Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
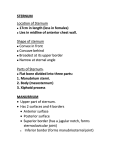
Lip Teh January 2006 Congenital Chest wall deformities Classification 1. Poland syndrome 2. pectus excavatum 3. pectus carinatum 4. sternal clefts 5. generic skeletal and cartilage dysplasias (e.g., absent ribs, vertebral anomalies). Embryology o Ossification proceeds craniocaudally during 6th-9th intrauterine month or later o Fusion of the 2 sides of the sternum proceeds cephalocaudal - cells migrate from two lateral plates of mesoderm on either side of the anterior chest Lip Teh January 2006 wall as bands to fuse in the midline to form the sternum by the tenth week of gestation. Anatomy of sternum First 7 pair of ribs articulates with sternum (true ribs) 1st sternochondral joint articulates with manubrium and is a primary cartilaginous joint Next six are synovial joints Manubriosternal and xiphisternal joints have hyaline covered surfaces with intervening fibrocartilage disc (the sternoclavicular joint has fibrocartilage surfaces with a intervening fibrocartilage disc) Vascular territories of the chest wall all feeding vessels Lip Teh January 2006 Pectus Excavatum Funnel chest Epidemiology most common congenital deformity of the chest wall, 90% of all chest wall anomalies. 1 in 300-400 live births M>F 3:1 No known cause but likely to be an intrinsic disturbance of osteogenesis and chondrogenesis, hereditary in 35% associated with Marfan(25%) and Poland syndromes Pathophysiology abnormal overgrowth of bone and cartilage of the anterior chest wall holding sternum posteriorly, typically affecting 4-5 ribs on each side of the sternum. begins at the manubriosternal junction, reaching its deepest point at the xiphisternal junction. Clinical Deformity usually noted at birth Progressive worsening during periods of growth spurts May be asymmetric, right side usually worse Features: o Depressed sternum Lip Teh January 2006 o rounded sloping shoulders hunched forwards o dorsal thoracic kyphosis o a “potbelly” o abnormal breathing characterized by retraction of the sternum on deep inspiration. Functional impairment is rare. Severe pectus excavatum is associated with exercise intolerance and evidence of respiratory(restrictive) and cardiac dysfunction (mitral valve prolapse – 20-60%). Investigations CXR – PA/lateral Chest CT o CT index = transverse chest diameter / anteroposterior diameter o CT index >3.2 correlated with a severe deformity requiring surgery at age 4-6 years to 1. relieve structural compression of the chest and allow normal growth of the thorax 2. avert cardiopulmonary dysfunction later in life 3. improve cosmesis.(Haller 1987) o Assess for displacement of cardiac structures Ancillary tests – PFT, ECG Lip Teh January 2006 Classification On lateral xray - anterior surface of the vertebral column to the posterior surface of the sternum (Fabricus 1957) 1. 2. 3. 4. Normal Mild Moderate Severe male 10.5cm, female 9cm >7cm 5-7cm <5cm Indications for Surgery 1. Cosmesis: most common reason - self-esteem and body image perception 2. Rarely to improve cardio-respiratory function in severe cases - controversial whether surgery improves pulmonary and cardiac function with some studies demonstrating increase and others decrease in function 3. Often there is a good psychological reason for surgery. 4. To allow improvement of the secondary, compensatory deformities Management Non-Surgical External brace/orthosis – Haje method (Direct Chest Compressor brace + exercises) Surgical Types: 1. Camouflage techniques 2. Sternal/cartilage resections 3. Minimally invasive - Placement of retrosternal bar Camouflage techniques Indicated for growth complete and asymptomatic cases Autograft deepithelialized pedicled latissimus dorsi flap (PRS 1997) buried, de-epithelialized transverse rectus abdominis myocutaneous flap (PRS 1986) Allograft Customised silicone implants (Murray 1965) i. Subxiphoid incision ii. Initially placed subcutaneous but now submuscular placement preferred iii. Inferior border of the pectoralis major muscle is identified and its insertion elevated from rib, costal cartilage, and sternum bilaterally. Lip Teh January 2006 iv. Fixation is facilitated by a Dacron patch on the posterior aspect of the implant. Southwick (PRS 2004) uses a calf implant placed above periosteum Complications i. Implant related 1. Palpability 2. Visibility 3. Migration 4. extrusion Resection and Reconstruction Timing of surgery – age 4 to teenagers near growth completion or dictated by symptoms Open technique (sternochondroplasty) pioneered by Ravitch (1949) anterior thoracic incision muscle and skin flaps raised each abnormal cartilage is excised with preservation of the perichondrium xiphoid is divided from the rest of the sternum and allowed to retract opening wedge osteotomy posteriorly on the sternum (with a wedge of rib) fixation of the sternum in the corrected position Modified Ravitich techniques Wolf (1987) used transcutaneous wires and an external brace Haller (1989) places a temporary retrosternal bar to prevent postop depression Hayashi (1992) uses a vascularised rib strut (left 7th rib) based on the anterior intercostal branch of the internal mammary artery following resection Matsui (1994) used a bioabsorbable strut >2.5mm thick (poly L-lactide) Genc (PRS 2002) used 2 PTFE bars i. Advantage over metal said to be easier removal and cheaper Lip Teh January 2006 Kobayashi (PRS 1997) used the endoscope to minimize the chest scar o 2.5-4 cm incision just above the xiphoid process o subperichondrial partial costal cartilage resection under direct visualization.. Cut is oblique to allow overlapping o pleura was freed from the sternum under visualization o wedge osteotomy of the sternum at the point of maximum curve deformation o retrosternal titanium or poly l-lactide struts were used o disadvantage is long operative times and difficult cartilage resection in adults Sternal Turnover Wada (1970) – devascularised turnover sternal graft i. Complications of avascular necrosis and infection, absorption and recurrence Lip Teh January 2006 Doty (1983) and Ishikawa (1988) used pