00251
-00252,
XXXXS_29
5867_rec fm
UCD_00352
-00354
Transport summary:
Diagnosis: Dilated cardiomyopathy
Referring Hospital: Abc Medical Center
Receiving Hospital: Lucille Packard
08/21/YYY ABC
Y
Children's
Hospital
Seda Xxx,
M.D.
Assessment: Transferred to ABC for dilated cardiomyopathy.
Emergency Admission to ABC Children's Hospital For Dilated
Cardiomyopathy
@ 10:59 AM: Echocardiogram report:
Indication: Presumed myocarditis
Findings:
{S, D,S}, normal Atrioventricular (AV) and Ventriculo-Arterial (VA)
connections
Patent Foramen Ovale (PFO) versus small secundum Atrial Septal Defect
(ASD) with left to right flow
Mild to moderate tricuspid valve regurgitation
Mild to moderate mitral valve regurgitation
Mild aortic valve regurgitation
No left ventricular outflow tract obstruction
Mild to moderate pulmonary valve regurgitation
No pulmonary valve stenosis
Confluent branch pulmonary arteries without obstruction
Normal origins of left and right coronary arteries
Left aortic arch, unobstructed
Severely dilated Left Ventricle (LV) with severe dysfunction
Right Ventricle (RV) not seen well, but probably with moderate
dysfunction
No pericardial effusion
Summary:
Severely decreased left ventricular function
Severely dilated left ventricle
20 of 87
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
283-01285
XXXX
XXXX
DATE
PROVIDER
08/21/YYY ABC
Y
Children's
Hospital
Andrew
XXXXXXX,
M.D.
08/21/YYY ABC
Y
Children's
Hospital
Justin xxxx,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
*Reviewer's comment: Admission record for this hospitalization is not available for
review.
@ 11:53 AM: Pediatric EKG report:
Findings:
Right atrial enlargement
Right ventricular hypertrophy
Probable left ventricular hypertrophy with secondary repolarization
abnormality
Borderline prolonged QT interval (327 ms)
Interpretation: Abnormal ECG
@ 01:14 PM: Pediatric Cardiology consultation for presumed myocarditis:
Patient is a two-month-old little girl with no significant past medical history who
was in her usual state of good health until about 10 days ago when shortly after
receiving her two-month vaccination series she developed fever. According to her
parents, she had fever consistently for five days which was symptomatically treated
with Tylenol. Around Sunday or Monday, her fevers discontinued, however, she
clinically deteriorated. Her parents described her as grunty and fussy and not
feeding as well.
Yesterday morning, her mother noticed her to become pale and stopped breathing.
She turned her over performed a few back blows after which patient had a few
episodes of vomiting and then developed respiratory distress. She was taken to
XXYY Hospital in the Mount Shasta area and was subsequently transferred to UC
Davis. An echocardiogram was performed which showed severely decreased
ventricular function, and given her history of fever, she was presumptively
diagnosed with myocarditis. She was started on inotropic therapy and this morning
was transferred to ABC Children’s Hospital at Stanford for further diagnosis and
management.
According to her parents, she has otherwise been a healthy child. She is a product of
a term delivery with no complications except for hyperemesis gravidarum. Her
prenatal laboratory studies were unremarkable.
Review of systems:
General: Specifically positive for five days of fever following vaccinations,
followed by poor feeding and fussiness.
Gastrointestinal: Poor feeding. Negative for vomiting or diarrhea (Except for the
one episode of vomiting yesterday).
Respiratory: Respiratory difficulty.
Physical examination:
Height: 57 cm; Weight: 4 kg
Vital signs: Temperature 36 degrees Celsius. Heart rate 159 in sinus rhythm (On
inotrope). Respiratory rate 30 (On a ventilator). Blood pressure 66/54. Oxygen
saturation 100% on 100% FiO2.
21 of 87
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
293
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
020-00023
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
General: Sedated, paralyzed.
Heent: Normocephalic, atraumatic. Mouth moist and intubated.
Lungs: Clear to auscultation bilaterally, although breath sounds are diminished on
the left side. No wheezes or rales.
Cardiovascular: S1, S2. Positive S3, no S4. Regular rate and rhythm. No murmurs,
rubs. The precordium is overall non-hyperdynamic.
Extremities: Warm and reasonably well perfused. Capillary refill time two to three
seconds. Pulses are equal and strong in all four extremities.
Diagnostic studies:
Parameter
WBC
Hemoglobin
Hematocrit
Platelets
BUN
Creatinine
AST
ALT
Value
20,500
9.1
25.4
473
23
0.5
200
98
Reference range
(Web search)
5000-19,500
12.7-18.3
37.4-55.9
288-598
5-18
0.2-0.5
0-60
0-50
Echocardiogram report reviewed.
Impression: Patient is a two-month-old girl with a recent onset of fever and now
severely decreased ventricular function.
Differential diagnosis:
Acute viral myocarditis
Dilated cardiomyopathy
Given her history of fever and acute decompensation, it is reasonable to treat her
presumptively for myocarditis, therefore, my recommendations are as follows:
Recommendations:
The patient should receive hemodynamic support as directed by the
Cardiovascular Intensive Care Unit (CVICU).
We agree with the decision to defer Extracorporeal Membrane Oxygenation
(ECMO) cannulation for now despite the mild trans-aminitis. Laboratory
studies will be redrawn in eight hours to get a trajectory for the patient. If
she shows worsening end-organ function, ECMO will likely be necessary.
We recommend treating the patient with Intravenous Immunoglobulin
(IVIG) a total of 2 g/kg (May be broken up into 2 doses) over a 24-hour
period. IVIG is believed to have some therapeutic effect with acute
myocarditis.
We would not treat with steroids now as the patient may continue to be
actively infected.
Recommended diagnostic workup: Respiratory aspirate for Direct
Fluorescent Antibodies (DFA) as well as parvovirus, adenovirus and
enterovirus Polymerase Chain Reaction (PCR), blood cultures and draw a
panel of reactive antibodies in anticipation of blood transfusions and IVIG
for pretransplant work up.
22 of 87
BATES Ref
XXXX
XXXX
DATE
PROVIDER
08/21/YYY ABC
Y
Children's
Hospital
Binh Huynh,
M.D.
08/22/YYY ABC
Y
Children's
Hospital
Andrew
XXXXXXX,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
The patient is not currently listed for transplantation. If the patient clinically
worsens, then we will consent the family for transplantation and make a
determination as to the patient’s candidacy. For the time being, transplant
candidacy will be deferred as the patient has a reasonable chance of
recovering if this is in fact acute fulminant myocarditis.
Minimize blood and platelet transfusions as well as blood draws as much as
possible as they are sensitizing events. Of course, if it is required for her
CVICU management, these therapies may be used at the discretion of the
CVICU team.
We will continue to follow the patient daily.
@ 02:46 PM: Ultrasound of head:
Clinical history: Two-month-old female with a history of dilated cardiomyopathy.
Impression: Non-specific linear echogenicity seen in the right thalamus, possibly
representing mineralizing vasculopathy, a nonspecific finding. Differential
considerations would include a Toxoplasmosis, Other agents, Rubella,
Cytomegalovirus, Herpes Simplex (TORCH) infection, chromosomal
abnormalities, or brain injury.
@ 02:10 AM: History and physical for dilated cardiomyopathy:
History reviewed. Patient is a 2-month-old female with dilated cardiomyopathy
versus myocarditis, mechanically ventilated on significant inotropic support with
Dopamine, Epinephrine and Milrinone, admitted for possible ECMO. Right IJ was
placed. Arterial line placement was unsuccessful due to weak/absent pulses by
report. Ceftriaxone was continued.
Height: 57 cm; Weight: 4 kg; Body Mass Index (BMI): 12.311 kg/m2
Physical examination:
Vital signs: Temperature – 36.5° C; Heart rate – 145 in sinus rhythm; BP – 78/60;
Oxygen saturation – 100% in FiO2 of 1.
General: Sedated and paralyzed.
HEENT: ETT in place. Moist, pink oral mucosa.
Lungs: Mildly coarse breath sounds throughout with diminished breath sounds on
both bases, left >right. No wheezes, rales or crackle.
Cardiovascular: Normoactive precordium, S1, S2. No S3, no S4. Regular rate and
rhythm. No murmurs, rubs, or gallops.
Abdomen: Soft, nontender, liver is 2 cm below Right Costal Margin (RCM).
Extremities: Warm to ankles with mildly cool feet and hands. Capillary refill time
two to three seconds. Pulses are equal and strong in all four extremities.
Respiratory support: Conventional ventilation.
Labs:
Parameter
Hemoglobin
Hematocrit
Value
10.3
29.2
23 of 87
Reference range
(Web search)
12.7-18.3
37.4-55.9
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
396-01397
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
024-00029
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
WBC
Platelets
BUN
Creatinine
AST
ALT
OCCURRENCE/TREATMENT
24.6
5-19.5
405
288-598
22
5-18
0.5
0.2-0.5
164
0-60
104
0-50
BATES Ref
Assessment: Patient is a two-month-old girl with a recent onset of fever and now
new-onset of severe systolic left ventricular dysfunction. The differential diagnosis
includes (But is not exclusive of) acute viral myocarditis, primary dilated
cardiomyopathy or anomalous coronary origins. Less likely etiologies include
sepsis, toxin-mediated heart failure, large left-to-right shunt (AV fistula or other
arteriovenous malformations). Given her history of fever and acute
decompensation, we are preemptively treating for viral myocarditis.
08/22/YYY ABC
Y
Children's
Hospital
Hediah XXX,
M.D.
Plan:
Cardiac failure - Uncompensated cardiogenic shock with transaminitis
(Acute hepatic insufficiency) and elevation in creatinine (Acute renal
insufficiency). Currently supported with Dopamine, Epinephrine and
Milrinone with ongoing discussion regarding elective cannulation for
extracorporeal membrane oxygenation support. Serial laboratory analysis
for end- organ function/evolution. Near Infrared Spectroscopy (NIRS)
monitoring. Serial lactate levels and Mixed Venous Oxygen saturation
(MVO2). We will start IVIG a total of 2 g/kg (Broken up into 2 doses) over
a 24-hour period. Diagnostic evaluation includes respiratory aspirate for
viral DFA, parvovirus, adenovirus and enterovirus PCR. Full
echocardiogram review and 12-lead EKG. Exam does not show any bruits
consistent with extra-cardiac left to right shunt. We will also obtain a panel
of reactive antibodies prior to blood transfusions.
Acute respiratory failure due to pulmonary edema from left atrial
hypertension. Controlled mechanical ventilation to optimize gas exchange.
CXR consistent with pulmonary edema without pleural effusions.
Anemia secondary to critical illness and recent phlebotomy. Will transfuse
Packed Red Blood Cells (PRBC) after immunologic studies are obtained.
Fluid overload. Will start a low dose Lasix infusion once hemodynamics
are stabilized,
On Fentanyl infusion. Judicious use of Benzodiazepines.
Parents updated as to the critical condition of patient. We will continue
discussions about need for ECMO and the possibility for heart
transplantation.
@ 04:10 AM: X-ray of chest:
Clinical history: Ten-week-old female with dilated cardiomegaly.
Impression:
Mild cardiomegaly, stable.
Small bilateral pleural effusions.
Endotracheal tube at the level of T3 (At the carina) on the final radiograph
(08/22/YYYY at 05:18 AM). Patient with chin flexed. The endotracheal
24 of 87
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
392-01393
XXXX
XXXX
DATE
PROVIDER
08/23/YYY ABC
Y
Children's
Hospital
Heika XxxxxYyyyy, M.D.
08/23/YYY ABC
Y
Children's
Hospital
Inger Xxxxx,
M.D.
08/24/YYY ABC
Y
Children's
Hospital
Peter Xxx,
M.D.
08/25/YYY ABC
Y
Children's
Hospital
XXXYYY,
M.D.
08/25/YYY ABC
Y
Children's
Hospital
Jonathan
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
tube may need to be adjusted.
Mild gaseous distension of several loops of bowel, incompletely evaluated
by this chest radiograph.
@ 04:47 AM: X-ray of chest:
Clinical history: Ten-week-old female with dilated cardiomegaly.
Impression:
Endotracheal tube tip at the thoracic inlet with patient’s chin down.
Left subclavian catheter tip in the left brachiocephalic vein.
Retrocardiac opacity, likely representing atelectasis.
@ 11:08 AM: Echocardiogram report:
Indication: Follow-up function in Dilated Cardiomyopathy (DCM)
Summary:
A tiny patent foramen ovale
The left atrium is severely dilated
Mild to moderate mitral valve regurgitation
Mild tricuspid regurgitation
There is mild pulmonary regurgitation
Severely dilated left ventricle
Severely decreased LV systolic function
@ 05:10 AM: X-ray of chest:
Clinical history: Eleven-week-old female with dilated cardiomyopathy
Impression:
Left subclavian catheter, unclear if arterial or venous. If venous, then
suboptimal position near the junction of the thoracic duct in the subclavian
vein, predisposing the patient to chylothorax.
Moderate cardiomegaly, stable.
Mild pulmonary edema. Effusion cannot be excluded.
Retrocardiac atelectasis.
@ 05:13 AM: X-ray of chest:
Clinical history: Eleven-week-old female with dilated cardiomyopathy
Impression:
Interval decrease in cardiomegaly
Mild pulmonary edema, improved
Improved aeration of both lungs, with re-expansion of left lower lobe
atelectasis
@ 03:10 PM: Internal Medicine, Immunology and Allergy consultation for
dilated cardiomyopathy:
History reviewed. Genetics was requested to consult on the patient, to evaluate for
concern of underlying metabolic disorder that would have contributed to the
25 of 87
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
391
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
280-01282
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
389-01390
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
388-01389
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
XXXX
XXXX
DATE
PROVIDER
Xxxxyyyy,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
development of patient’s current cardiomyopathy.
Gestation: Patient was born at term to a 27-year-old mother, father 29 years of age.
There were no noted complications during pregnancy, except that mother reports
having significant emesis throughout pregnancy, and requiring bed rest due to early
contractions. The patient was born via normal spontaneous vaginal delivery. Birth
weight 6 pounds 1 ounce at XYZ Memorial Hospital. There were no complications
noted during birth or there afterwards. She was discharged after approximately two
days.
Development: The patient was previously noted as having developed a social
smile, was active, had good tone, moving all extremities well, eating well, without
problems, as reported by the patient’s mother.
Laboratories and imaging studies: Echocardiogram shows PFO versus small
ASD, with left-to-right flow, moderate tricuspid regurgitation, moderate mitral
regurgitation, mild aortic regurgitation, moderate pulmonary regurgitation. No left
ventricular outlet obstruction is appreciated. No pulmonary stenosis. A left aortic
arch is observed and severe left ventricular dysfunction, without evidence of
pericardial effusion. Electrolytes are currently within normal limits. Lactate is 1.
Urine Cytomegalovirus (CMV) negative. Respiratory DFA is negative. Parvo virus
is negative. Adenovirus is negative. AST 86, ALT 107.
Review of systems:
Cardiovascular: Severe dilated cardiomyopathy.
Respiratory: Significant respiratory distress. Currently intubated.
Physical examination:
Cardiovascular: Regular rate and rhythm. Murmurs consistent with the patient’s
echocardiogram are difficult to appreciate, due to rapid heart rate.
Thorax: Breath sounds are clear to auscultation bilaterally.
Neurologic: Patient is sedated. However, is responsive to auditory and tactile
stimulation, shows appropriate tone and grasp reflex, despite sedation.
Impression: The patient is a two-month-old female without significant past medical
history, now presenting with dilated cardiomyopathy and severe left ventricular
dysfunction, with a concern for underlying metabolic disorder.
Summary and comment: In this two-month-old female with rapid onset
cardiomyopathy and associated heart failure, the differential includes a number of
possible genetic conditions and possible underlying metabolic disorders. The
differential includes 1p36 deletion syndrome, Alstrom syndrome, Refsum disease,
dilated cardiomyopathy with ataxia, and Barth syndrome. Underlying metabolic
disorders that could contribute to the patient’s current presentation include disorders
of fatty acid oxidation, organic acidemias, amino acidopathies, glycogen storage
disease, congenital disorders of glycosylation and mitochondrial disorders.
At this time, the patient does not present with significant dysmorphology that would
indicate any one specific syndrome or underlying dysmorphic disorder in particular.
Accordingly, we recommend a general assessment for disorders of metabolism, to
26 of 87
BATES Ref
015-00019
XXXX
XXXX
DATE
PROVIDER
08/26/YYY ABC
Y
Children's
Hospital
XXXYYY,
M.D.
08/26/YYY ABC
Y
Children's
Hospital
08/26/YYY ABC
Y
Children's
Hospital
Justin xxxx,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
include total and free carnitine, acyl-carnitine profile, plasma amino acids, urine
organic acids, Creatine-Kinase (CK) level, and carbohydrate deficient transferrin
testing to be sent. If this testing is demonstrated to be normal, we would consider
recommend sending testing for a cardiomyopathy genetic screening panel. Primary
team can also consider an Ophthalmology exam in this patient.
@ 05:23 AM: X-ray of chest:
Clinical history: Eleven-week-old female with dilated cardiomyopathy
Impression:
Lines and tubes in stable condition
Moderate cardiomegaly, stable
Pulmonary edema, improved
Labs - Biochemical genetics:
Parameter
Carnitine, free
Carnitine, total
Acyl/Free carnitine ratio
Hydroxyproline
Asparagine
Ornithine
Interim summary note:
Value
19.2
23.1
0.2
29
11
104
Reference range
18-58 umol/L
20-71 umol/L
0.1-0.4
0-23 nmol/L
21-95 nmol/L
22-103 nmol/L
Brief identification: 2-month-old female with viral myocarditis versus primary
cardiomyopathy mechanically ventilated on inotropic support with Dopa,
Epinephrine and Milrinone.
Assessment and plan: 2 month old girl presenting with cardiogenic shock and
newly diagnosed severely depressed left ventricular systolic function with suspected
LV non compaction. The differential diagnosis includes acute viral myocarditis or
primary dilated cardiomyopathy. Viral studies have been negative thus far.
Cardiovascular: Cardiac failure with compensated cardiogenic shock on
vasopressor support. Mild end-organ dysfunction-transaminitis (Acute hepatic
insufficiency), improving and elevation in creatinine (Acute renal insufficiency),
resolved. Currently supported with Dopamine, Epinephrine and Milrinone. Wean
Epinephrine as to 0.02 mcg/kg/min now and if stable NIRS and Mixed Venous
Oxygen Saturation (SVO2) in 12 hrs will wean again. Continue Dopamine to 5
mcg/kg/min and milrinone 0.75 mcg/kg/min. Change to daily cardiac metabolic
panel to monitor end-organ function with Epinephrine wean. Lactate levels and
MVO2 every morning. Defer mechanical device support for now with stable
hemodynamics on current support and evidence of good end organ function
Heart failure/Heart transplant: Currently not listed for transplant, workup in
progress. Minimize transfusions. Plan for cardiac catheterization on 08/29/YYYY
for biopsy and hemodynamics for transplant evaluation. Will need ECMO standby.
Respiratory: Acute respiratory failure due to pulmonary edema from left atrial
hypertension. Controlled mechanical ventilation to optimize gas exchange. CXR
consistent with pulmonary edema without pleural effusions. No change in
ventilation support while weaning Epinephrine to minimize myocardial
27 of 87
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
387
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_03
997-04003
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
079-00082
XXXX
XXXX
DATE
PROVIDER
08/27/YYY ABC
Y
Children's
Hospital
Beverley
XXX, M.D.
08/28/YYY ABC
Y
Children's
Hospital
Beverley
XXX, M.D.
08/28/YYY ABC
Y
Children's
Hospital
Inger Xxxxx,
M.D.
08/29/YYY ABC
Y
Children's
Hospital
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
work/oxygen demand.
Heme: No immediate issues. Anemia secondary to postnatal nadir, critical illness
and recent phlebotomy. Status post PRBC transfusion times 2 on 08/23/YYYY.
Continue systemic anticoagulation with Heparin given risk for systemic
embolization with severely depressed function. Adjust Heparin GTT to reach goal
levels. Start Epogen.
Gastrointestinal: Currently None Per Oral (NPO). Improving transaminitis.
Maximize nutrition. Continue Zantac. Trophic feeds once stable off Epinephrine.
Renal: Mild renal insufficiency with cardiogenic shock. Creatinine normalized and
making good urine on Lasix GTT. Appears euvolemic on exam. Goal fluid balance
for today is even to slightly negative. Change to Lasix as needed. Continue
Allopurinol. Urinalysis level improved today.
Social: Parents updated as to the critical condition of patient. We will continue
discussions about need for ECMO and the possibility for heart transplantation.
X-ray of chest:
Clinical data: Two-month-old female with dilated cardiomyopathy, viral
myocarditis versus primary cardiomyopathy. Evaluate for atelectasis.
Impression:
Stable postoperative changes and supportive equipment including ETT with
tip in the mid-trachea, an enteric tube with tip in the stomach, a right IJ
central venous catheter with tip at the cavoatrial junction and a left
subclavian central venous catheter with tip in the left brachiocephalic vein
Stable moderate cardiomegaly
Clear lungs with no focal atelectasis or consolidation
@ 05:37 AM: X-ray of chest:
Clinical history: Two-month-old female with dilated cardiomyopathy, evaluate
atelectasis.
Impression:
Stable mild to moderate cardiomegaly, and stable mild pulmonary edema
Enteric tube with tip within the proximal stomach, recommend slight
advancement
@ 12:35 PM: Pediatric echocardiogram report:
Indication: Myocarditis, evaluate function pre-catheterization.
Summary:
The left atrium is moderately dilated
Mild mitral valve regurgitation
Severely dilated left ventricle
Severely decreased LV systolic function
Patent foramen ovale
@ 03:15 PM: Echocardiogram report:
Indication: Follow-up dilated cardiomyopathy, status post biopsy for pericardial
effusion. (Pericardial effusion biopsy procedure report is not available for review).
28 of 87
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
385-01386
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
384-01385
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
277-01279
XXXXS_29
7160_rec fm
ABC
Children's
XXXX
XXXX
DATE
PROVIDER
Rajesh Xxx,
M.D.
08/29/YYY ABC
Y
Children's
Hospital
Beverley
XXX, M.D.
08/30/YYY ABC
Y
Children's
Hospital
Beverley
XXX, M.D.
08/31/YYY ABC
Y
Children's
Hospital
XXXYYY,
M.D.
08/31/YYY ABC
Y
Children's
Hospital
Peter Xxx,
M.D.
08/31/YYY Sunquest Lab
Y
Gerald XXX,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Impression: Status post biopsy in a patient with dilated cardiomyopathy. There is
no pericardial effusion. The left ventricle is dilated and function is severely
depressed and unchanged.
Summary:
Directed study to assess pericardial effusion
Severely decreased LV systolic function
Mild to moderate mitral valve regurgitation
@ 03:15 PM: X-ray of chest:
Clinical data: Atelectasis
Impression:
Slightly high ETT, otherwise stable tubes and lines
Unchanged mild cardiomegaly and congestion
X-ray of chest:
Clinical history: Dilated cardiomyopathy, evaluate pulmonary edema.
Impression: Increasing cardiomegaly and pulmonary edema on the current exam in
comparison with previously. The right subclavian line appears lower in position,
currently within the mid-right atrium. Other findings are essentially stable.
@ 04:20 AM: X-ray of chest:
Reason for exam: Pulmonary edema.
Impression:
Low positioning of the endotracheal tube with tip directed towards the right
mainstem bronchus, this tube is lower than on previous examinations.
Advancement of a left subclavian line into the left innominate vein.
Borderline cardiomegaly.
@ 12:57 PM: X-ray of abdomen:
Clinical data: Naso-Jejunal (NJ) placement
Impression:
Nasogastric tube has advanced into the duodenum.
New right femoral Peripherally Inserted Central Catheter (PICC) line in
place with the tip overlying the L4 vertebral body to the right of midline.
Right subclavian catheter tip remains overlying the right atrium.
Pathology report for endomyocardial biopsy:
Clinical diagnosis: Cardiomyopathy
Specimen submitted: Right ventricular endomyocardial biopsy
Diagnosis:
Heart, Right ventricular endomyocardial biopsy: Hypertrophy and fibrosis
29 of 87
BATES Ref
Hospital_01
273-01276
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
382-01383
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
380-01381
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
379-01380
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
313-01314
XXXXS_29
6150_rec fm
Stanford
Hospitals &
Clinics_000
12
XXXX
XXXX
DATE
PROVIDER
09/01/YYY ABC
Y
Children's
Hospital
David
Xxxxxx, M.D.
09/01/YYY ABC
Y
Children's
Hospital
Peter Xxx,
M.D.
09/01/YYY ABC
Y
Children's
Hospital
Sushma
XXXX, M.D.
Elizabeth
Pppp, PA-C
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
compatible with dilated cardiomyopathy.
@ 01:58 AM: EKG report:
Findings:
Sinus tachycardia
Rate - >179
Left ventricular hypertrophy
Repolarization abnormality suggests Left Ventricular Hypertrophy (LVH)
Biatrial enlargement
Non-specific ST and T wave abnormalities; Unchanged from prior
QRSD interval – 85 ms
QT interval – 225 ms
QTc interval – 407 ms
Interpretation: Abnormal ECG
@02:00 AM X-ray of chest:
Reason for exam: Cardiomegaly
Impression:
Stable positioning of an endotracheal tube, enteric tube, left subclavian
arterial line, right central venous line.
Retrocardiac atelectasis, unchanged.
Cardiomediastinal silhouette is abnormal, unchanged.
No pulmonary edema.
Interim summary note:
Problem list:
Dilated cardiomyopathy/LV non-compaction/Congestive Heart Failure
(CHF) with poor LV function. Biopsy suggestive of DCM. Viral studies
and biopsy did not suggest myocarditis. Catheterization: Pulmonary
Capillary Wedge Pressure (PCWP) 12, coronary arteries were normal,
Central Venous Pressure (CVP) 3, low Post-Void Residual(PVR). Inotrope
dependent, on Dopamine and Milrinone. Listed for heart transplant, status
1A.
Respiratory failure, mechanically ventilated
Opioid and Benzodiazepine dependence
Feeding intolerance, poor nutritional status
Anemia, multifactorial
Chronic anticoagulation for prophylaxis of thrombus in the setting of poor
LV function
Hospital course: History reviewed. Patient was weaned off Epinephrine, and has
been maintaining stable hemodynamics and end organ perfusion on Dopamine of 5
mcg/kg/min, and Milrinone 0.5 mcg/kg/min. She has been activated as a status 1A
on the heart transplant waiting list.
From a pulmonary standpoint, patient remains intubated and mechanically
30 of 87
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
292
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
377-01378
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
075-00078
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
ventilated on moderate settings. She has good compliance and adequate
oxygenation. It is unclear if patient will be able to tolerate the physiologic stress of
extubation, given her limited cardiac reserves. To optimize her chances of success,
we anticipate deferral an extubation trial until she has had one week of full
nutritional support
BATES Ref
In the course of her critical illness, patient has developed a dependence on opioids
and Benzodiazepines. She currently is on continuous infusions of Morphine and
Versed to maintain her comfort and safety, while intubated with invasive
monitoring lines. Her Morphine and Versed infusions are in the process of being
transitioned to enteral Methadone and Ativan over the next 48 hours.
Patient had been breastfeeding prior to admission. She had been supported with
Total Parenteral Nutrition (TPN), which is being weaned off as her enteral feeds are
advanced. Per nutrition, her goal feeding volume is 23ml/hr of Meat and Bone Meal
(MBM). We are following her tolerance of feeding advance closely. To maintain
euvolemia, she receives scheduled IV Lasix. CVP has been ranging from 3-5.
09/02/YYY ABC
Y
Children's
Hospital
XXXYYY,
M.D.
09/03/YYY ABC
Y
Children's
Hospital
Heike XxxxxYyyyy, M.D.
09/04/YYY ABC
Y
Children's
Hospital
Heike XxxxxYyyyy, M.D.
Patient had initially struggled with mild renal insufficiency in the setting of
cardiogenic shock. Her Creatinine has since normalized and she is making good
urine on scheduled doses of IV Lasix.
X-ray of chest:
Reason for exam: Cardiomegaly
Impression:
Single frontal chest radiograph demonstrates stable positioning of a leftsided subclavian arterial line, right-sided central line with tip in the
cavoatrial junction, endotracheal tube, and enteric tube.
Unchanged retrocardiac atelectasis.
Cardiomediastinal silhouette is abnormal, unchanged.
X-ray of chest:
Reason for exam: Atelectasis
Impression:
The endotracheal tube is low positioning with tip near the level of T4.
There is stable positioning of an enteric tube, right IJ.
Enlarged cardiomediastinal silhouette, stable.
Unchanged retrocardiac atelectasis.
X-ray of chest:
Reason for exam: Chest expansion
Impression:
The right PICC is projecting into the right atrium. Otherwise, stable
positioning of medical support devices
Unchanged mild peripheral pulmonary edema
Multiple gas distended loops of bowel
31 of 87
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
376-01377
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
375-01376
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
373-01375
XXXX
XXXX
DATE
PROVIDER
09/06/YYY ABC
Y
Children's
Hospital
Francis
XXXXXX,
M.D.
09/06/YYY ABC
Y
Children's
Hospital
Theresa Tacy,
M.D.
09/08/YYY ABC
Y
Children's
Hospital
Ralph Xxxxx,
M.D.
09/08/YYY ABC
Y
Children's
Hospital
Peter Xxx,
M.D.
09/09/YYY ABC
Y
Children's
Hospital
Beverley
XXX, M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
@ 04:00 AM: X-ray of chest:
Reason for exam: Chest expansion
Impression:
Stable positioning of medical support devices
Enlarged cardiomediastinal silhouette that remains unchanged
Mild pulmonary edema, unchanged
@ 10:05 AM: Echocardiogram report:
Indication: Follow-up DCM
Summary:
Severely decreased LV systolic function
The left atrium is mildly dilated
Mild to moderate mitral valve regurgitation
Severely dilated left ventricle
@ 10:29 AM: X-ray of chest:
Clinical history: A 3-month-old with DCM
Reason for exam: ETT placement, evaluate lung fields, NJ placement.
Impression:
Naso-jejunal tube with the tip coiled in the stomach. There is an
endotracheal tube with the tip projecting down to the right mainstem
bronchus. Recommend adjusting the position of these tubes.
Enlarged but unchanged cardiomediastinal silhouette.
Cardiomediastinal shift towards the left hemithorax with associated leftsided atelectasis secondary to endotracheal tube placement.
@ 01:03 PM: X-ray of abdomen:
Clinical history: DCM. NJ placement.
Impression:
NJ tube is positioned with tip in the descending duodenum
Nasogastric tube in the fundus of the stomach
Cardiomegaly and left retrocardiac atelectasis, stable
X-ray of chest:
Reason for exam: Atelectasis
Impression:
Enteric tube coiled in the stomach. Otherwise, stable positioning of medical
supporting devices.
Enlarged but unchanged cardiomediastinal silhouette
Unchanged retrocardiac atelectasis
Unchanged pulmonary edema
32 of 87
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
371-01372
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
270-01272
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
369-01371
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
312-01313
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
365-01368
XXXX
XXXX
DATE
PROVIDER
08/21/YYY ABC
YChildren's
09/09/YYY Hospital
Y
09/09/YYY ABC
Y
Children's
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Labs:
Date
Hgb
(Ref:
10-14
gm/dl)
9.9
Hct
(Ref:
30-42
%)
29
08/21/YY
YY
08/22/YY
9.2
27
YY
08/23/YY
8.2
24
YY
08/24/YY
12.9
38
YY
08/25/YY
13.6
40
YY
08/26/YY
12.9
38
YY
08/27/YY
12.9
38
YY
08/28/YY
10.5
31
YY
08/29/YY
9.5
28
YY
08/30/YY
10.5
31
YY
08/31/YY
11.6
34
YY
09/01/YY
10.9
32
YY
09/02/YY
10.5
31
YY
09/03/YY
11.2
33
YY
09/04/YY
10.9
32
YY
09/05/YY
10.9
32
YY
09/06/YY
10.9
32
YY
09/07/YY
10.9
32
YY
09/08/YY
YY
09/09/YY
10.2
30
YY
Interim summary note:
pH
(Ref:
7.357.45)
7.34
pCO2
(Ref:
35-45)
43.2
pO2
(Ref:
80105)
106
HCO3
(Ref:
22-26)
23.1
O2
Saturati
on (Ref:
95-98)
98
7.43
42.2
172
28.3
100
7.40
52.6
160
31.5
99
7.40
53.8
184
33.1
100
7.39
55.9
142
33.6
99
7.38
55.0
203
32.4
100
7.39
47.4
188
29.0
100
7.35
53.6
200
29.7
100
7.40
43.6
179
27.0
100
7.41
46.0
211
29.5
100
7.43
47.9
196
31.9
100
7.37
55.6
217
32.1
100
7.36
57.7
155
32.7
99
7.35
61.5
40
33.6
70
7.35
58.2
42
32.3
73
7.32
63.0
39
32.6
67
7.35
61.5
36
33.9
64
7.38
55.2
28
32.4
50
7.38
54.4
38
31.8
70
7.30
61.1
36
29.8
60
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_03
971-03996
XXXXS_29
7160_rec fm
33 of 87
XXXX
XXXX
DATE
PROVIDER
Hospital
Elizabeth
Xxxxx, M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Hospital course: History reviewed. Patient has been maintaining stable
hemodynamics and end organ perfusion on Dopamine of 3 mcg/kg/min and
Milrinone 0.25 mcg/kg/min while intubated. She remains activated as a status 1A
on the heart transplant waiting list. With crying and agitation she does become
tachycardic with rates up to 200. While intubated, she has tolerated brief episodes
of tachycardia. She is a candidate for emergency mechanical circulatory support if
needed.
BATES Ref
ABC
Children's
Hospital_00
072-00074
From a pulmonary standpoint, patient has intubated and mechanically ventilated
since her admission on 08/21/YYYY. She has good compliance and adequate
oxygenation. Because it was unclear if she would tolerate the physiologic stress of
extubation, given her limited cardiac reserves, she remained intubated throughout
this week to allow for more nutritional support and Continuous Positive Airway
Pressure (CPAP) trials to assess her respiratory mechanics. She tolerated CPAP
trials with normal Work of Breathing (WOB) and acceptable Arterial Blood Gases
(ABG’s) and somatic NIRS
She was extubated today to High Flow Nasal Cannula (HFNC) and initially
struggled with mild upper airway obstruction and difficulty clearing secretions. This
progressed over the next 4 hours and she became tachycardic, agitated and poorly
perfused. CXR prior to reintubation showed completed collapse of the left lung.
From an airway standpoint, she was re-intubated without difficulty. Her cardiac
output deteriorated as she developed respiratory failure and during the process of
reintubation. With reintubation she received small bolus doses of Phenylephrine and
a fluid bolus to stabilize her blood pressure. In addition, the Dopamine and
Milrinone infusions were increased. With this decompensation, she was tachycardic
with a drop in her somatic NIRS (Lowest in 40’s). However within an hour of
reintubation, her Heart Rate (HR) returned to 130’s and NIRS came back up to
upper 60’s. The overall period of stress was approximately 2 hrs.
In the course of her critical illness, patient has developed a dependence on Opioids
and Benzodiazepines. She has been transitioned to enteral Methadone and Ativan
with as needed doses of Versed and Morphine for breakthrough. She has tolerated
weaning of the Methadone and Ativan doses this week.
Patient is being supported with TPN while NPO for the extubation trial. Prior to this
she was tolerating goal feeds of MBM 26 kcal/oz at 24ml/hr. To maintain
euvolemia, she receives scheduled enteral Lasix. CVP has been ranging from 3-5.
09/10/YYY ABC
Y
Children's
Hospital
Gail Xxxxx,
M.D.
Patient had initially struggled with mild renal insufficiency in the setting of
cardiogenic shock. Her Creatinine has since normalized and she is making good
urine on scheduled doses of enteral Lasix.
@ 02:50 AM: EKG report:
Findings:
Sinus rhythm
Normal P-axis, Ventricular rate: 121-179
Repolarization abnormality suggests LVH
ST depression, T negative
34 of 87
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
291
XXXX
XXXX
DATE
PROVIDER
09/10/YYY ABC
Y
Children's
Hospital
Shreyas
Xxxxx, M.D.,
Ph.D.
09/10/YYY ABC
Y
Children's
Hospital
Shreyas
Xxxxx, M.D.,
Ph.D.
09/10/YYY ABC
Y
Children's
Hospital
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Borderline prolonged QT interval
Left atrial enlargement
P-R interval = 92 ms
QT interval = 319 ms
Interpretation: Abnormal ECG
@ 05:55 AM: X-ray of chest:
Clinical data: 3-month-old female with DCM awaiting transplantation. Evaluate
for atelectasis.
Impression:
Stable supportive equipment
Waxing and waning aeration of the left upper lobe with near complete
opacification of the left lung field over sequential radiographs
@ 05:59 AM: X-ray of abdomen:
Clinical data: 3-month-old female with DCM awaiting transplantation. Evaluate
NJ-tube placement.
Impression: Enteric tube with tip likely in the duodenum. Recommend AnteroPosterior (AP) view for further evaluation
@ 12:15 PM: Ultrasound - Venous bilateral lower extremities:
Clinical data: DCM awaiting heart transplant
Impression: Unremarkable. No evidence for venous thrombosis.
09/11/YYY ABC
Y
Children's
Hospital
@ 05:04 AM: X-ray of chest:
Shreyas
Xxxxx, M.D.,
Ph.D.
09/12/YYY ABC
Y
Children's
Hospital
Impression:
Interval placement of enteric tube with tip projecting over the stomach
Interval re-expansion of left lung with better visualization of cardiomegaly
@ 04:05 AM: X-ray of chest:
XXXYYY,
M.D.
09/12/YYY ABC
Y
Children's
Hospital
Rajesh Pppp,
M.D.
Clinical history: DCM
Clinical data: Evaluate lung expansion
Impression:
Moderate cardiomegaly with mild central pulmonary edema, stable when
compared to study dated 09/11/YYYY
There is nasogastric tube tip projecting over the gastroesophageal junction
@ 12:09 PM: Echocardiogram report:
Indication: Evaluate for ventricular thrombus and fibrosis
Findings:
The left atrium is mildly-moderately dilated
35 of 87
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
363-01364
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
311-01312
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
394-01396
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
361-01362
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
359-01360
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
268-01269
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
09/13/YYY ABC
Y
Children's
Hospital
Beverley
XXX, M.D.
09/14/YYY ABC
Y
Children's
Hospital
XXXYYY,
M.D.
09/15/YYY ABC
Y
Children's
Hospital
Francis Xxyy,
M.D.
09/12/YYY ABC
YChildren's
09/15/YYY Hospital
Y
OCCURRENCE/TREATMENT
Mild mitral valve regurgitation is present
Trivial tricuspid valve regurgitation
The left ventricular chamber is severely dilated. Left ventricular systolic
function is severely decreased. The left ventricular mass measures 213.1
g/m2 indexed to the body surface area.
The right ventricular chamber is of normal size. Right ventricular systolic
function is normal.
There is trivial aortic valve insufficiency.
There is trivial pulmonary regurgitation. There is no pulmonary valve
stenosis.
No pericardial effusion.
Summary:
Severely dilated left ventricle
Severely decreased LV systolic function
The left atrium is mildly-moderately dilated
Mild mitral valve regurgitation
X-ray of chest:
Clinical history: 3-month-old patient with DCM awaiting heart transplant
Impression:
Moderate cardiomegaly with mild central pulmonary edema, stable when
compared to study dated 09/12/YYYY.
Left retrocardiac opacity, possibly representing an area of subsegmental
atelectasis versus a developing infiltrate, new when compared to study
dated 09/12/YYYY. Recommend continued attention on follow-up
imaging.
X-ray of chest:
Clinical history: 3-month-old patient with DCM awaiting heart transplant
Impression:
Moderate cardiomegaly with mild central pulmonary edema, stable when
compared to study dated 09/13/YYYY
Left retrocardiac opacity, possibly representing an area of subsegmental
atelectasis, stable when compared to study dated 09/13/YYYY
X-ray of chest:
Clinical history: 3-month-old patient with DCM awaiting heart transplant
Impression:
Moderate cardiomegaly with mild central pulmonary edema, stable when
compared to study dated 09/14/YYYY
Labs:
Date
09/12/YYY 09/13/YYY
Y
Y
36 of 87
09/15/YYY
Y
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
357-01358
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
356-01357
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
355-01356
XXXXS_29
7160_rec fm
ABC
Children's
XXXX
XXXX
DATE
PROVIDER
09/16/YYY ABC
Y
Children's
Hospital
Erika Xxxxx,
M.D.
09/16/YYY ABC
Y
Children's
Hospital
Heike XxxxxYyyyy, M.D.
09/16/YYY ABC
Y
Children's
Hospital
Heike XxxxxYyyyy, M.D.
09/16/YYY ABC
Y
Children's
Hospital
Heike XxxxxYyyyy, M.D.
09/16/YYY ABC
Y
Children's
Hospital
Heike XxxxxYyyyy, M.D.
09/16/YYY ABC
Y
Children's
Hospital
David
Xxxxxx, M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
4.0
8.0
2.5
C-reactive protein
(Ref: <0.9)
@ 04:20 AM: X-ray of chest:
Clinical history: Patient with DCM awaiting heart transplant
Impression:
Moderate cardiomegaly with central pulmonary edema, stable when
compared to study dated 09/15/YYYY.
The patient’s right upper extremity PICC line tip is projecting over the right
atrium.
The patient’s endotracheal tube tip is extending towards the right main stem
bronchus. Recommend repositioning.
@ 10:50 AM: X-ray of chest:
Clinical history: Patient with DCM awaiting heart transplant
Impression:
Moderate cardiomegaly with central pulmonary edema, stable when
compared to study dated 09/16/YYYY.
The patient is status post extubation.
@ 12:00 PM: X-ray of chest:
Clinical history: Patient with DCM awaiting heart transplant
Impression:
Moderate cardiomegaly with central pulmonary edema, stable when
compared to study dated 09/16/YYYY
@ 12:00 PM: X-ray of abdomen:
Clinical data: Patient with DCM awaiting heart transplant. Evaluate bowel gas
pattern.
Impression: Unremarkable gas pattern without evidence of obstruction of ileus.
@ 03:36 PM: X-ray of chest:
Clinical history: 3-month-old female, evaluate atelectasis.
Impression:
Interval resolution of left lower lobe atelectasis. Low lung volumes with no
focal consolidation.
Persistent moderate cardiomegaly with central pulmonary edema.
Interim summary note:
Hospital course: Patient has been maintaining stable hemodynamics and end organ
perfusion on Dopamine of 3 mcg/kg/min and Milrinone 0.5 mcg/kg/min while
intubated. She remains activated as a status 1A on the heart transplant waiting list.
With crying and agitation she does become tachycardic with rates up to 200. While
intubated, she has tolerated brief episodes of tachycardia. She is a candidate for
37 of 87
BATES Ref
Hospital_04
004
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
353-01354
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
352-01353
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
351-01352
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
310-01311
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
350-01351
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
068-00071
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
emergency mechanical circulatory support if needed.
BATES Ref
From a pulmonary standpoint, patient has intubated and mechanically ventilated
since her admission on 08/21/YYYY. She has good compliance and adequate
oxygenation. Because it was unclear if she would tolerate the physiologic stress of
extubation, given her limited cardiac reserves, she remained intubated through
09/01/YYYY to allow for more nutritional support and CPAP trials to assess her
respiratory mechanics. She tolerated CPAP trials with normal WOB and acceptable
ABG’s and somatic NIRS prior to extubation on 09/01/YYYY. Following
extubation on 09/01/YYYY she had progressive respiratory failure with
tachycardia, agitation and deteriorating cardiac output. CXR prior to reintubation
showed completed collapse of the left lung. From an airway standpoint, she was reintubated without difficulty. She recovered from this stressor and within 48 hrs was
back to baseline.
Over the past week she has tolerated enteral feedings, is back to baseline low
ventilator settings and CXR (Mild pulmonary edema and retrocardiac atelectasis)
and tolerated a CPAP trial. She was extubated 09/16/YYYY initially to HFNC and
then transitioned to nasal CPAP as she had increased work of breathing. Her CXR
remained stable and on CPAP she did not collapse her left lung. However, she had
marginal reserves and was tachycardic to the 180-220 range with agitation, crying
and airway clearance maneuvers despite generous pain and sedation medications.
Of note her VBG’s were stable with a normal pH, CO2.
In the course of her critical illness, patient has developed a dependence on opioids
and benzodiazepines. She has been transitioned to enteral Methadone and Ativan
and this had been well tolerated prior to her extubation/reintubation on
09/01/YYYY. Over the past week she has required the addition of a Morphine and
Versed infusion for adequate pain control and sedation with additional as needed
doses. She has tolerated slow weaning of these infusions over the past 2 days.
Patient is being supported with TPN while NPO for the extubation trial. Prior to this
she was tolerating goal feeds of MBM 28 kcal/oz at 25ml/hr. To maintain
euvolemia, she receives scheduled enteral Lasix. CVP has been ranging from 5-7.
09/17/YYY ABC
Y
Children's
Hospital
XXXYYY,
M.D.
09/18/YYY ABC
Y
Children's
Hospital
Patient had initially struggled with mild renal insufficiency in the setting of
cardiogenic shock. Her Creatinine has since normalized and she is making good
urine on scheduled doses of enteral Lasix.
@ 05:20 AM: X-ray of chest:
Clinical history: Patient with DCM, evaluate chest tube placement.
Impression:
Stable appearance of supportive equipment
Persistent moderate cardiomegaly and mild pulmonary edema
Slightly retrocardiac opacity, consistent with left lower lobe atelectasis
X-ray of chest:
Clinical history: 3-month-old female with DCM, awaiting heart transplantation.
38 of 87
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
348-01349
XXXXS_29
7160_rec fm
ABC
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
XXXYYY,
M.D.
09/19/YYY ABC
Y
Children's
Hospital
XXXYYY,
M.D.
09/20/YYY ABC
Y
Children's
Hospital
Rajesh Pppp,
M.D.
09/21/YYY ABC
Y
Children's
Hospital
Peter Xxx,
M.D.
09/23/YYY ABC
Y
Children's
Hospital
Sushma
XXXX, M.D.
OCCURRENCE/TREATMENT
Impression:
Endotracheal tube with tip at the level of T4-5, slightly above the carina
directed toward the right main stem bronchus. There are two enteric tubes,
one with tip in the second portion of the duodenum, one with tip in the
stomach.
Persistent low lung volumes.
Cardiomediastinal silhouette enlargement, unchanged.
Retrocardiac atelectasis, unchanged.
Nonobstructive bowel gas pattern.
X-ray of chest:
Clinical data: Chest expansion, DCM.
Impression: Unchanged cardiomegaly.
Echocardiogram report:
Indication: Follow-up cardiomegaly, rule out thrombus.
Summary:
Severely decreased LV systolic function
Severely dilated left ventricle
The left atrium is mildly-moderately dilated
Mild tricuspid regurgitation
Mild mitral valve regurgitation
X-ray of chest:
Clinical history: DCM
Impression: Stable appearance of moderate cardiomegaly.
Interim summary note:
Hospital course: History reviewed. There was a second attempt at extubation on
09/16/YYYY. She was initially on HFNC and then transitioned to nasal CPAP as
she had increased work of breathing. Her CXR remained stable and on CPAP she
did not collapse her left lung. However, she had marginal reserves and was
tachycardic to the 180-220 range with agitation, crying and airway clearance
maneuvers despite generous pain and sedation medications. Of note her VBG’s
were stable with a normal pH, CO2. Because of her marginal reserves and concern
she would not be able to maintain adequate cardiac output despite maximal support
she was re-intubated without difficulty. She recovered quickly and was back to
baseline within 48 hrs and has remained stable on low mechanical ventilator
settings. The plan is for patient to remain intubated and mechanically ventilated to
allow for growth and rest pre-transplant. She currently does not have any ventilator
associated complications and has been quite stable.
Over the past week, she has tolerated a slow wean of the infusions and is requiring
39 of 87
BATES Ref
Children's
Hospital_01
309-01310
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
347-01348
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
265-01267
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
345-01347
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
063-00067
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
fewer as needed with increased dosing of Methadone and Ativan. The plan will be
to slowly wean the Methadone and Ativan by 10% on alternating days starting on
09/24/YYYY.
BATES Ref
Patient is tolerating full volume enteral feedings, initially with fortified MBM and
now with fortified Enfamil. The MBM stores have been depleted, patient’s mother
is taking intermittent Xanax and is saving all milk pumped 40 hrs after Xanax
dosing (This is to minimize her exposure to additional benzodiazepine in the breast
milk). To maintain euvolemia, she receives scheduled enteral Lasix. CVP has been
ranging from 5-7.
Patient had initially struggled with mild renal insufficiency in the setting of
cardiogenic shock. Her Creatinine has since normalized and she is making good
urine on scheduled doses of enteral Lasix.
09/24/YYY ABC
Y
Children's
Hospital
Francis
XXXXXX,
M.D.
09/26/YYY ABC
Y
Children's
Hospital
Ritu Xxx,
M.D.
09/26/YYY ABC
Y
Children's
Hospital
Ralph Xxxxx,
M.D.
09/29/YYY ABC
Y
Children's
Hospital
Patient had fever with elevated WBC and C-Reactive Protein (CRP) following
extubation on 09/01/YYYY. She received a 3 day course of Vancomycin and
Zosyn. Blood and urine cultures were no growth, WBC normal and she had no focal
signs of infection.
X-ray of chest:
Clinical data: 3-month-old female with DCM.
Impression:
Stable postoperative chest
Moderate cardiomegaly, stable
Mild interstitial edema, stable
@ 11:07 PM: EKG report:
Findings:
Sinus tachycardia
Rate >186
Probable LVH with secondary repolarization abnormality
Borderline prolonged QT interval – 283 ms
QTc > 460 ms
Interpretation: Abnormal ECG.
@ 11:10 PM: X-ray of chest:
Clinical history: 3-month-old female with DCM and CHF.
Impression:
Stable cardiomegaly and mild pulmonary edema
Stable lines and drains – ETT is seen with its tip above the carina. A right
subclavian line is seen with its tip at the superior vena cava, stable position
of two nasogastric tubes.
Interim summary note:
Hospitalization by System:
40 of 87
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
343-01344
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
290
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
341-01343
XXXXS_29
7160_rec fm
ABC
XXXX
XXXX
DATE
PROVIDER
David
Xxxxxx, M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Cardiovascular: History reviewed. Patient has been maintaining stable
hemodynamics and end organ perfusion on Dopamine of 3 mcg/kg/min and
Milrinone 0.5 mcg/kg/min while intubated. Due to her past failed intubations and
the thought that she is unable to maintain adequate hemodynamics while extubated,
the plan is to leave her intubated while she awaits a heart. Over the last week she
has been more tachycardic with HRs in the 150s with increases to the 200s when
agitated. The exact etiology of her tachycardia is unclear. She received PRBCs on
09/26/YYYY with little improvement. Her sedation was also adjusted with some
improvement in her resting HR. On 09/29/YYYY we decreased the Dopamine to
see if this was causing her tachycardia. The plan is that if the tachycardia continues
to persist, we will try Digoxin.
Respiratory: From a pulmonary standpoint, patient has been intubated and
mechanically ventilated since her admission on 08/21/YYYY. She has good
compliance and adequate oxygenation. Because it was unclear if patient would
tolerate the physiologic stress of extubation, given her limited cardiac reserves, she
remained intubated through 09/01/YYYY to allow for more nutritional support and
CPAP trials to assess her respiratory mechanics. She tolerated CPAP trials with
normal WOB and acceptable ABG’s and somatic NIRS prior to extubation on
09/01/YYYY. Following extubation on 09/01/YYYY she had progressive
respiratory failure with tachycardia, agitation and deteriorating cardiac output. CXR
prior to reintubation showed completed collapse of the left lung. From an airway
standpoint, she was re-intubated without difficulty. She recovered from this stressor
and within 48 hrs was back to baseline. She failed extubation again on
09/16/YYYY this time with tachycardia, decreasing NIRS and agitation. She was
electively re-intubated and the decision was made to leave her intubated while she
awaits a heart. She was weaned back down to low ventilation settings and her CXR
has shown stable mild pulmonary edema. We started daily CPAP sprints on
09/26/YYYY which she has tolerated well. She had a mucus plug on 09/27/YYYY
which required an intermittent increase in her ventilation settings and delayed her
sprints. She has also had increased yellow secretions, but no evidence of infection.
Pulmozyme was started on 09/27/YYYY with good improvement in her secretions.
Neurology: In the course of her critical illness, patient has developed a dependence
on opioids and benzodiazepines. She has been transitioned to enteral Methadone
and Ativan and this had been well tolerated prior to her extubation/reintubation on
09/01/YYYY. She was restarted on Morphine and Versed infusions after her failed
extubation and was eventually weaned off again by 09/24/YYYY. Since then she
has struggled with withdrawal requiring increases in her Methadone and Ativan
doses and multiple as needed. On 09/28/YYYY her Methadone and Ativan was
changed to alternating every 4 hour dosing with a decrease in her needed
requirements.
Gastrointestinal: TPN has been required during periods of NPO around
extubation, however, she has mostly received enteral feeds with a focus of
maximizing her nutrition. Currently she is receiving Enfamil NJ feeds of 30ml/hour
(28 Kcal) for l50 ml/kg/day and 120 kcal/kg/day with good weight gain of 10-20
g/day. Beneprotein was added to increase her protein intake as her prealbumin
levels have been low. We are following her prealbumin levels weekly. She is also
receiving a multivitamin. Breast milk supply: Mother is pumping regularly to but is
taking Xanax periodically. She is saving MBM that is pumped >40 hrs after her last
Xanax dose
Renal: Patient had initially struggled with mild renal insufficiency in the setting of
41 of 87
BATES Ref
Children's
Hospital_00
059-00062
XXXX
XXXX
DATE
PROVIDER
10/02/YYY ABC
Y
Children's
Hospital
Erika Xxxxx,
M.D.
10/02/YYY ABC
Y
Children's
Hospital
Daniel
Xxxxyyyy,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
cardiogenic shock. Her Creatinine has since normalized and she is making good
urine on scheduled doses of enteral Lasix twice daily. She did receive additional
doses of Lasix this week for concern over increased pulmonary edema on CXR or a
positive fluid balance over 400 cc. We are following her renal function bi-weekly as
a decrease in her renal function would be an indicator for placement on a
Ventricular Assist Device (VAD).
Heme: Patient is at risk for thrombus formation due to her depressed LV function
and cavitation seen on Echocardiogram. She was initially maintained on a
prophylactic Heparin infusion of 10 units/kg/hour and Aspirin (ASA). On
09/19/YYYY she was transitioned to prophylactic Lovenox with a goal Anti-Xa
level of 0.3-0.5. Last Anti-Xa level was 0.32 on 09/25/YYYY. She is getting every
other week echo’s to assess for thrombus formation. She is also on Epogen 3 times
a week and iron supplements. She was transfused on 09/26/YYYY for a HCT of 24.
Last HCT on istat was 28 on 09/26/YYYY.
Infectious Disease (ID): Patient had of fever with elevated WBC and CRP
following on 09/12/YYYY. She received a 3 day course of Vancomycin and Zosyn.
All cultures were negative. She has been afebrile and her WBC is now normal and
she has no focal signs of infection.
@ 01:28 AM: X-ray of chest:
Reason for exam: Pleural effusion
Clinical history: 3-month-old female with history of DCM and CHF awaiting heart
transplant.
Impression:
Lower lung volumes
Improved pulmonary edema
ETT at the C7-T1. Other lines and drains remain stable.
Heart failure progress notes:
Chief complaint: 3.5 month-old admitted on 08/21/YYYY with cardiogenic shock
secondary to dilated cardiomyopathy (Biopsy confirmed), now status 1A listed for
transplant.
Interval history: Stable overnight.
Problem-based assessment and plan:
Heart failure: Dilated cardiomyopathy with respiratory failure. Failed extubation
because of poor cardiac output. Severe LV dysfunction by echocardiogram, but has
had stable clinical examination. Currently on Digoxin 28 mg twice daily, Milrinone
0.5 mg. Less tachycardia than previously, range 125-179.
Transplant: Patient is listed as status 1A. Anticipate movement towards
mechanical support if unable to tolerate feeds or remains on significant amount
ventilator support. Teaching ongoing with family. Criteria for Berlin would include:
Persistent acidosis, arrhythmia, hemodynamic instability, evidence for progressive
end-organ failure.
Respiratory failure: Failed extubation times 2, good support on ventilator at this
time with improved chest X-ray appearance and volumes. Will continue to re-
42 of 87
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
339-01340
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
091-00094
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
address timing of next extubation attempt, hold at this time.
Renal/Fluids: Adequate fluid management with twice daily Lasix. Input/output
+341. Goal relative euvolemia.
Heme: On Lovenox prophylaxis dosing for clot prophylaxis. On Aspirin.
Nutrition: Tolerating NJ feeds. Monitor closely for tolerance and growth.
Immunology: Will obtain Human Leukocyte Antigen (HLA) typing two weeks
following last blood transfusion and monthly. Last done on 09/12/YYYY. Will
monitor for rising antibody levels, start IVIG if there is an increase.
Sedation: Continue Methadone/Ativan IV every 4th hourly with improved comfort.
BATES Ref
Height: 57 cm; Weight: 5.6 kg
Physical examination:
General: Awake, comfortable.
Ear, Nose, Throat (ENT): Intubated. Mouth moist.
Lungs: Scattered rhonchi bilaterally, but good breathing sounds.
Cardiac: S1/S2 Regular Rate and Rhythm (RRR). No murmurs, rubs or gallops. No
S3 heard today.
Gastrointestinal: Soft non-tender. Liver edge palpable 3 cm below the right costal
margin.
Extremities: Warm, good perfusion.
Musculoskeletal: Reasonable strength.
10/03/YYY ABC
Y
Children's
Hospital
XXXYYY,
M.D.
10/03/YYY ABC
Y
Children's
Hospital
Rajesh Pppp,
M.D.
10/04/YYY ABC
Y
Children's
Hospital
Francis
XXXXXX,
M.D.
Target discharge date: 10/20/YYYY
@ 04:05 AM: X-ray of chest:
Reason for exam: Chest expansion
Impression:
ETT with tip at the level of the carina directed towards the right mainstem
bronchus. There is a right central line with tip in the innominate vein. There
is stable positioning of two enteric tubes.
Enlarged but unchanged cardiomediastinal silhouette.
@ 10:39 AM: Echocardiogram report:
Indication: Follow-up echocardiogram for patient with DCM, pre-heart transplant.
Rule out thrombus formation in left ventricle.
Summary:
Severely decreased LV systolic function
Severely dilated left ventricle
The left atrium is mildly dilated
@ 02:20 AM: X-ray of chest:
Reason for exam: Atelectasis
Impression: Stable cardiomegaly with shallow lung volumes.
43 of 87
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
338-01339
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
263-01264
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
337-01338
XXXX
XXXX
DATE
PROVIDER
10/04/YYY ABC
Y
Children's
Hospital
Steven Xx,
M.D.
Robert
Xxxxxx, M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
@ 08:36 AM: Renal consultation regarding plasma exchange for
desensitization:
History reviewed. Patient was found to have dilated cardiomyopathy and has been
intubated secondary to congestive heart failure. She is currently being offered a
heart transplant, and it was found that she has a C1Q positive antibody, so they are
consulting for plasma exchange for desensitization/antibody removal.
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
011-00014
Review of systems:
Constitutional: Fevers after 2 month old vaccines.
Respiratory: Congestive heart failure.
Cardiovascular: Cardiomyopathy.
Height: 57 cm; Weight: 5.6 kg; BMI: 12.31 kg/m2
Vital signs:
Temperature – 36.8° C
HR – 121
Cuff BP - 68/43
Respiratory rate – 23
Central venous pressure – 12 mmHg
Peripheral pulse rate – 119
Physical examination:
Cardiac: Regular rate and rhythm. No murmur.
Assessment and plan: Patient with dilated cardiomyopathy and congestive heart
failure who we are consulting on for plasmapheresis to remove a C1Q positive
antibody to her donor. Her kidney function is likely normal with a creatinine
clearance of 85mL/min/1.73m2.
10/05/YYY ABC
Y
Children's
Hospital
XXXYYY,
M.D.
10/05/YYY ABC
Y
Children's
Hospital
Olaf Xxxx,
Plasmapheresis: We will not require another catheter placed if we can attach the
plasmapheresis machine to the bypass machine. We will recalculate a 1.5 volume
exchange based on the increased blood volume of the bypass machine plus the
patient’s blood volume. We will use 100% Fresh Frozen Plasma (FF), which will
require 2 units of FFP to be available and thawed during the procedure.
@ 02:41 AM: X-ray of chest:
Clinical data: DCM, CHF
Findings: The ETT is at the carina. There is complete left lung atelectasis. The
enteric tube has been removed. A right IJ tube is in place in the right atrium. The
right subclavian central venous catheter tip is in the distal right brachiocephalic
vein. No pneumothorax. Right lung is clear.
@ 06:36 AM: Operative report for orthotopic heart transplantation:
Pre and postoperative diagnosis: End-stage dilated cardiomyopathy
Procedure:
44 of 87
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
336-01337
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
XXXX
XXXX
DATE
PROVIDER
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Orthotopic heart transplantation
Median sternotomy and cardiopulmonary bypass
*Reviewer's comment: Per this operative report, we note that baby Sophia
underwent orthotopic heart transplantation for her end-stage dilated
cardiomyopathy.
Anesthesia: General anesthesia
Identification: This is a three-month-old infant who has been listed for cardiac
transplantation for about a month and a half due to dilated end-stage
cardiomyopathy. She has spent the last six weeks on the ventilator in the ICU. She
was on inotropes and could not be extubated. Today, a donor heart became
available that was about 80% body size of the recipient. It had good function. We
accepted this heart and proceeded with transplantation. The parents were informed
about risks and benefits, and agreed to proceed.
Procedure in detail: The patient was placed supine on the operating table and
prepped and draped in the usual sterile fashion. We performed a standard median
sternotomy and resected the thymus completely. We opened the pericardium. We
placed pursestring sutures in the ascending aorta, Superior Vena Cava (SVC),
Inferior Vena Cava (IVC) and right upper pulmonary vein. The heart was grossly
dilated and poorly functioning. When the donor heart was about 20 minutes away,
we gave Heparin and went on cardiopulmonary bypass. We cooled to 25 degrees.
We cross-clamped the aorta and removed the old heart in the typical fashion. We
prepared cuffs for the left atrium, SVC and IVC. We transected the great vessels in
typical fashion.
When the donor heart became available, we take it out of the ice and prepared it for
implantation in the typical way. There was a small PFO that we closed with a
suture. We then implanted it starting with the left atrium followed by the IVC
followed by the Pulmonary Artery (PA) and then the aorta. We had vents in the left
atrium and in the pulmonary artery. We then de-aired the left side of the heart and
removed the cross-clamp. We rewarmed the patient and performed the SVC
anastomosis using running 7-0 Prolene for the back wall and a series of interrupted
sutures for the anterior wall. We then came off cardiopulmonary bypass on mild
inotropic support. Cardiac function was excellent. The heart was in sinus rhythm.
Ischemic time had been about three-and-a-half hours. The CVP line on top of the
SVC anastomosis now read about 8 mmHg which made us suspicious of an SVC
narrowing at the anastomotic site.
We measured the Right Atrial (RA) pressure to be about 8 at the time. We,
therefore, went back on cardiopulmonary bypass with bi-cable cannulation and
filleted the anterior part of the SVC anastomosis open and patched it with a piece of
autologous pericardium. We then came off bypass again and decannulated. There
was no obstruction at this point with the supra-anastomotic SVC pressure being four
the second time it came off bypass. We accepted this result and gave Protamine.
There was no substantial bleeding. We placed two chest tubes and two ventricular
pacing wires and closed the sternum with wires and the skin and subcutaneous
45 of 87
BATES Ref
086-00087,
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
090
XXXX
XXXX
DATE
PROVIDER
10/05/YYY ABC
Y
Children's
Hospital
XXXYYY,
M.D.
10/05/YYY ABC
Y
Children's
Hospital
Andrew
XXXXXXX,
M.D.
10/05/YYY ABC
Y
Children's
Hospital
Peter Xxx,
M.D.
10/06/YYY ABC
Y
Children's
Hospital
Peter Xxx,
M.D.
10/06/YYY ABC
Y
Children's
Hospital
Daniel Xxxx,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
tissue in the usual fashion. The patient tolerated this well and was transferred to the
ICU in stable condition.
@ 07:26 AM: X-ray of chest:
Clinical data: Postoperative
Findings: The endotracheal tube has been repositioned with reexpansion of the left
lung. Patient has undergone cardiac surgery with new sternotomy wires, mediastinal
drain and right chest tube in place. No pneumothorax. Cardiomegaly has decreased.
There is new mild pulmonary edema. The right IJ central venous catheter has been
repositioned with its tip now in the proximal SVC.
@ 08:07 AM: EKG report:
Findings:
Sinus rhythm
Normal P-axis, ventricular rate 106-108
Premature ventricular contraction
Probable right ventricular hypertrophy
P-R interval = 87 ms
QT interval = 268 ms
QTc interval = 404 ms
@ 03:36 PM: X-ray of chest:
Reason for exam: Atelectasis
Findings: Re-demonstrated are postsurgical changes in the sternum and
mediastinum, a nasogastric tube, endotracheal tube, right pleural drain and
mediastinal drain. Epicardial pacer leads. These are all stable. Heart size is mildly
enlarged. There has been worsening of aeration in the upper portion of the left
hemithorax since earlier in the day, and persistent left retrocardiac atelectasis. The
right lung remains well expanded. Mild pulmonary edema persists. Right internal
jugular line is stable.
Impression:
Cardiomegaly and mild pulmonary edema, stable.
Worsening atelectasis, left upper lung zone and stable left retrocardiac
atelectasis.
@ 04:50 AM: X-ray of chest:
Reason for exam: Chest expansion
Impression: Improved left lung aeration with stable minimal pulmonary edema.
@ 08:30 AM: Echocardiogram report:
Indication: Follow-up for new heart transplant.
Summary:
Status post heart transplant operation
46 of 87
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
336-01337
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
289
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
334-01335
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
333-01334
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
260-01262
XXXX
XXXX
DATE
PROVIDER
10/06/YYY ABC
Y
Children's
Hospital
Peter Xxx,
M.D.
10/07/YYY ABC
Y
Children's
Hospital
XXXYYY,
M.D.
10/07/YYY ABC
Y
Children's
Hospital
Norman
XXXX, M.D.
10/08/YYY ABC
Y
Children's
Hospital
Shreyas
Xxxxx, M.D.,
Ph.D.
10/08/YYY ABC
Y
Children's
Hospital
Ritu Xxx,
M.D.
10/08/YYY Stanford
Y
Health Care
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Normal LV systolic function
No coarctation of the aorta
Mild tricuspid regurgitation
Mild mitral valve regurgitation
@ 11:22 AM: X-ray of abdomen:
Reason for exam: NJ placement
Impression: New long feeding tube with tip in the duodenum. No acute intraabdominal disease suspected.
@ 03:55 AM: X-ray of chest:
Reason for exam: Chest expansion
Impression:
Stable positioning of medical support devices
Central pulmonary edema
Unchanged enlargement of the cardiomediastinal silhouette
@ 11:36 AM: Echocardiogram report:
Indication: Status post heart transplant, target study to evaluate pulmonary edema
around right atrium, right ventricular function. Concern with increased CVP.
Summary:
Status post heart transplant operation
Normal LV systolic function
There is clot seen around right atrium
Trivial tricuspid regurgitation
@ 05:42 AM: X-ray of chest:
Reason for exam: Chest expansion
Impression:
Stable supportive equipment and post-surgical changes
Slight interval decrease in pulmonary edema
@ 08:46 AM: EKG report:
Findings:
Incomplete analysis due to missing data in precordial lead
Sinus rhythm
Normal P-axis, ventricular rate 106-186
Right ventricular hypertrophy
P-R interval = 97 ms
QT interval = 232 ms
QTc interval = 379 ms
@ 08:49 AM: Pathology report for thymus and native heart:
Diagnosis:
47 of 87
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
307-01308
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
332-01333
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
258-01259
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
331
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
287
XXXXS_29
6150_rec fm
Stanford
XXXX
XXXX
DATE
PROVIDER
Gerald XXX,
M.D.
10/09/YYY ABC
Y
Children's
Hospital
Peter Xxx,
M.D.
10/09/YYY ABC
Y
Children's
Hospital
Ritu Xxx,
M.D.
10/09/YYY ABC
Y
Children's
Hospital
Heike XxxxxYyyyy, M.D.
10/10/YYY ABC
Y
Children's
Hospital
Heike XxxxxYyyyy, M.D.
10/10/YYY ABC
Y
Children's
Hospital
Andrew
XXXXXXX,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Thymus, thymectomy: No significant histopathologic abnormality
Heart, native, orthotopic transplant: End stage dilated cardiomyopathy
@ 05:02 AM: X-ray of chest:
Reason for exam: Atelectasis
Impression:
Low lung volumes
Tip of the endotracheal tube is in the mid intrathoracic trachea
Tip of the feeding tube is in the body of the stomach
Right-sided chest tube and drain which traverses the mediastinum with tip
in the left hemithorax remains present
Right internal jugular catheter tip remains in the right internal jugular line
Status post median sternotomy with epicardial pacer wires
@ 08:59 AM: EKG report:
Findings:
Incomplete analysis due to missing data in precordial lead
Sinus rhythm
Normal P-axis, ventricular rate 106-186
Right Ventricular Hypertrophy (RVH), consider LVH
P-R interval = 135 ms
QT interval = 260 ms
QTc interval = 409 ms
@ 09:54 PM: X-ray of abdomen:
Reason for exam: NJ placement. 4-month-old with DCM status post heart
transplant.
Findings: Demonstrates a normal, nonobstructive bowel gas pattern without
evidence of free air. A nasogastric tube can be seen with its tip likely at the
duodenal/jejunal junction. Overlying epicardial leads are seen. The bilateral lung
bases appear to be clear.
@ 00:25 AM: X-ray of abdomen:
Reason for exam: NJ placement. 4-month-old with DCM status post heart
transplant.
Findings: Demonstrates a normal, nonobstructive bowel gas pattern without
evidence of free air or abnormal dilatation. The nasogastric tube is again seen, now
with its tip at the third portion of the duodenum.
@ 01:45 AM: EKG report:
Findings:
Sinus rhythm
Normal P-axis, ventricular rate 106-186
LVH
Extreme leftward forces
48 of 87
BATES Ref
Hospitals &
Clinics_000
33-00034
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
329-01331
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
288
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
306-01307
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
306-01307
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
286
XXXX
XXXX
DATE
PROVIDER
10/10/YYY ABC
Y
Children's
Hospital
Hediah XXX,
M.D.
10/10/YYY ABC
Y
Children’s
Hospital
Megan Xxx,
N.P.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
P-R interval = 136 ms
QT interval = 268 ms
QTc interval = 414 ms
@ 01:08 PM: X-ray of chest:
Reason for exam: Pneumothorax
Impression:
Status post removal of chest tubes with no pneumothorax
Mild cardiomegaly
Interim summary note:
Diagnosis: Asthma, unspecified
Brief identification: 3-month female with dilated cardiomyopathy now status post
heart transplant on 10/05/YYYY.
Hospitalization by system: History reviewed.
Patient received her transplant on 10/05/YYYY. She returned to the CVICU on
Dopamine, Epinephrine, and Milrinone. She had stable hemodynamics. On
Postoperative Day (POD) # 2 her CVP’s started trending up slightly and her liver
was down about 2 cm. An echocardiogram on POD # 1 showed an underfilled RV
with good ventricular function. She also had clot formation around her RA heart
undersized. A repeat echocardiogram on POD #2 showed a better filled RV with
good systolic function. An evaluation of her SVC showed turbulent flow by color
doppler and slight gradient at the anastomosis sight. There was also clot noted
around the RA/SVC. The conclusion was that the clot maybe contributory to the
elevated CVP by pressing on the RA. The CVP is being measured by the right IJ
which on X-ray is proximal to the assumed anastomosis site. Over the next few
days her CVP has trended down. We have been able to wean off her Epinephrine
and Dopamine by POD # 4. We will continue her Milrinone through extubation. It
is important to pass on that at her first biopsy in the catheterization lab that an
assessment of her SVC anastomosis be done.
From a Transplant standpoint she received IVIG and Solumedrol in the Operating
Room (OR). She was started on Extended Release Basiliximab on POD #1 and will
receive her second dose on POD # 5. Her Cyclosporin was started on POD # 2 and
is being adjusted for a goal Cyclosporin level of 300-350. This is to be given
sublingual at all times. She is on her Mycophenolate Mofetil (MMF) and
Ganciclovir and is scheduled for her IVIG on POD # 14. She will have her first
biopsy 4 weeks post transplant.
From a pulmonary standpoint, currently she remains intubated. We have been able
to wean her ventilation for normal oxygenation and over the weekend we initiated 1
hour sprints which she has tolerated. We have a goal extubation date of
10/11/YYYY or 10/12/YYYY. In the course of her critical illness, patient has
developed a dependence on opioids and benzodiazepines.
In the post-operative period she has continued on her scheduled Ativan and
49 of 87
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
327-01329
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
054-00058
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Methadone but has also been on Morphine and Versed GTTs. We have increased
her enteral Ativan and Methadone and are slowly weaning off the GTTs. She has
been awake but consolable as we have done this wean. She had been breastfeeding
prior to admission. She is being supported with TPN while NPO for the extubation
trials.
BATES Ref
We started patient’s enteral feeds on POD # 2 initially NG but on POD # 4 after an
emesis we have advanced her tube to NJ. She is on full volume feeds currently. We
will advance kilocalories once she is extubated. She will need Occupational
Therapy (OT) consultation to re-establish her oral feeds.
10/11/YYY ABC
Y
Children’s
Hospital
XXXYYY,
M.D.
10/12/YYY ABC
Y
Children’s
Hospital
Peter Xxx,
M.D.
10/13/YYY ABC
Y
Children’s
Hospital
XXXYYY,
M.D.
09/10/YYY ABC
YChildren’s
10/13/YYY Hospital
Y
Patient had initially struggled with mild renal insufficiency in the setting of
cardiogenic shock. Her Creatinine has since normalized and she is making good
urine on scheduled doses of enteral Lasix.
X-ray of chest:
Reason for exam: Line placement
Impression: New left PICC line in left mid-subclavian vein.
X-ray of chest:
Reason for exam: Chest expansion
Impression:
Persistently low lung volumes, stable compared to prior exams
Left PICC line in the IJ vein. Would recommend withdraw by at least 2.5
cm, which will place the tip in the distal subclavian vein.
@ 03:25 AM: X-ray of chest:
Reason for exam: Chest expansion
Impression:
Improved aeration bilaterally
Stable cardiomegaly
Nasogastric tube seen with its tip projecting in the jejunum
The left arm PICC line is seen with its tip at the mid-subclavian vein
Labs:
Date
09/10/YY
YY
09/11/YY
YY
09/12/YY
YY
Hgb
(Ref:
10-14
gm/dl)
11.6
Hct
(Ref:
30-42
%)
34
pH
(Ref:
7.357.45)
7.38
10.9
32
10.2
30
44
pO2
(Ref:
80105)
33
25.8
O2
Saturati
on (Ref:
95-98)
62
7.36
46.4
33
26.5
60
7.36
50.5
36
28.4
65
50 of 87
pCO2
(Ref:
35-45)
HCO3
(Ref:
22-26)
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
325-01326
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
323-01325
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
322-01323
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
444-01466
XXXX
XXXX
DATE
PROVIDER
10/13/YYY ABC
Y
Children’s
Hospital
Deborah X,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
28
7.37
57.2
35
09/13/YY
9.5
YY
09/16/YY
10.9
32
YY
09/18/YY
10.2
30
YY
09/19/YY
9.5
28
YY
09/24/YY
9.2
27
YY
09/26/YY
9.5
28
YY
09/30/YY
10.2
30
YY
10/03/YY
9.2
27
YY
10/04/YY
9.2
27
YY
10/05/YY
10.9
32
YY
10/06/YY
10.2
30
YY
10/07/YY
9.2
27
YY
10/08/YY
8.2
24
YY
10/09/YY
9.9
29
YY
10/10/YY
9.9
29
YY
10/11/YY
9.5
28
YY
10/12/YY
9.2
27
YY
10/13/YY
10.5
31
YY
Interim summary note:
BATES Ref
32.7
64
7.28
63.8
25
30.1
62
7.34
52.5
34
28.1
61
7.38
47.7
35
28.4
66
7.38
52.8
32
31.5
60
7.34
58.7
33
31.8
59
7.36
60.8
37
34.2
66
7.42
43.6
27
28.0
51
7.56
35.3
39
31.3
81
7.41
48.0
204
30.7
100
7.44
40.3
129
27.5
99
7.46
33.6
126
24.0
99
7.44
29.8
161
20.3
100
7.48
39.5
164
29.4
100
7.43
47
99
31.4
98
7.42
44.5
146
29.1
99
7.51
38.4
317
30.4
100
7.43
46.9
93
30.8
133
Patient identification: 4-month female status post heart transplant on 10/05/YYYY
secondary to dilated cardiomyopathy.
Hospitalizations by systems: History reviewed.
Cardiovascular: Patient is now hemodynamically stable off all inotropes. Most
recent echocardiogram was on 10/07/YYYY and demonstrated normal biventricular
systolic function. Her SVC anastomosis will need to be monitored by angiogram
and pressure measurement in the course of future surveillance heart
catheterizations. Patient’s current immunosuppression regimen includes
Cyclosporine, CellCept, and Prednisolone. Her target Cyclosporine trough is 300350. Her dose is being adjusted on a daily basis by the transplant team.
51 of 87
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
050-00053
XXXX
XXXX
DATE
PROVIDER
10/14/YYY ABC
Y
Children’s
Hospital
Hediah XXX,
M.D.
10/14/YYY ABC
Y
Children’s
Hospital
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Respiratory: Following her heart transplant, patient had good compliance and gas
exchange on the ventilator. She was extubated on 10/12/YYYY, and is currently
requiring 0.5 L Nasal Cannula (NC), which is being weaned off. Her chest film is
clear, and on exam she has copious upper airway secretions. She receives Xopenex
nebulization and nasal suction every 4th hourly and Chest Physiotherapy (CPT)
every 6th hourly. This regimen can be weaned as she continues to progress.
Neurologic: In the course of her critical illness, patient has developed a dependence
on opioids and benzodiazepines. She has been transitioned from continuous
infusions of Morphine and Versed to enteral Methadone and Ativan within the last
12 hours. Once her dosing is scheduled, a weaning schedule can be initiated.
Fluids/Electrolytes/Nutrition: Patient currently receives NJ continuous feeds.
Occupational Therapy is anticipated to see the patient on 10/13/YYYY for a Patient
Controlled (PC) feeding trial. To maintain euvolemic status, patient receives an
enteral daily dose of Lasix.
Renal: Most recent BUN and Creatinine were <5 and 0.3 respectively. She has no
active Nephrology concerns.
@ 04:15 AM: X-ray of chest:
Reason for exam: Chest expansion
Impression:
Stable postoperative changes and supportive equipment
Mild to moderate cardiomegaly, stable
Clear lungs
@ 10:50 AM: X-ray of abdomen:
Reason for exam: Nasogastric tube placement
Shreyas
Xxxxx, M.D.
10/15/YYY ABC
Y
Children’s
Hospital
Impression: Naso-enteric tube tip projecting over the gastric body.
Shreyas
Xxxxx, M.D.
10/15/YYY ABC
Y
Children’s
Hospital
Impression: Mild cardiomegaly, stable when compared to study dated
10/14/YYYY
@ 10:35 AM: Echocardiogram report:
Daniel Xxxx,
M.D.
10/16/YYY ABC
Y
Children’s
Hospital
@ 08:02 AM: X-ray of chest:
Reason for exam: Lung expansion
Indication: Heart transplant, evaluate function
Summary:
Status post heart transplant operation
Normal LV systolic function
No coarctation of the aorta
Trivial pericardial effusion
Normal aorta
X-ray of chest:
Reason for exam: Atelectasis
52 of 87
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
321-01322
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
305-01306
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
320-01321
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
255-01257
XXXXS_29
7160_rec fm
ABC
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
Shreyas
Xxxxx, M.D.
10/17/YYY ABC
Y
Children’s
Hospital
Heike XxxxxYyyyy, M.D.
10/17/YYY ABC
Y
Children’s
Hospital
OCCURRENCE/TREATMENT
Impression: Mild cardiomegaly, stable when compared to study dated
10/15/YYYY.
@ 08:55 AM: X-ray of chest:
Reason for exam: Chest expansion
Impression: Mild cardiomegaly, stable when compared to study dated
10/16/YYYY. Overall lung aeration is improved when compared to recent prior
imaging.
@ 02:20 PM: Pain Service consultation for opioid and benzodiazepine taper:
History reviewed. In the course of her critical illness, patient has developed a
dependence on opioids and benzodiazepines. She has been transitioned from
Julie Xx, M.D. continuous infusions of Morphine and Versed to enteral Methadone and Ativan on
10/12/YYYY. During the transition she was initially on every 4 hour dosing of both
Methadone and Ativan, then 6 hourly, then returned to 4 hourly as GTT were
completely stopped. She tolerated re-transition to oral yesterday from 0.8 mg IV 4th
hourly of both medications to 0.8 mg Nasogastric (NG) every 4th hourly Ativan and
1 mg NG every 4th hourly of Methadone. Withdrawal Assessment Tool (WAT)
scores remained low over weekend, 0-1 yesterday for mild tremor startle only.
Team would like weaning recommendations and hopefully a schedule which will
allow mother to get more sleep at night. Currently drugs are every 2 hourly
alternating.
Review of systems:
Gastrointestinal: Tolerating feeds, continuous.
Height: 58 cm; Weight: 5.41 kg; BMI: 12.31 kg/m2
Vital signs:
Temperature – 36.7
HR – 136
Cuff BP – 98/55
Respiratory rate – 28
Peripheral pulse rate – 137
Physical examination:
General: No acute distress, smiling.
Lungs: Unlabored. Few course upper airway rhonchi.
Heart: Regular rate and rhythm. Chest wound healing well. No erythema.
Extremities: Warm and well perfused.
Labs:
Parameter
Hemoglobin
Hematocrit
Value
10.0
29.8
53 of 87
Reference range
(Web search)
10-14 gm/dl
30-42%
BATES Ref
Children's
Hospital_01
319-01320
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
318
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
007-00010
XXXX
XXXX
DATE
PROVIDER
10/20/YYY ABC
Y
Children’s
Hospital
Norman
XXXX, M.D.
10/20/YYY ABC
Y
Children’s
Hospital
Stuart Ginn,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Assessment and recommendations: 4-month female status post heart transplant on
10/05/YYYY secondary to dilated cardiomyopathy, opioid and benzodiazepine
dependence. Attempt to transition both medications to every 6 hourly, continue
alternating to prevent excessive sedation with both given together. Ativan 1.2mg
NG every 6 hourly alternating with Methadone 1.3 mg (Represents wean of
between 10-20%) every 6 hourly continue monitoring withdrawal scores. Will write
taper tomorrow if patient does well with this transition.
@ 12:13 PM: Echocardiogram report:
Indication: Status post heart transplant
Summary:
Status post heart transplant operation
Normal LV systolic function
No coarctation of the aorta
No change since prior study
@ 03:09 PM: Pediatric Otolaryngology consultation for hoarseness and
increased work of breathing status post prolonged intubation:
Patient with history of dilated cardiomyopathy who underwent successful heart
transplantation on 10/05/YYYY. Per primary team she had a prolonged intubation
of approximately 9 weeks and was extubated on 10/12/YYYY. Post-extubation she
was initially stridulous with increased secretions but was responsive to Decadron
and racemic Epinephrine doses and was weaned to room air oxygen without
significant difficulty. She has remained hoarse since her extubation per her mother,
who states that her voice/cry were normal and strong prior to her intubation and
subsequent surgery.
Overnight she had increased work of breathing, tachypnea, and some increased
secretions with associated de-saturations into the 80s which was responsive to a
single dose of racemic Epinephrine. She has been stable and breathing quietly today
and maintaining good oxygen saturation levels on room air. She is afebrile and
otherwise appears well and stable. ENT is consulted for evaluation of her upper
airway.
Vital signs:
Temperature – 37.7
HR – 153
Cuff BP – 102/59
Respiratory rate – 32
Peripheral pulse rate – 152
Physical examination:
General: Resting comfortable. No audible stridor or retraction at rest.
Lungs: Mild inspiratory stridor on auscultation. Lung sounds clear. No retractions.
Flexibly Fiberoptic Laryngoscopy: A pediatric flexible laryngoscope was
advanced through the right nasal cavity. Diffuse supraglottic edema noted without
associated erythema. Unable to adequately assess glottis or vocal folds secondary to
54 of 87
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
252-01254
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
003-00006
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
OCCURRENCE/TREATMENT
BATES Ref
supraglottic edema.
Impression: Status post heart transplant with prolonged intubation and subsequent
hoarseness and significant supraglottic edema on examination, likely secondary to
local trauma due to intubation and airway manipulation. Unable to adequately
assess vocal folds/glottis at this time due to edema.
10/21/YYY ABC
Y
Children’s
Hospital
Peter Xxx,
M.D.
10/24/YYY ABC
Y
Children’s
Hospital
Francis
Xxxxx, M.D.
10/28/YYY ABC
Y
Children’s
Hospital
Rajesh Pppp,
M.D.
10/28/YYY ABC
Y
Children’s
Hospital
Recommendations:
Change to Proton Pump Inhibitor (PPI) for better reflux prophylaxis
Decadron 1/2 mg/kg every 8 hourly for 24-48 hours at discretion of primary
team to decrease edema
Recommend racemic Epinephrine as needed
Will follow and plan to repeat flexible laryngoscopy when clinically
improved to re-assess airway
X-ray of chest:
Reason for exam: Chest expansion
Impression: Mild cardiomegaly, stable when compared to study dated
10/17/YYYY. Otherwise, the lung parenchyma is unremarkable without evidence
of focal consolidations or pleural effusions.
X-ray of chest:
Reason for exam: Chest expansion
Impression:
Mild cardiomegaly, stable
Stable low lung volumes
Stable support equipment
Stable postoperative appearance of the chest
@ 08:42 AM: Echocardiogram report:
Indication: Heart transplant, biopsy
Summary:
Directed study to assess pericardial effusion and Tricuspid Regurgitation
(TR)
Status post heart transplant operation
Normal LV systolic function
Trivial TR
@ 05:50 PM: Operative report for micro-direct laryngoscopy and
bronchoscopy:
Pre and postoperative diagnosis: Supraglottic edema; Stridor.
Anna Xxxxx,
M.D.
Procedure: Micro-direct laryngoscopy and bronchoscopy.
Anesthesia: General anesthesia
55 of 87
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
317
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
316-01317
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
250-01251
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
083-00085,
XXXXS_29
7160_rec fm
ABC
XXXX
XXXX
DATE
PROVIDER
10/29/YYY Stanford
Y
Health Care
Gerald XXX,
M.D.
10/31/YYY ABC
Y
Children’s
Hospital
Amanda Xxx,
P.T.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Indications for procedure: The patient is status post cardiac transplant on
10/05/YYYY. She was intubated for about nine weeks. She was noticed to have
post-extubation stridor and with retraction. The previous fiberoptic scope exam
demonstrates supraglottic edema. She has been treated with Decadron and racemic
Epinephrine. It was decided the patient should undergo the micro-direct
laryngoscopy and bronchoscopy before her catheterization lab. The risks, benefits,
and details of procedure were discussed with the patient’s family who agreed to
proceed with the procedure.
Intraoperative findings:
Much improved supraglottic edema. Able to visualize the vocal cords
bilaterally. Difficult to visualize the vocal cords movement due to the
sedation.
Small amount of the granulation tissue at the left posterior vocal process.
Stage II subglottic stenosis.
Normal distal trachea and left and right bronchi.
The size 3 ETT was able to pass easily and the size 3.5 ETT can be passed
though snugly.
Pathology report of right ventricle endomyocardial biopsy:
Diagnosis:
Heart, right ventricle, endomyocardial biopsy: No evidence of acute cellular
rejection (Grade 0).
Physical Therapy (PT) notes for recurrent stridor:
Patient is status post heart transplant secondary to dilated cardiomyopathy.
Recurrent stridor – Found to have subglottic stenosis.
Objective: Worked on developmental activities including visual/social stimulation,
midline play, facilitated kicking, rolling supine to side-lying, hands to knees,
supported sitting and prone.
BATES Ref
Children's
Hospital_00
088-00089
XXXXS_29
6150_rec fm
Stanford
Hospitals &
Clinics_000
44-00045
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
299-01300
Assessment: Patient tolerated session well with stable vital signs. Some stridor
noted following brief cry, however quickly resolved. She did not demonstrate any
visual interaction on faces or toys. Mother reports having observed similar behavior
and has discussed with Dr. Rosenthal. Brings hands to midline and single hand to
mouth. Limited variety of movement outside of these 2 movement patterns.
Decreased quantity and vigor of kicking expected for age with decreased abdominal
activation. Attempts to hold head erect in supported sitting with decreased head and
neck control for age. Tolerated prone well, remained sucking on finger throughout
with head in left rotation. Delayed prone skills. No attempts at lifting head with
primitive shoulder girdle noted.
08/21/YYY ABC
YChildren’s
10/31/YYY Hospital
Y
Plan: 2-3 times/week throughout hospitalization.
Labs:
Date
Hgb (Ref: 1014 gm/dl)
Hct (Ref:
30-42 %)
56 of 87
WBC (Ref:
5.0-9.5 K/uL)
Platelets (Ref:
150-400 K/uL)
XXXXS_29
7160_rec fm
ABC
Children's
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
11/01/YYY ABC
Y
Children’s
Hospital
Sandra
Xxxxx,
O.T.D.
OCCURRENCE/TREATMENT
29.8
12.5
10/17/YYY 10.0
Y
10/24/YYY 11.2
33.9
3.5
Y
10/31/YYY 11.7
34.2
7.7
Y
Occupational Therapy (OT) notes for recurrent stridor:
458
BATES Ref
Hospital_01
402-01407
383
363
Patient with recurrent stridor status post heart transplant – Found to have subglottic
stenosis.
Objective: Patient positioned semi-upright in tumble-form seat, blanket roll placed
under shoulders to improve positioning for airway. Educated Registered Nurse
(RN) and Medical Officer on Call (MOC) on safety precautions when using tumbleform seat in crib.
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
295-01296
In addition, patient remains not appropriate for oral feeding at this time due to her
respiratory/airway status. Will defer to Physician teams regarding when patient will
be appropriate for oral feeding trials.
Assessment: Continue to follow and provide support regarding patient’s
developmental needs.
11/01/YYY ABC
Y
Children’s
Hospital
Amanda Xxx,
P.T.
11/02/YYY ABC
Y
Children’s
Hospital
Peter Xxx,
M.D.
11/04/YYY ABC
Y
Children’s
Hospital
Hediah XXX,
M.D.
08/21/YYY ABC
YChildren’s
11/04/YYY Hospital
Y
Plan: 2-3 times a week, throughout hospitalization.
Physical Therapy notes status post heart transplantation:
Patient fitted in tumble-form for upright sitting to assist with stridor. Small blanket
roll placed for slight neck extension.
Assessment: Good fit in chair. Mother educated on use.
Plan: 2-3 times week throughout hospitalization.
X-ray of abdomen:
Reason for exam: NG tube placement
Impression: NG tube remains in place in the distal stomach.
X-ray of chest:
Reason for exam: Pulmonary edema
Impression:
Mild cardiomegaly, stable
Bilateral low lung volumes, stable. No significant pulmonary edema.
Hospitalization records: Wound care report, laboratory reports, surgery log
information, consent forms, Nursing staff’s name, assessment, orders, authorization
forms, flow sheets, requisition forms, case management forms, medication
administration records, input/output records:
57 of 87
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
297-01298
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
304
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_01
314-01315
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
OCCURRENCE/TREATMENT
BATES Ref
BATES Ref: XXXXS_295867_rec fm UCD_00007-00100, XXXXS_296150_rec fm
Stanford Hospitals & Clinics_00004-00007, 00009-00011, 00040-00043, 0004600092, XXXXS_296150_296154_rec fm XXYY Valley Health CTR_00211-00212,
XXXXS_297160_rec fm ABC Children's Hospital_00037-00049, 00095-01249,
01294, 01301-01303, 01408-01443, 01467-03208, 03210-03600, 03606-03970,
04005-04809
11/04/YYY ABC
Y
Children’s
Hospital
David XXXX,
M.D.
Rajesh Pppp,
M.D.
Palau XXX,
M.D.
*Reviewer's comment: Hospitalization records have been combined and not
elaborated.
Discharge summary:
Admit Date:
Length of hospital stay:
*Reviewer's comment: After extended period of hospitalization for a period of 2
months and 15 days, here we note that baby Sophia was discharged home with NG
feeds and supplies on 11/04/YYYY.
Admitting diagnosis: Cardiogenic shock
Principal diagnosis: Dilated cardiomyopathy
Secondary diagnoses:
Airway obstruction
Asthma, unspecified
Constipation
Gastritis
Heart transplant
Sedative dependence
Stridor inspiratory
Principal operations and procedures:
Orthotopic heart transplant (10/05/YYYY)
Extubated 10/12/YYYY
Immunosuppression
Direct laryngoscopy and bronchoscopy
Consulting services: Cardiac Transplant, Nutrition, OT, Physical Therapy,
ENT, Pain
Hospital course: Patient admitted on 08/21/YYYY for cardiogenic shock. Her
echocardiogram revealed DCM with poor LV function. She underwent heart
transplant on 10/05/YYYY. She returned from the OR on inotropes. She was
monitored closely for evidence RV failure, which did not materialize. She is now
hemodynamically stable off all inotropes. Most recent echocardiogram was on
10/15/YYYY and demonstrated normal biventricular systolic function with trace
Mitral Regurgitation (MR) and TR. Her SVC anastomosis will need to be
monitored by angio and pressure measurement in the course of future surveillance
58 of 87
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_00
030-00036
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
heart catheterizations. She was started on Diltiazem 2.7mg NG twice daily for
coronary artery protection and Amlodipine 0.6mg daily for goal systolic BPs 90100, which she has maintained. Last echocardiogram on 10/28/YYYY was normal.
Continue Diltiazem 2.7 mg twice daily for Graft Coronary Artery Disease (GCAD)
prophylaxis. Continue Amlodipine 0.6 mg daily and Lasix NG twice daily.
Immunosuppression: Patient’s current immunosuppression regimen includes
Cyclosporine, CellCept, and Prednisolone.
Respiratory: Following her heart transplant, patient had good compliance and gas
exchange on the ventilator. She was extubated on 10/12/YYYY with 24 hour of
Decadron. Post-extubation she required aggressive respiratory treatment support
with deep suctioning, Citalopram (CTP) and Albuterol due to respiratory muscle
weakness from prolonged intubation. These treatments were able to be weaned by
10/18/YYYY. Overnight 10/19/YYYY she developed stridor and some increased
WOB which improved with racemic Epinephrine. She was evaluated by ENT on
10/20/YYYY and was found to have significant supraglottic swelling over her
arytenoid cartilage and subglottic stenosis, likely secondary to local trauma due to
intubation and airway manipulation. She was started on Decadron 0.5mg/kg every 8
hourly for 48 hrs with every 2 hourly as needed racemic Epinephrine. Her Zantac
was switched to PPI Omeprazole for treatment of possible reflux. Overnight
10/20/YYYY she continued to require racemic Epinephrine and by 10/21/YYYY
due to continued stridor, increased WOB (RR in 60’s), retractions, flaring, and less
response to racemic Epinephrine, it was decided to transfer her to the Pediatric
Intensive Care Unit (PICU) for escalation of care. She has not required oxygen, as
she maintains her saturations greater than 95% despite having stridor. She is on
inhaled corticosteroids. ENT evaluation on 10/28/YYYY showing improved
supraglottic edema and normal vocal cord motility, still with mild subglottic
stenosis. She was not a candidate for dilatation, and any potential intervention
would be an open surgery. Family and team would like to avoid surgical
intervention if possible. Clinically her stridor was resolving and was transferred
back to floor on 11/02/YYYY
Neurologic: In the course of her critical illness, patient has developed a dependence
on opioids and benzodiazepines. She currently receives enteral Methadone and
Ativan, which are being weaned in accordance with a schedule.
Nutrition/Gastrointestinal: Patient was fed NJ continuously until stable from a
respiratory perspective. Occupational Therapy had been working with her for PC
feeding trials and oral stimulation. Currently on NG feeds with MBM when
available or Enfamil 28kcal/oz at goal of 32 ml/hr for 130 kcal/kg/day. Patient
started on Magnesium and Sodium chloride supplementation. Currently on Lasix
twice daily and Omeprazole for reflux symptoms.
Heme: She was anemic and has been on Epogen and iro– - last Hct 34 on
10/31/YYYY. Will discontinue Epogen on discharge. Continue iron.
Infectious Disease: In the course of her hospitalization, patient has not had any
positive blood or urine cultures. She was not tolerating inhaled Amphotericin, so it
was changed to Voriconazole. She has been afebrile. She continues on Valcyte,
Bactrim, Voriconazole and Nystatin for prophylaxis against opportunistic infection.
She also is receiving CytoGam every 2 weeks (Given 10/21/YYYY and
11/04/YYYY).
Social/Other: Psychiatry team was seeing mother during hospitalization and
diagnosed with anxiety and team recommended Zoloft for mother.
59 of 87
BATES Ref
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
OCCURRENCE/TREATMENT
BATES Ref
Discharge vital signs:
Temperature – 36.5°C
HR – 151
Cuff BP – 92/58
Respiratory rate – 24
Physical examination:
General: No acute distress, playful and vigorous.
Cardiac: Normal S1, physiologic split S2. No murmur.
Extremities: Warm. No edema. Capillary refill time <2 sec. Pulses – 2+/4. No
radio-femoral delay.
Disposition: Short Stay Unit (SSU) on 11/07/YYYY for Cyclosporine A (CSA)
level. Plan to send home with PICC for weekly lab draws – starting 11/09/YYYY
SSU. Discharged home with NG feeds and supplies.
Feeds upon discharge: Breast milk, formula, tube feeding.
11/09/YYY ABC
Y
Children’s
Hospital
Daniel
Xxxxyyyy,
M.D.
Follow-up care: Weekly lab draws, echocardiograms, transplant visits on
Wednesdays, starting 11/09/YYYY. CSA level at short stay on 11/07/YYYY.
Follow-up visit status post orthotopic heart transplantation:
Patient presented for her first outpatient clinic visit for follow-up and non-invasive
evaluation for allograft rejection. The last cardiac biopsy was done on 10/28/YYYY
that showed no evidence of rejection. The first coronary angiogram will be
performed at 1 year post-transplant.
Review of systems:
Constitutional: No fevers, but overall vague discomfort, relieved by Tylenol.
Mother is administering Tylenol every 6 hours for the past 2 days for what seems
like pain associated with changing positions and moving her legs.
HEENT: Slight cough and positional stridor, but mother has found sleeping
positions for patient that minimize any stridor.
Respiratory: No wheezing or increased work of breathing noted
Gastrointestinal: Emesis times 1 two days ago, thought to be associated with
giving medications via NG too close together. She has been getting MiraLax, and
has stooled large amounts with no increase in frequency.
Neurologic: Mother has been managing the Ativan/Methadone taper schedule, and
has had to hold some of the weans based on some withdrawal symptoms.
Interval history: Since discharge, patient has not had any symptoms referable to
the cardiovascular system.
Diet: NG tube fed with Enfamil 28 kcal/oz at a continuous rate of 32 cc/hr.
Tolerating feeds fine.
Vital signs:
Temperature – 36.7
HR – 166
60 of 87
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00240
-00244
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
OCCURRENCE/TREATMENT
BATES Ref
Cuff BP – 98/59
Respiratory rate – 36
Physical examination:
ENT: Small whitish region to left buccal mucosa.
Respiratory: Positional stridor only when sitting more upright.
Cardiovascular: Tachycardic rate to 160 while calm.
Echocardiogram report:
No significant valve regurgitation
Status post heart transplant
Normal LV systolic function
Fractional shortening – 34%
Labs:
Parameter
Hemoglobin
Hematocrit
WBC
Platelets
Cyclosporine level
11/16/YYY ABC
Y
Children’s
Hospital
Value
13.4
39.8
9.5
541
270
Reference range
(Web search)
10-14 gm/dl
30-42%
5-19.5 K/uL
150-400K/uL
300-350 ng/ml
Assessment and plan: Status post heart transplantation. From a clinical standpoint,
patient has subglottic stenosis but appears well and shows no signs or symptoms
suggestive of allograft rejection.
With a 14 hour trough cyclosporine level of 270 ng/mL and a goal level of
300-350 ng/mL, patient’s cyclosporine is close to within range, particularly
with her recent unstable, supratherapeutic levels. We will make no changes
to her dose at this time and recheck another level in 1 week.
To protect against graft coronary artery disease, we would like to initiate
Lipitor at 1mg once daily.
Valcyte should be at once daily administration.
Return to clinic in 1 week, 11/16/YYYY. Cardiac biopsy on 11/28/YYYY.
We will evaluate her SVC gradient with the next biopsy with pressures and
angiogram. CytoGam: 11/18/YYYY.
Patient’s heart rate is elevated today, but her echocardiogram shows normal
systolic function and she has been afebrile. It is possible that her heart rate
may be elevated if she is in pain, but we have encouraged mother to call us
for persistent heart rates above the 160s while calm/at rest, or for any other
concerns.
Follow-up Hospital Care @ ABC Children’s Hospital
*Reviewer's comment: Per the forthcoming follow-up visits, we note that baby
Sophia after an extended period of hospitalization for her cardiac issues consulted
various specialist such as Pediatric Otolaryngology, Pediatric cardiology,
Pediatric Gastroenterology, Infectious Disease etc.. as elaborated below.
Follow-up visit status post orthotopic heart transplantation:
Since discharge, patient has not had any symptoms referable to the cardiovascular
61 of 87
XXXXS_29
6150_29615
4_rec fm
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
OCCURRENCE/TREATMENT
system.
David XXXX,
M.D.
Donna Xxxx,
C.P.N.P.
Review of systems:
Constitutional: No fevers, but overall vague discomfort ongoing, worse in the
mornings, improved with Tylenol. Otherwise, sleeping through the night
HEENT: Positional stridor.
Respiratory: No wheezing or increased work of breathing noted.
Gastrointestinal: Tolerating feeds fine, with no emesis. Stooling less frequently
with large, “blowout” stools, sometimes seedy and mostly greenish in color.
Appeared slightly more comfortable after Omeprazole administration this morning,
and after having held the feeds a few times this morning.
Neurologic: Mild hand tremor noted. Mother has been managing the
Ativan/Methadone taper schedule
Skin: Appears more flush/pink to the face and extremities, but no obvious rash.
Slight redness noted above insertion site of the PICC.
Hematologic: PICC line unable to draw and sluggish in drawing this morning unable to obtain labs.
Vital signs:
Temperature – 36.3
HR – 150
Cuff BP – 113/85
Respiratory rate – 32
Physical examination:
Respiratory: Positional stridor only when sitting more upright.
Cardiovascular: Tachycardic rate to 145 while calm.
Echocardiogram report:
Hyperdynamic LV systolic function.
No coarctation of the aorta.
Trivial pulmonary valve stenosis.
Fractional shortening of 39%.
Assessment and plan: Patient is status post heart transplantation who is returning
for routine follow-up. From a clinical standpoint, patient shows no signs or
symptoms suggestive of allograft rejection but does have an elevated HR at rest
with no clear cause.
We will consider an EKG and a Holter monitor to further evaluate her
tachycardia.
Dr. Rosenthal discussed a referral to Gastroenterology to evaluate for the
possibility of a G-tube, as patient currently is not eating by mouth and is
NG tube dependent. Patient will meet with ENT this week for follow-up for
her subglottic stenosis, and further discussion will take place regarding the
possibility of safely eating by mouth.
Based on mother’s report of patient’s increased comfort following
Omeprazole administration, we will increase her Omeprazole to 8 mg twice
daily and reassess.
Return to clinic in 1 week
62 of 87
BATES Ref
XXYY
Valley
Health
CTR_00235
-00239
XXXX
XXXX
DATE
PROVIDER
11/18/YYY ABC
Y
Children’s
Hospital
Anna Xxxxx,
M.D.
Suzanne
Ppppp, M.S.,
PA-C
DOB: 03/22/YYYY
DOB: 06/07/YYYY
BATES Ref
OCCURRENCE/TREATMENT
Cardiac biopsy: 11/28/YYYY. We would like to re-evaluate patient’s SVC
anastomosis at that time.
CytoGam at 100mg/kg tomorrow, 11/17/YYYY, in the Short Stay Unit.
XXXXS_29
Pediatric Otolaryngology consultation for subglottic stenosis:
6150_29615
The patient is status post heart transplantation. Mother states that the patient has
4_rec fm
been stable from a respiratory standpoint. She denies any increased work of
XXYY
breathing or significant stridor. The patient has had weeks of irritability and “a very Valley
red face.” She was given Benadryl and the redness of her face resolved and her
Health
heart rate came down from 160/170 to 120. The patient is currently receiving 100% CTR_00232
of her nutrition through a nasogastric tube.
-00234
Physical examination:
Nose: A nasogastric tube is present on the left side.
Neck: No stridor or retractions.
Chest: There are multiple leads overlying her left chest monitoring her heart rate.
Procedure: Following appropriate preparation, a flexible laryngoscopy was
performed through the right naris. This illustrated a normal nasal passage with
patent choana. The nasopharynx and oropharynx were normal. The larynx was
notable for significantly redundant aryepiglottic folds with resultant hooding of the
arytenoids. The true vocal cords were not visible.
11/20/YYY ABC
Y
Children’s
Hospital
David XXXX,
M.D.
Donna Xxxx,
C.P.N.P.
Assessment and plan: Patient with a history of cardiac transplant secondary to
dilated cardiomyopathy. She was also diagnosed with subglottic stenosis
intraoperatively back in October. From an airway standpoint, she appears to be
doing quite well. She is stable without any respiratory distress. Dr. Messner
explained that the goal is to get her feeding orally. Therefore, the patient will be
scheduled for a modified barium swallow. The requisition will be processed today.
Additionally, she will be scheduled for a behavioral audiogram in the next couple of
months seeing as though the patient never had a newborn hearing screen. She will
return to clinic in four weeks for reevaluation.
Addendum report for CytoGam infusion:
I (Dr. Rosenthal) saw the patient during her visit for her CytoGam infusion in the
Short Stay Unit. After successfully using Tissue Plasminogen Activator (TPA) to
clear the patient’s line, a Complete Blood Count revealed an elevated platelet count
of 659,000. Thus, we would like to initiate 40 mg of Aspirin daily for now and will
continue to monitor her platelet count.
Due to an elevated heart rate of 162, an EKG revealed sinus tachycardia, and a
Holter monitor was placed on the patient. We will follow up with the results of the
Holter when they are available.
Following Diphenhydramine administration as a scheduled pre-medication before
CytoGam, patient’s facial flushing disappeared and her heart rate decreased to the
high 120s, increasing our suspicion that perhaps she has a medication allergy which
may be contributing to her vague discomfort over the past two weeks. Due to
mother’s history of being severely allergic to Bactrim, we will hold the patient’s
63 of 87
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00238
-00239
XXXX
XXXX
DATE
PROVIDER
11/23/YYY ABC
Y
Children’s
Hospital
Daniel
Xxxxyyyy,
M.D.
Donna Xxxx,
C.P.N.P.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Bactrim at this time and see if her discomfort improves. If the discontinuation of
Bactrim is necessary, we will initiate inhaled Pentamidine monthly as an alternative
for Pneumocystis Carinii Pneumonia (PCP) prophylaxis while she is on Prednisone
during the first year post-transplant.
Follow-up visit status post orthotopic heart transplantation:
Since discontinuing her Septra for a suspected allergy, patient has not required
Tylenol as needed for discomfort, she appears less flushed, and her heart rate has
improved somewhat.
Review of systems:
HEENT: Sleeping well with only occasional positional stridor. Voice stronger.
Respiratory: No increased work of breathing. Slight snoring noted.
Gastrointestinal: Tolerating feeds well. Taking MiraLax as needed for regular
stooling. Emesis times 1 related to gagging.
Hematologic/lymphatic: Platelets high, on ASA 40 mg daily. PICC line not
drawing blood.
Skin: PICC to left upper arm.
Vital signs:
Temperature – 36.6
HR – 137
Cuff BP – 81/69
Respiratory rate – 26
Physical examination:
Cardiovascular: Heart rate 138 while calm.
Abdomen: Liver 1 cm below costal margin.
Echocardiogram report:
Trace tricuspid valve regurgitation
No mitral or aortic valve regurgitation
No left ventricular outflow tract obstruction
No pulmonary valve stenosis or regurgitation
Normal left ventricular size and systolic function
No pericardial effusion
Fractional shortening: 35%
Holter monitor report:
Sinus rhythm with normal blunted circadian pattern and activity related
heart rate variability
No atrial ectopy
No ventricular ectopy
Tachycardia throughout day
Labs:
Parameter
Value
64 of 87
Reference range
(Web search)
BATES Ref
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00221
-00225
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
Hemoglobin
Hematocrit
WBC
Platelets
Cyclosporine level
11/28/YYY ABC
Y
Children’s
Hospital
Daniel
Xxxxyyyy,
M.D.
Donna Xxxx,
C.P.N.P.
OCCURRENCE/TREATMENT
12.5
10-14 gm/dl
37.1
30-42%
7.3
5-19.5 K/uL
588
150-400K/uL
407
300-350 ng/ml
Assessment and plan: Patient is status post heart transplantation. From a clinical
standpoint, patient is now 7 weeks post-transplant and shows no signs or symptoms
suggestive of allograft rejection.
With a trough Cyclosporine level of 407 ng/mL and a goal level of 300350, we will hold tonight’s dose and reduce her dosing to 20 mg in the
morning, 25 mg in the evening. We will recheck another CSA level with
her cardiac biopsy on Monday.
We will discontinue her Voriconazole.
We will keep patient off Septra, and re-evaluate whether she can tolerate
the medication in a few months. In the meantime, we will arrange for
monthly inhaled Pentamidine for PCP prophylaxis as an alternative to daily
Septra administration.
Swallow study: 12/08/YYYY
Return to clinic: 1 week
Cardiac biopsy: On 11/28/YYYY. We will re-evaluate patient’s SVC at that
time. She will receive CytoGam after the biopsy for Cytomegalovirus
(CMV) prophylaxis.
Since patient’s PICC line is not drawing and has already required TPA, the
risks of infection and other complications outweigh the lines benefits of
more easily obtained laboratory draws. Thus, after next week’s CytoGam
infusion, we will discontinue her PICC line.
Follow-up visit status post orthotopic heart transplantation for cardiac biopsy:
BATES Ref
XXXXS_29
6150_29615
Patient is scheduled a cardiac biopsy to evaluate for allograft rejection. She will also 4_rec fm
get CytoGam after her biopsy today.
XXYY
Valley
Interval history: Since the last clinical encounter on Wednesday, 11/23/YYYY,
Health
patient began crying inconsolably on Thursday night and awoke throughout the
CTR_00226
night with irritability. She then had emesis on 11/25/YYYY, which prompted the
-00231
parents to bring her to the Emergency Department (ED) that afternoon. (ED records
are not available for review). Patient was evaluated in the ED for possible pain
related to starting Lipitor or feeding intolerance, was assessed for rhabdomyolysis,
and found to have a Creatine Kinase (CK) within normal limits of 76 units/L. She
was thought to be cardiovascularly stable, and was subsequently discharged.
The following day, she developed diarrhea and more emesis, but no fever. She also
began coughing and sneezing, but had no congestion, after which mother thought
about withdrawal symptoms. Of note, mother had been supplementing patient with
MBM, approximately 30-40 mL/day for the past several weeks, which was
discontinued on Wednesday. Mother notes that she has been on Xanax
(Alprazolam), but as recommended, was pumping and dumping her milk for the 12
hours after medication administration. However, it is possible patient was receiving
some residual Benzodiazepine exposure via MBM, which was stopped Wednesday.
65 of 87
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Mother then gave an increased dose of Ativan at 0.2mg (0.1 mL) on 11/26/YYYY
at 5 pm to see if her symptoms would improve, followed by her regularly scheduled
dose of 0.1 mg (or 0.05 mL) at 8 pm. On 11/27/YYYY at 2 am and 8 am, she
received 0.2 mg (0.1 mL), and then at 2 pm, received 0.3 mg (0.15 mL) for ongoing
diarrhea and irritability. Patient continued to have symptoms of sweatiness, shaking,
and sneezing. On 11/27/YYYY at 8 pm and 11/28/YYYY at 2 am, patient received
0.4 mg (or 0.2 mL) of Ativan, with an improvement noted in her symptoms, as she
finally slept and appeared more comfortable.
Review of systems:
Constitutional: Irritability and fussiness, not sleeping at night, which started
Thursday evening. Afebrile.
HEENT: Positional stridor. Sneezing and coughing but no mucus.
Respiratory: No increased work of breathing.
Gastrointestinal: Emesis and diarrhea starting Friday. Of note, patient appeared
more comfortable last night, which may be related to receiving Pedialyte instead of
Enfamil in preparation for biopsy today.
Hematologic/lymphatic: Platelets high, on ASA 40 mg daily. PICC line not
drawing blood, will be discontinued after infusion today.
Skin: PICC to left upper arm, to be discontinued today after the CytoGam infusion.
Height: 62 cm; Weight: 5.9 kg; BMI: 15.35 kg/m2
Vital signs:
Temperature – 37.6
HR – 137
Cuff BP – 103/52
Respiratory rate – 28
Physical examination:
Cardiovascular: HR 135 while calm.
Abdomen: Liver 1 cm below costal margin.
Echocardiogram with biopsy: Showed no pericardial effusion.
Biopsy results: No evidence of rejection, grade 0.
3 mmHg mean gradient across the SVC.
Labs:
Parameter
Hemoglobin
Hematocrit
WBC
Cyclosporine level
Value
10.7
31.0
4.8
199
Reference range
(Web search)
10-14 gm/dl
30-42%
5-19.5 K/uL
300-350 ng/ml
Assessment and plan: Patient is status post heart transplantation who is returning
for her scheduled monthly cardiac biopsy and for a CytoGam infusion. From a
clinical standpoint, patient is now 8 weeks post-transplant and shows no signs or
66 of 87
BATES Ref
XXXX
XXXX
DATE
PROVIDER
11/30/YYY ABC
Y
Children’s
Hospital
David XXXX,
M.D.
Seth XXX,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
symptoms suggestive of allograft rejection, but with possible feeding intolerance
and withdrawal symptoms.
With a trough cyclosporine level of 199 ng/mL and a goal level of 300-350,
would like to increase her dose to 25 mg twice a day. We will recheck
another CSA level on Friday.
I have consulted with the Pain Team, and have written a new taper schedule
based on their recommendations and patient’s current opioid doses.
We will keep patient off Septra, and re-evaluate whether she can tolerate
the medication in a few months. In the meantime, she will receive inhaled
Pentamidine for PCP prophylaxis as an alternative to daily Septra
administration, to begin 11/29/YYYY.
Swallow study: 12/08/YYYY
Return to clinic: Wednesday 11/30/YYYY, then in 1 week.
Cardiac biopsy on 12/28/YYYY.
Okay to switch to Similac 28 kcal/oz, to continue at same continuous NGT
rate of 32 cc/hr.
I have stressed the importance of notifying our Cardiology Team regarding
any concerns or changes in patient’s condition.
BATES Ref
Follow-up visit status post orthotopic heart transplantation:
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00217
-00220
Interval history: Since the last clinical encounter, she is much improved. She had
experienced several days of withdrawal symptoms for which the parents gave extra
Ativan with improvement in symptoms. They have since contacted the Pain Service
who altered her Methadone and Ativan taper. She is still experiencing fussiness and
diarrhea, however, much improved over last week. Symptoms are also reported to
have improved after changing from Enfamil to Similac.
Vital signs:
Temperature – 36.6
HR – 160
Cuff BP – 105/62
Respiratory rate – 32
Physical examination:
ENT/Mouth: Mild gingival hypertrophy.
Cardiovascular: Regular rate and rhythm. Normal perfusion.
Assessment and plan:
Based on the physical examination and laboratory studies, there is no
evidence to suggest for allograft rejection.
The goal CSA level is 300-350 ng/mL and thus the dose remains
unchanged. Repeat drug levels will be performed in 2 days.
Next cardiac biopsy: 12/28/YYYY
Pentamidine 12/17/YYYY.
12/08/YYYY - Swallow study for evaluation for initiation of oral feeds.
Two doses of CytoGam left (Approximately weeks 12 and 16.)
Return to clinic in 2 weeks.
67 of 87
XXXX
XXXX
DATE
PROVIDER
12/12/YYY ABC
Y
Children’s
Hospital
Sarah Xxxxx,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Will consider re-starting Clonidine #1 patch at next visit if BPs still
elevated. Family to call Pain Team to address ongoing withdrawal signs.
Correspondence to Dr. XX regarding gastrotomy tube placement:
Patient is status post heart transplantation. She has not had any oral feeds since her
admission to the hospital on 08/21/YYYY. There, she was fed by NJ and then NG
feeds with Enfamil 28kcal/oz at 32 mL per hour, which she tolerated well in the
hospital and after discharge.
About 2 weeks ago, patient pulled out her NG tube at home and mother replaced it.
At that time she started having increased emesis, which was non-bloody and nonbilious, about six times a day. She was evaluated by CT on 12/08/YYYY, at which
time her NG tube was replaced with improvement in her vomiting, but it did not
completely resolve. (CT scan report not available for review). Patient has had only
4 episodes of emesis since the CT visit, but continues to have gagging.
In response to patient’s emesis and gagging, her mother reduced her feeds first to 29
mL an hour then to 25 and now since a > 1 cup emesis last night, to 22 mL per hour.
The vomiting does not happen at a particular time of day. Mother only associates it
with the removal of the NG tube, but also notes that the week prior to her emesis,
ENT suggested changing her formula from Enfamil to Similac due to evidence of
reflux on their scope study. Mother reports that patient does seem interested in
tastes of apple sauce on her lips and also interested in watching her mother when
her mother is eating.
At the CT visit 1 mL feeds placed on her tongue were attempted. She did accept
two good swallows without any coughing and then gagged on another 1 mL feed, so
the evaluation was stopped. It was noted that she seemed fatigued and did not have
any signs of feeding readiness, also did not note any functional nutritive suck. CT
recommended giving tastes on lips of thick pureed food a few times a day, which
Mother has been doing. They also recommended a swallow study when she has
improved ability to feed and less aversion to food.
Review of systems: She has recently had increased blood pressure that is thought to
be due to her Prednisolone and she was started on a Clonidine patch as of yesterday
12/11/YYYY. There was concern for tachycardia as well, and she had 24 hour
ambulatory heart rate monitoring where her average was 135; no intervention was
taken. Due to her Methadone taper she has had diarrhea, this has recently been
improving. She normally has two to three stools a day and about 10 urine diapers.
Physical examination:
HEENT: NG is placed.
Cardiovascular/Pulmonary: No stridor appreciated. Heart is regular rate and
rhythm with no murmurs, rubs, or gallops.
Skin: Well healed surgical scars on chest. No rashes.
Assessment and recommendations: Patient who has had a long course of NJ/NG
feeding since August, YYYY, before her heart transplant, who also has a diagnosis
of improving subglottic stenosis. She presented today to be evaluated for inability to
68 of 87
BATES Ref
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00213
-00216
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
tolerate her NG feeds during the last two and a half weeks and evaluation for
gastrostomy tube placement. Despite the increased vomiting, she is well-appearing
and well-hydrated.
*Reviewer's comment: We also note baby Sophia’s critical condition of a long
course of NJ/NG feeding since August, YYYY even before her heart transplant and
also of having a diagnosis of subglottic stenosis (Subglottic stenosis (SGS) is a
narrowing of the subglottic airway, which is housed in the cricoid cartilage).
BATES Ref
Vomiting: It will be very important to determine the cause of the increased
vomiting of late. This could be due to tube placement, esophageal irritation,
Methadone taper, mechanical difficulty with swallowing coordination,
Gastroesophageal Reflux Disease (GERD) or gastric motility. It is also important
for her to continue getting enough calories to grow. To check of the formula is too
concentrated for her stomach we will first attempt to change from 28 kcals/ounce to
25 kcals/ounce formula and increase her volume slowly to achieve the same amount
of calories per day. She will meet with the Dietician today to help talk about how to
mix and increase her NG feeds.
She is encouraged to continue with her swallow study that is currently scheduled for
12/22/YYYY. If the swallow study is abnormal, we may get an upper GI study or
gastric emptying study before proceeding with gastrostomy tube placement. If
patient is able to tolerate sufficient calorie intake through the first interventions
(Less concentrated or thinner formula), and is also showing signs of decreased food
aversion, we may recommend keeping her on NG tube feeds until she is able to
tolerate all of her feeding by mouth.
12/21/YYY ABC
Y
Children’s
Hospital
Anna Xxxxx,
M.D.
Crowley
Xxxx, PA-C
*Reviewer's comment: Swallow study reports are not available for review.
Pediatric Otolaryngology consultation for supraglottic edema and stridor:
Mother states that the patient has been stable from a respiratory standpoint. The
patient has had negative cardiac biopsies thus far, indicating no rejection. At her last
visit on 11/18/YYYY, she was recommended to undergo a modified barium
swallow seeing as Dr. Messner was enthusiastic about getting her to feed orally.
However, she was seen by Occupational Therapy on 12/15/YYYY, who
recommended she postpone the modified barium swallow seeing as she was taking
such minimal amounts orally. (OT records not available for review).
Mother states that she continues to have OT sessions twice per week. Mother
herself is also placing solid foods on her lips so that she can at least taste them. At
this point in time, her modified barium swallow scheduled for 01/18/YYYY.
Review of systems: Positive for eating and feeding difficulties and sleep
disturbance.
Physical examination:
General: Patient is breathing quietly at rest.
Ears: The left external auditory canal is patent, though the tympanic membrane is
not readily visible. The right external auditory canal reveals nonocclusive wax.
Nose: A nasogastric tube is present on the right side.
69 of 87
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00205
-00207
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
12/23/YYY Gene
Y
Diagnosis
OCCURRENCE/TREATMENT
Assessment and plan: Patient carries the diagnosis of grade 2 subglottic stenosis
which was diagnosed intraoperatively back in October. She continues to be quite
stable from a respiratory standpoint. The goal is to get her feeding orally, however it
is quite possible that she will need a gastrostomy tube in the meantime, seeing as
though the transition to oral feeding will probably be slow. The patient was also
recommended to undergo an audiogram. This can hopefully be reviewed at the next
visit. Lastly, Dr. Messner explained that if, in fact, the patient goes under anesthesia
for gastrostomy tube placement, Dr. Messner would like to coordinate a microdirect laryngoscopy and bronchoscopy in the same sitting in order to evaluate the
status of her airway.
Cardiology genetics report:
Diagnosis: Dilated cardiomyopathy
Nizar Xxx,
M.D.
Result: No disease causing mutation was detected.
BATES Ref
XXXXS_29
7160_rec fm
ABC
Children's
Hospital_03
604-03605
Jackie
Tahiliani,
M.S., C.G.C.
12/28/YYY ABC
Y
Children’s
Hospital
David XXXX,
M.D.
Donna Xxxx,
C.P.N.P.
Follow-up visit status post heart transplantation:
Since last encounter, the parents have noted that her feet appear slightly cooler and
sweaty at times. Her legs appear more full, and her skin folds around her wrists and
thighs have subsided. Of note, she has gained weight since the last visit.
Review of systems:
Constitutional: For approximately one week, mother reports patient appears more
“puffy” in her extremities. Afebrile. Off Ativan for 3 weeks.
HEENT: Ongoing occasional sneezing and coughing since withdrawal symptoms
began.
Gastrointestinal: Sensitive gag reflex. Yesterday had emesis of milky/mucousy
fluid times 4, otherwise has been averaging 1- 2 episodes of emesis a day, not
specifically related to medication administration.
Skin: Some residual marks from frequent blood pressure checks in her lower legs;
hirsutism to back, face.
Height: 63.5 cm; Weight: 6.45 kg; BMI: 15.99 kg/m2
Vital signs:
HR – 146
Cuff BP – 102/59
Respiratory rate – 34
Physical examination:
Constitutional: Anterior fontanelle flat
Cardiovascular: Tachycardic rate, regular rhythm.
Skin: Hirsutism. Healing areas of erythema to legs bilaterally.
70 of 87
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00200
-00204
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
OCCURRENCE/TREATMENT
BATES Ref
Echocardiogram report:
No significant atrioventricular valve regurgitation
No left ventricular outflow obstruction
No aortic valve regurgitation
Mild color flow acceleration across the right SVC, not Doppler interrogated
today.
Qualitatively hypertrophied LV with normal systolic function
No pericardial effusion.
Fractional shortening of 55%.
Labs:
Parameter
Hemoglobin
Hematocrit
Platelets
Cyclosporine level
01/20/YYY ABC
Y
Children’s
Hospital
Roshni XXX,
M.D.
Value
13.6
24
406
248
Reference range
(Web search)
10-14 gm/dl
30-42%
150-400K/uL
300-350 ng/ml
Assessment and plan: Patient is now almost 3 months post-transplant and shows
no signs or symptoms suggestive of allograft rejection.
With a trough cyclosporine level of 248ng/mL and a goal level of 300-350,
we would like to increase her dose to 45 mg twice a day and recheck
another level during her next cardiac biopsy next week.
Return to clinic: in 3 weeks
Cardiac biopsy: 01/03/YYYY. CytoGam on 01/06/YYYY.
Follow-up with GI for further evaluation for a G-tube in order to fully
support her growth, especially given recent concerns of more frequent
emesis with the NG tube despite making adjustments to her feeds.
We would like to refer her to our Infectious Disease team to evaluate the
need for any changes in antimicrobial prophylaxis.
We would like to stop her Aspirin. We will continue to monitor her platelet
count.
Counseled on adequate fluid intake for infants. We will continue to monitor
her kidney function and assess for any signs of edema.
Correspondence to Dr. XX regarding Infectious Disease consultation:
Patient is almost completely nasogastric tube fed at this point, and there is a plan for
gastrostomy tube placement. After her discharge, she was briefly admitted at ABC
Children’s Hospital at Stanford at the beginning of YYYY, from January 2, YYYY,
until January 4, YYYY, for a viral illness complicated by dehydration, but
thereafter has been doing very well. (Hospitalization records from 01/02/YYYY01/04/YYYY are not available for review). Currently, Mother has no specific
concerns regarding Sophia’s health. She is on a lot of medications, including
immunosuppression, obviously, for her heart transplantation, but overall has been
recovering remarkably well.
Patient’s mother has several questions, which include whether patient can
71 of 87
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00195
-00199
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
participate in swimming in the river and also whether she can be around soil; about
having cats at home, as well as about exposure to the dust that is a constant problem
while living in the ranch.
BATES Ref
Review of systems: Patient is almost completely nasogastric tube fed. She is on a
24-calorie formula that is mixed with a little bit of Pedialyte that is given as a
continuous infusion at 35 mL per hour. She has significant oral aversion from her
prolonged intubation and, hence, the plan is for her to have a gastrostomy tube
placed in the near future.
Physical examination:
Vital signs: Temperature 36.8 degrees, blood pressure 108/65.
General appearance: There is mild hypertrichosis that is noted on the face.
Lungs: Bilateral good air entry. No crackles or wheezes.
Heart: S1, S2 heard. No murmurs.
Chest: There is a well-healed sternotomy wound that is noted, as well as other
healed scars from her chest tubes as well as PICC line.
02/01/YYY ABC
Y
Children’s
Hospital
Seth XXX,
M.D.
Assessment: Patient who is doing very well postoperatively, who now is going to
be returning to her home, which is a ranch with potential multiple exposures. Given
her immuno-compromise, the family is here specifically to get advice regarding
how best to prevent potential infections. We discussed to avoid any contact with
animal feces or areas where potentially there is contamination with feces. We
discussed very specifically that patient should not be swimming in the river.
Follow-up visit status post heart transplantation:
Patient has done well. She has returned home to her ranch in Northern California
and is adjusting well. Her feeding is improved and she is tolerating her continuous
NG feeds.
Vital signs:
HR – 144
Cuff BP – 108/81
Respiratory rate – 24
Physical examination:
Constitutional: Anterior fontanelle flat
Cardiovascular: Tachycardic rate, regular rhythm.
Skin: Hirsutism. Healing areas of erythema to legs bilaterally.
Echocardiogram report:
Normal ventricular function and no pericardial effusion
No significant tricuspid regurgitation
Labs:
Parameter
Hemoglobin
Hematocrit
Value
13.4
36.9
72 of 87
Reference range
(Web search)
10-14 gm/dl
30-42%
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00191
-00194
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
Platelets
Cyclosporine level
02/15/YYY ABC
Y
Children’s
Hospital
Rajesh Pppp,
M.D.
OCCURRENCE/TREATMENT
435
150-400K/uL
365
300-350 ng/ml
Assessment and plan:
Based on the physical examination and laboratory studies, there is no
evidence to suggest for allograft rejection.
The goal CSA level is 275-325 ng/mL and thus the dose remains
unchanged. Repeat drug levels will be performed in two weeks
Next cardiac biopsy: April, YYYY
Return to clinic in two weeks
Plan to discontinue Prednisone and Lasix if next biopsy is negative.
Hospitalization @ ABC Children’s Hospital for Fever and Frequent Emesis
*Reviewer's comment: Child Sophia was hospitalized from 02/12/YYYY-02/15/YYYY
Discharge summary:
Date of admission: 02/12/YYYY
Admitting diagnosis: 8 months status post heart transplant on 10/05/YYYY
admitted with fever and frequent emesis.
Detailed hospital course: Patient presented with fever and vomiting for ten to
twelve hours prior to admission and increased fussiness and poor sleep 2-3 days
prior to admission, which was initially attributed to teething. She had been drowsy
and less arousable since approximately 1 pm on the day of admission. She had been
vomiting approximately from 10 am to 12 pm every 30 min-1 hr, and the family had
been running Pedialyte through her NG tube at 35 ml/hr. Patient has a history of
feeding intolerance with emesis, for which she is maintained on continuous feeds.
Patient has had a mild cough, no runny nose, and some loose stools. The family
does have outside animals including dog, cat, chicken, and goats as well.
Patient was admitted, but access was unable to be obtained. She was empirically
placed on 1 L 100% NC, given Intramuscular (IM) Ceftriaxone after an anaerobic
blood culture was sent, and had a relatively reassuring chemical panel. Patient was
transferred to the Cardiovascular ICU for closer monitoring given altered level of
consciousness and to obtain IV access.
Hospital course:
Cardiovascular: Since admission patient has been well perfused on exam,
no clinical evidence of poor cardiac output. Echocardiogram showed no
pericardial effusion. RV and LV systolic function are normal. Trivial TR is
noted.
Transplant: Per Transplant Team she received CytoGam on 02/13/YYYY.
She continues on CellCept and Prednisolone at her home doses.
Respiratory: Patient was placed on 1 L of oxygen upon admission, which
was weaned for O2 saturations >92%.
A CXR done upon admission showed: No radiographic evidence to
suggest pneumonia. She received Pentamidine Isoniazid prior to discharge.
Neurology: Due to lethargy noted upon admission a CT and Lumbar
Puncture (LP) was done on 02/13/YYYY. The CT and LP showed no acute
73 of 87
BATES Ref
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00185
-00188
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
04/07/YYY XYZ
Y
Memorial
Hospital
District
OCCURRENCE/TREATMENT
abnormalities. Her lethargy has improved. A CSF culture from LP was sent
and is preliminarily negative as of 02/15/YYYY.
Gastrointestinal: Patient was started on Pedialyte via NG at 35ml/hr. On
02/14/YYYY she was advanced to 1/2 strength, then 3/4 strength feeds of
Similac 24 kcal/oz and Pedialyte which is her home feeding regimen. She
has not had any further emesis since advancing feeds. Her electrolytes have
remained stable although her magnesium was low at 1.4 on 02/14/YYYY.
Renal: Patient has had good urine output, BUN normal and Creatinine
mildly elevated at 0.4. No active nephrology concerns.
Infectious Disease: Patient had a fever on the day of admission, none since
admission. Ceftriaxone was discontinued on 02/15/YYYY which was when
cultures were negative.
Discharge vital Signs:
Temperature- 36.1
HR - 98
Cuff BP - 100/58
Respiratory Rate 31
X-ray of chest:
Clinical history: Previous heart transplant.
Impression: Postoperative changes. No active acute process identified.
D. T.
Matthews,
M.D.
04/12/YYY ABC
Y
Children’s
Hospital
David XXXX,
M.D.
Donna Xxxx,
C.P.N.P.
Follow-up visit status post heart transplantation:
Over the weekend, patient developed a fever to 101.4 rectally during the night, and
had some small emesis episodes. She did not have any other Upper Respiratory
Infection (URI) symptoms, and had no diarrhea. She was started on Keflex for
suspected Urinary Tract Infection (UTI). Since then she has done well, and is
slowly working back up to bolus feeds without any significant issues with emesis.
Review of systems:
Constitutional: Tmax 101.4 rectally approximately 5 days ago
Gastrointestinal: Slight cough before small amounts of emesis, but has been
tolerating medications fine. Stools have been slightly more loose due to her current
antibiotics.
Height: 70 cm; Weight: 7.2 kg; BMI: 14.69 kg/m2
Physical examination:
Cardiovascular: Tachycardic rate, regular rhythm.
Echocardiogram report:
Status post heart transplant operation
Normal LV systolic function
No coarctation of the aorta
74 of 87
BATES Ref
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00173
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00125
-00129
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
OCCURRENCE/TREATMENT
BATES Ref
Normal aorta
No pulmonary valve stenosis
Fractional shortening of 37%
Labs:
Parameter
Hemoglobin
Hematocrit
Platelets
Cyclosporine level
07/03/YYY ABC
Y
Children’s
Hospital
David XXXX,
M.D.
Value
12.3
34.5
480
429
Reference range
(Web search)
10-14 gm/dl
30-42%
150-400K/uL
300-350 ng/ml
Assessment and plan: Patient is now 6 months post-transplant and shows no signs
or symptoms suggestive of allograft rejection.
With a trough Cyclosporine level of 429 ng/mL and a goal level of 250300, we would for her to hold one dose of Cyclosporine tonight and
decrease back down to 40 mg twice a day.
Return to clinic in 5 weeks. She will receive pentamidine for PCP
prophylaxis tomorrow.
Cardiac biopsy on June YYYY
Given patient’s clinical improvement on Keflex after 5 days, it is okay for
patient to not complete a full 14-day course of antibiotics.
Follow-up visit status post heart transplantation:
Patient has not had any symptoms from a cardiovascular perspective. Her HR has
been between 120-140.
Review of systems:
Gastrointestinal: She is not as gaggy as she has been. Occasional gagging.
Intermittent constipation.
Vital signs:
Temperature – 36.3
HR – 150
Cuff BP – 121/74
Respiratory rate – 28
Physical examination:
ENT: Gingival hypertrophy.
Echocardiogram: The cardiac function is within normal limits. There is no
pericardial effusion. Fractional shortening of 40%.
Labs:
Parameter
Hemoglobin
Hematocrit
Cyclosporine level
Value
10.2
29.1
300
75 of 87
Reference range
(Web search)
10-14 gm/dl
30-42%
250-300 ng/ml
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00120
-00123
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
08/01/YYY ABC
Y
Children’s
Hospital
Daniel
Xxxxyyyy,
M.D.
OCCURRENCE/TREATMENT
Assessment and plan:
Her biopsy today showed a grade 1A for mild acute rejection.
*Reviewer's comment: It has been noted in this visit, that child Sophia
developed “grade 1A for mild acute rejection”.
The goal Cyclosporine 250-300 level is 300 ng/mL and is within the target
range. Repeat drug levels will be performed in 2 weeks
Next cardiac biopsy: 2 months
Return to clinic 1 month
Slowly decease the Pedialyte mixed with the formula, which will increase
her overall calories
Follow-up visit status post heart transplantation:
Review of systems:
Gastrointestinal: Occasional gagging. Intermittent constipation.
Diet: Patient is eating a wide variety of table foods from meats to cherries.
Height: 71 cm; Weight: 7.55 kg; BMI: 14.977 kg/m2
Nancy Xxxxx,
C.P.N.P.
BATES Ref
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00116
-00119
Vital signs:
Temperature – 36.6
HR – 140
Cuff BP – 118/90
Respiratory rate – 25
Labs:
Parameter
Hemoglobin
Hematocrit
Platelets
Cyclosporine level
08/20/YYY ABC
Y
Children’s
Hospital
David XXXX,
Value
11.9
35.3
406
350
Reference range
(Web search)
10-14 gm/dl
30-42%
150-400K/uL
250-300 ng/ml
Assessment and plan: Patient is 10 months post transplant and is clinically stable.
Her next biopsy will be scheduled for within the next 2-3 weeks because of
her previous 1A.
The goal Cyclosporine level is 250-300. Her level today is slightly above
the target range. Repeat drug levels will be performed at the time of her
biopsy.
Return to clinic 1 month
Schedule follow-up with GI clinic.
Increase her feeds to a minimum of 850 cc/day with a goal of 950 cc/day
for the next several weeks to see if she will start gaining weight again.
Follow-up visit for cardiac biopsy to evaluate allograft rejection:
Patient has not had any symptoms referable to the cardiovascular system.
Review of systems:
76 of 87
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
XXXX
XXXX
DATE
PROVIDER
M.D.
Donna Xxxx,
C.P.N.P.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Constitutional: Failure to thrive after making adjustments to her NG feeds to try
and increase oral intake. Since increasing her total daily volume/calories via NG
feeds, patient has demonstrated some weight gain, but still falls below the growth
curve for her size/age.
Gastrointestinal: Diarrhea and vomiting last week, now resolved. Of note, mother
was ill with same symptoms too
Skin: Bumpy rash to right forearm, left upper arm - non-irritating, stable.
Height: 69 cm; Weight: 7.78 kg; BMI: 16.34 kg/m2
Vital signs:
Temperature – 36.2
HR – 152
Cuff BP – 117/63
Respiratory rate – 20
Physical examination:
Constitutional: Still sleepy due to sedation.
ENT: No stridor, one lower tooth.
Heme: Catheterization site to right groin with bandaid.
Echocardiogram report: Post cardiac biopsy study. The cardiac function is within
normal limits. There is no pericardial effusion. Fractional shortening of 40%.
Biopsy results: No evidence of acute cellular rejection – Grade 0.
Labs:
Parameter
Hemoglobin
Hematocrit
Cyclosporine level
Value
9.2
26.5
197
Reference range
(Web search)
10-14 gm/dl
30-42%
250-300 ng/ml
Assessment and plan: Patient is now more than 10 months post-transplant, and
based on biopsy results, she shows no evidence of acute cellular rejection and is
stable from a cardiovascular perspective.
With a trough cyclosporine level of 197 and a goal range of 250-300
ng/mL, patient’s level is below target range. However, previous levels have
been within or above target range on the same dose, so no changes will be
made at this time and repeat level will be obtained in two weeks.
Return to clinic: 6 weeks
Repeat biopsy: beginning of November
Due to a low hemoglobin and hematocrit a repeat level will be obtained in
two weeks along with patient’s Cyclosporine level.
Consultation with Gastroenterology for concern re ongoing failure to thrive
in two weeks.
Inhaled Pentamidine in two weeks, to continue monthly until Prednisone is
completely discontinued.
Decrease Prednisone to 0.3 mg once daily.
77 of 87
BATES Ref
Health
CTR_00112
-00115
XXXX
XXXX
DATE
PROVIDER
09/10/YYY ABC
Y
Children’s
Hospital
David XXXX,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Infection control precautions were discussed.
Follow-up visit status post heart transplantation for inhalation treatment:
Patient is here for an inhalation treatment for inhaled Pentamidine for PCP
prophylaxis while taking Prednisone.
Patient has had a 4-5 day history of cough and nasal congestion without fever. Her
cough is intermittent and does not cause significant respiratory distress. She is not
vomiting with cough. The nasal discharge has mostly been clear. Her family has
been traveling over the last few days and patient has been a little bit more fussy
today, but she has not been sleeping well. She also appears to be teething because
she is chewing on her fingers a lot .There have been several wildfires in their area
which has made the air quality very poor.
Review of systems:
Respiratory: Intermittent cough.
Gastrointestinal: NG tube feeds. Was seen by Gastroenterology team this morning
with some adjustments to her feeds to try and stimulate her appetite.
BATES Ref
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00108
-00111,
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00104
-00107
Vital signs:
Temperature – 36.4
HR – 151
Cuff BP – 100/58
Respiratory rate – 39
10/09/YYY ABC
Y
Children’s
Hospital
Dr. Nguyen
Assessment and plan: Patient is now 11 months post transplant and is clinically
stable, with mild URI symptoms.
Okay to give inhaled Pentamidine. Will continue with monthly Pentamidine
until the Prednisone is completed.
The goal Cyclosporine level is 250-300 ng/mL and will be checked later
this week.
Next cardiac biopsy: November YYYY
Return to clinic: 10/10/YYYY
Infection control reviewed with family/patient the use of the N95 mask or
respirator during hospital construction.
Correspondence to Dr. XX regarding feeding difficulties:
Patient was referred to Gastroenterology (GI) Clinic for management of feeding
difficulties and failure to thrive. She displayed no signs of oral aversion and she was
eating without difficulty, though she was still dependent on NG tube feeds for all of
her nutrition. She had some anemia that was thought to be multifactorial in the past,
but her last Hemoglobin and Hematocrit (H&H) on 10/09/YYYY was 11.7 and
34.9.
Physical examination:
HEENT: Patient has an 8-French NG tube in the left naris without skin breakdown.
Assessment: Patient continues to do very well from a GI perspective. Again,
evidence of oral aversion or oromotor difficulties. Despite reduction in her total
78 of 87
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00143
-00144
XXXX
XXXX
DATE
PROVIDER
11/21/YYY ABC
Y
Children’s
Hospital
Daniel
Xxxxyyyy,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
caloric intake via the PediaSure from 1000 calories per day to 750 calories per day
in the interim, she has managed to gain weight, albeit on the lower side of normal
for age. She also seems to be taking larger quantities by mouth.
Recommendations: We will reduce the PediaSure from 750 mL total volume to
600 mL total volume to encourage more oral intake of regular food.
Follow-up visit status post heart transplantation:
Patient’s annual study was cancelled because of persistent URI illness. She had
fever 2 weeks ago that lasted for 2 days accompanied by vomiting. Her blood
pressure was low and the Norvasc was discontinued. She improved for several days
and now has had a 4 days history of nasal congestion and eye discharge without
fever. She is coughing, had decreased oral intake and had trouble sleeping when
laying down.
Height: 74 cm; Weight: 7.95 kg; BMI: 14.51 kg/m2
Vital signs:
Temperature – 36.5
HR – 142
Cuff BP – 108/62
Respiratory rate – 28
Physical examination:
Eyes: Slightly red eyes with minimally injected discharge at this time.
Echocardiogram report (Dated 11/20/YYYY):
The systolic function of both ventricles is normal. There is no pericardial effusion
or significant valve dysfunction. Fractional shortening of 32%.
Labs:
Parameter
Hemoglobin
Hematocrit
Platelets
BUN
Value
10.4
31.0
429
26
Reference range
(Web search)
10-14 gm/dl
30-42%
150-400K/uL
5-18
Assessment and plan: Patient is now 13 months post transplant and is stable from a
cardiac perspective, but with URI and Recurrent Otitis Media (ROM).
Based on the physical examination and laboratory studies, there is no
evidence to suggest for allograft rejection.
The goal cyclosporine level is 200-250 ng/mL and slightly above target.
Repeat drug levels will be performed with her annual study.
Next cardiac biopsy: 2-3 weeks allowing time for URI to resolve.
Return to clinic: 3 months.
Infection control - reviewed.
Start Amoxicillin 300mg twice daily for 10 days for Otitis Media (OM).
Reviewed medication dose and side effects with parents.
79 of 87
BATES Ref
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00099
-00103
XXXX
XXXX
DATE
PROVIDER
01/07/YYY ABC
Y
Children’s
Hospital
David XXXX,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Patient may not receive any live virus vaccines.
Follow-up visit status post heart transplantation for annual studies:
Patient presented for annual studies with cardiac biopsy to evaluate for allograft
rejection, hemodynamics and evaluation of her SVC gradient and coronary
angiogram to assess for graft coronary artery disease.
She still has a residual cough, but overall has been doing well otherwise.
Height: 64 cm; Weight: 8.5 kg; BMI: 20.75 kg/m2
Vital signs:
Temperature – 37.4
HR – 118
Cuff BP – 90/57
Respiratory rate – 29
Physical examination:
ENT: No stridor. Multiple teeth erupting.
Heme: Catheterization site with bandaid intact.
Echocardiogram report:
No tricuspid valve regurgitation
Trace-to-mild pulmonary valve insufficiency
Qualitatively normal right ventricular systolic function
Normal left ventricular systolic function
No pericardial effusion
Fractional shortening of 48%
Cardiac biopsy results: No evidence of acute rejection – Grade 0.
Angiogram: The SVC pressure is 6 mmHg to the right atrium and mild
angiographic narrowing. The coronary arteries are normal.
Labs:
Parameter
Hemoglobin
Hematocrit
Value
9.6
28.1
Reference range
(Web search)
10-14 gm/dl
30-42%
Assessment and plan: Patient is 19 months of age status post heart transplantation.
Based on biopsy results, patient shows no evidence of acute cellular rejection or
graft coronary artery disease and is stable from a cardiovascular perspective.
With a late trough cyclosporine level of 177 and a goal range of 200-250,
patient’s level is not an accurate 12-hour trough, but is close to target range.
No changes will be made to her dose and a repeat level will be obtained
next week locally.
Return to clinic: 2 months
80 of 87
BATES Ref
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00095
-00098
XXXX
XXXX
DATE
PROVIDER
03/27/YYY ABC
Y
Children’s
Hospital
David XXXX,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Repeat biopsy: May YYYY
Okay to wean Nystatin and discontinue Lasix.
Follow-up with GI to follow weight gain.
Infection control precautions were discussed.
Follow-up visit status post heart transplantation:
Patient has had multiple illnesses since January, but has not required any
hospitalizations. Blood pressures at home have been between high 80s to high 90s
systolic. Heart rate has been averaging in the 130s, which is slightly more elevated
than previously noted. However, patient is active and playful, with good energy.
Review of systems:
HEENT: URI symptoms a few weeks ago.
Respiratory: No noted stridor with any at her intercurrent illnesses. History of
subglottic stenosis. Per mother, ENT suggested that if patient continues to do well,
she may be able to stop Budesonide after the spring.
Gastrointestinal: NG tube fed for supplemental nutrition. Followed in GI clinic.
BATES Ref
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00091
-00094
Height: 78 cm; Weight: 8.7 kg; BMI: 14.3 kg/m2
Vital signs:
Temperature – 36.3
HR – 131
Cuff BP – 119/62
Respiratory rate – 26
Echocardiogram report: Post cardiac transplantation evaluation. The cardiac
function is normal. There are no effusions noted. There is no significant valvar
regurgitation. Fractional shortening of 34%.
05/21/YYY ABC
Y
Children’s
Hospital
David XXXX,
M.D.
Assessment and plan: Patient is status post heart transplantation. From a clinical
standpoint, patient is doing well 17 months post-transplant, and shows no signs or
symptoms suggestive of allograft rejection.
Return to clinic for her next cardiac biopsy.
Cardiac biopsy: May YYYY
Okay to stop Nystatin. Monitor for signs of thrush.
Infection control precautions were again reviewed with the family.
Follow-up visit status post heart transplantation for repeat cardiac biopsy:
Since the last clinical encounter, patient has not had any symptoms referable to the
cardiovascular system. Approximately two weeks ago, she experienced an episode
of tachycardia and vomiting, for which she was assessed in her local ER. (ER
records not available for review). The symptoms self-resolved, and were thought to
be related to a food poisoning episode per mother. Patient has not had any further
episodes since. Blood pressures at home have been between 98-105 systolic. Heart
rate has been between the 120s to 130s.
Review of systems:
Respiratory: No signs of dyspnea or stridor. History of subglottic stenosis
81 of 87
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00087
-00090
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Gastrointestinal: Has not required the NG tube for over one week. Stools formed,
not watery.
BATES Ref
Height: 78 cm; Weight: 9 kg; BMI: 14.79 kg/m2
Vital signs:
Temperature – 36.9
HR – 129
Cuff BP – 89/42
Respiratory rate – 30
Echocardiogram report:
Trivial tricuspid valve regurgitation inadequate to estimate RV systolic
pressure
Trace pulmonary valve insufficiency
No mitral or aortic valve regurgitation
Mild flow acceleration across the superior vena cava with a mean gradient
of 4 mmHg
Qualitatively normal right ventricular systolic function.
Normal left ventricular size and global systolic function.
No pericardial effusion
Biopsy results: No evidence of rejection – Grade 0.
Labs:
Parameter
Hemoglobin
Hematocrit
BUN
Cyclosporine level
11/11/YYY ABC
Y
Children’s
Hospital
David XXXX,
M.D.
Value
8.9
27.6
26
172
Reference range
(Web search)
10-14 gm/dl
30-42%
5-18
200-250 ng/ml
Assessment and plan: Based on biopsy results, patient shows no evidence of
rejection and is stable from a cardiovascular perspective.
With a trough cyclosporine level of 172 and a goal range of 200-250,
patient’s level is slightly below target range. Thus, we will increase her
dose of CSA to 40 mg in the morning 45 mg in the evening and repeat
another level in 1-2 weeks
Return to clinic: 2 months. Repeat biopsy: 4 months
Hypomagnesemia: Increase magnesium slightly to 1.5 mL thrice daily and
monitor for any signs of muscle cramping.
Counseled regarding trying to administer iron with orange juice for
improved absorption and better palatability.
Follow-up visit status post heart transplantation for cardiac biopsy:
Since the last clinical encounter, patient developed a high fever with diarrhea and
emesis, for which her previous biopsy was canceled. She has improved over the
past week, and has been at afebrile. Apart from these symptoms, she has not had
any symptoms referable to the cardiovascular system.
82 of 87
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
XXXX
XXXX
DATE
DOB: 03/22/YYYY
DOB: 06/07/YYYY
PROVIDER
OCCURRENCE/TREATMENT
Blood pressures at home have been between high 80s to low 100s systolic. Heart
rate has been between 110s to 120s.
Review of systems:
Constitutional: High fever to 104.5 over one week ago
HEENT: Ongoing runny nose
Respiratory: Some snoring noted with recent illness
Gastrointestinal: Diarrhea with fever, but no further issues. No emesis over the
past two days. Before patient’s recent illnesses, she had tolerated all oral intake
without the NG tube and was demonstrating stable weight gain. Since her recent
illnesses, however, she has had the NG tube in place
Skin: Stable, flesh colored bumps to arms and legs, sometimes itchy.
Height: 74.5 cm; Weight: 10.3 kg; BMI: 18.56 kg/m2
Vital signs:
Temperature – 36.7
HR – 130
Cuff BP – 103/87
Respiratory rate – 20
Physical examination:
Constitutional: Irritable and upset, but somewhat consolable with parents.
Echocardiogram report: The cardiac function is within normal limits. There is no
pericardial effusion. Due to patient movement, this study is limited. Fractional
shortening of 41%.
Biopsy results: No evidence of rejection – Grade 0.
Labs:
Parameter
Hemoglobin
Hematocrit
WBC
BUN
Value
9.4
28.7
2.6
26
Reference range
(Web search)
10-14 gm/dl
30-42%
5-19.5 K/uL
5-18
Assessment and plan: Based on biopsy results patient shows no evidence of
rejection and is stable from a cardiovascular perspective.
With a trough Cyclosporine level of 214 and a goal range of 175-225,
patient’s level is within target range. Thus, no changes will be made to her
dose and a repeat level can be obtained in one month.
Return to clinic: two months
Repeat biopsy: four months (February YYYY) for annual study
Patient’s WBC is low today. We would like to repeat her CBC in two
weeks. If patient’s CBC is within normal limits at that time we would like
to increase her CellCept dosing.
83 of 87
BATES Ref
CTR_00078
-00082
XXXX
XXXX
DATE
PROVIDER
01/09/YYY ABC
Y
Children’s
Hospital
David XXXX,
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Infection control precautions were reviewed.
Follow-up visit status post heart transplantation:
Since the last clinical encounter patient has not had any symptoms referable to the
cardiovascular system. Blood pressures at home have been between 80s to 100
systolic. Heart rate has been averaging in the 110s to 120s.
Review of systems:
HEENT: URI symptoms including runny nose which began approximately 2 weeks
ago.
Respiratory: Cough developed about one week ago. No signs of respiratory
distress.
Gastrointestinal: Has not required the NG tube recently. Followed by GI for
history of poor weight gain.
Height: 87.5 cm; Weight: 10.15 kg; BMI: 13.26 kg/m2
Vital signs:
Temperature – 36.8
HR – 124
Cuff BP – 943/53
Respiratory rate – 26
Echocardiogram report:
Post cardiac transplantation evaluation
There is no mitral regurgitation
There is trace tricuspid regurgitation which estimates a RV-RA pressure
gradient of 17 mmHg
There is mild flow acceleration across the superior vena cava
The cardiac function is normal - No allusions noted
Fractional shortening of 38%
Labs:
Parameter
Hemoglobin
BUN
Value
11.2
28
Reference range
(Web search)
10-14 gm/dl
5-18
Assessment and plan: From a clinical standpoint, patient currently is recovering
from an upper respiratory infection but appears stable; she is more than two years
post-transplant and shows no signs or symptoms suggestive of allograft rejection.
With a trough cyclosporine level of 207 and a target range of 175-225,
patient’s level is within target range. Thus, we will make no changes to her
dose and repeat another level at the next clinical encounter.
Return to clinic: two to three months following after her cardiac
biopsy/May or June YYYY.
After discussing patient’s weight and progress nutritionally, we agree with
the plan to start Periactin to stimulate her appetite.
With regard to patient’s current URI symptoms, we have recommended that
84 of 87
BATES Ref
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00073
-00077,
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00070
-00072
XXXX
XXXX
DATE
PROVIDER
05/15/YYY Stanford
Y
Children’s
Health
Kaylie Xxxx,
M.D.
06/30/YYY Carrie Xxxx,
Y
M.D.
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
patient may use her nebulizer Budesonide during her current illness to see if
it will help with her coarse breath sounds,
Infection control precautions were again reviewed.
Correspondence to Dr. XX regarding GI consultation for failure to thrive and
feeding refusal:
Summary: Patient is doing very well from a GI perspective despite lack of weight
gain over the past several months, probably due to decreased total caloric intake
after supplemental PediaSure was reduced by mother from 3 to 4 cans a day to now
less than 1 can a day. She is drinking regular whole milk and eating a large variety
of regular and high calorie foods. She has absolutely no problems with oral motor
deficits and her appetite is excellent. I do not think she would have additional
benefit with any GI-related medications at this time.
My only suggestion for now is that she should have regular weight checks with her
Primary Team (Cardiology) and should there be concerns about drop in weight,
then certainly I can see her back in GI clinic. I will leave the orders for PediaSure at
about 3 cans a day and encouraged the mother to try to get her to drink as much of
this as possible without causing a struggle and without a decrease in her appetite for
or intake of other foods so that she maintains adequate weight gain.
X-ray of chest:
History: Cough. History of heart surgery as an infant.
Impression: Probable bronchitis versus reactive airway disease.
10/06/YYY ABC
Y
Children’s
Hospital
David XXXX,
M.D.
Follow-up visit status post heart transplantation:
Since the last visit to the Heart Transplant Clinic, from a cardiovascular perspective,
patient has been doing well overall. She has, however, had almost 4 months of
intermittent loose stool. Mother recalls that it began after she swam in the river near
their home (Rural, on their ranch). This was the first time she swam there, and the
diarrhea seemed to correlate with the exposure.
*Reviewer's comment: It has been noted that child Sophia was involved in
swimming activities in the river nearby her family’s ranch.
It waxes and wanes and she will have near-normal stool for a few days, then it
becomes pasty, then she has several days of very loose stool 5-6 times per day. She
stays hydrated and has no fever. There is no blood in the stool and she does not
vomit. She sometimes has crampy abdominal pain with this. No respiratory
symptoms.
Vital signs:
HR – 90-100
Systolic BP – low 100’s
Respiratory rate – 25
Physical examination:
85 of 87
BATES Ref
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00130
-00131
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00022
XXXXS_29
6150_29615
4_rec fm
XXYY
Valley
Health
CTR_00150
-00155
XXXX
XXXX
DATE
PROVIDER
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
Cardiovascular: Quiet precordium, normal S1 and S2, no murmurs, no S3 and S4.
Pulmonary/chest: Effort normal and breath sounds normal. No respiratory distress.
Echocardiogram report:
No significant atrioventricular valve regurgitation
No left ventricular outflow tract obstruction
No aortic valve regurgitation
No pulmonary valve stenosis
Trace pulmonary valve regurgitation
Normal left ventricular size and systolic function
Qualitatively normal right ventricular systolic function
No pericardial effusion
Fractional shortening: 34.6%
Labs:
Parameter
Hemoglobin
Hematocrit
Cyclosporine level
11/10/YYY Multiple
YProviders
12/31/YYY
Y
Value
9.1
28.1
134
Reference range
(Web search)
10-14 gm/dl
30-42%
200-250 ng/ml
Assessment and plan: Patient is now 3 years post transplant and is doing well.
From a clinical standpoint, she shows no signs or symptoms suggestive of allograft
rejection. She has unfortunately had almost 4 months of diarrhea with no other
symptoms which seem to correlate with swimming in the river near her family’s
ranch.
The goal CSA level is 175-226 and a level of 134 is below the target range.
Next cardiac biopsy will be in 3 months
Return to clinic in 3 months
Infection control: Family is aware of our current infection central
recommendations In light of the hospital construction.
Medication changes: Increase CSA to 55 mg twice daily
Multiple visits for cold symptoms, flu symptoms, nutrition and feeding
difficulties, swollen gums, swollen tonsils, prophylactic immunotherapy, bumps
on face, NG tube feeds, right wrist pain, right ear pain, cough, chronic
diarrhea and ear infection:
BATES Ref: XXXXS_296150_296154_rec fm XXYY Valley Health CTR_00048,
00046-00047, 00140-00142, 00045, 00172, 00148-00149, 00043-00044, 00042,
00137-00139, 00041, 00062, 00038-00040, 00037, 00083-00086, 00134-00136,
00036, 00035, 00132-00133, 00034, 00025-00026, 00023-00024, 00019-00021,
00017-00018, 00165-00167, 00010-00016, 00007-00008, 00005-00006
06/07/YYY Multiple
*Reviewer's comment: Patient visited hospital multiple times for infections
secondary to immunosuppressive therapy and for NG tube feeds which are not
cardiac related and hence combined and not elaborated; They will be elaborated
later upon request.
Miscellaneous records: Authorization, admission record, consent forms, blank
86 of 87
BATES Ref
XXXX
XXXX
DATE
Y05/13/2015
PROVIDER
Providers
10/16/1998
05/21/2015
Multiple
Providers
DOB: 03/22/YYYY
DOB: 06/07/YYYY
OCCURRENCE/TREATMENT
pages, labs, flow sheets, assessment, immunization history, orders, checklist, coding
summary form,
BATES Ref: XXXXS_295867_rec fm UCD_00001-00002, 00103, 00106-00107,
00110, 00263-00270, 00343-00345, 00351, 00360-00362, 00370XXXXS_296150_rec fm Stanford Hospitals & Clinics_00003, XXXXS_296150_rec
fm Stanford Hospitals & Clinics_00008, 00013-00032, 00035-00039,
XXXXS_296150_296154_rec fm XXYY Valley Health CTR_00001-00004, 00009,
00049-00061, 00063, 00065-00069, 00124, 00145-00147, 00168-00171, 0017400182, 00189-00190, 00208-00210, 00245-XXXXS_297160_rec fm ABC Children's
Hospital_00002, XXXXS_297160_rec fm ABC Children's Hospital_01398-01401,
03209, 03601-03603
*Reviewer's comment: No significant details are noted from above records, hence
combined and not elaborated.
Miscellaneous records: Blank pages, card details, consent and authorization forms,
checklist, problem list, orders, acknowledgement, advance beneficiary notice,
patient education, laboratory reports, medical bills, insurance details, patient’s
information, face sheet, assessment forms, radiology reports, medical questionnaire,
visits for fever and chills, infected belly button, skin abscesses of groin, flu shot,
anxiety, Intrauterine Device (IUD) falling out, right breast lump, well woman exam,
IUD removal, mammogram, pathology report, affidavit and legal documents:
BATES Ref: 297065_rec fm ABCHealth Center - 000001-00019, 000020-00027,
000030-00035, 000037, 297065_rec fm ABCHealth Center - 000039-297066_rec
fm XYZ Memorial-Dr. XX, MD - 00002, 000008-00011, 000025-00027, 000033,
000035, 000064-00065, 000069, 000071, 000073-00074, 000081-00082, 00008600087, 000103, 000109-00110, 000135-00149, 000154-00160, 000162-00185,
000187, 000192-00196, 000197-00287, 000289
*Reviewer's comment: No significant details are noted from above records, hence
combined and not elaborated.
87 of 87
BATES Ref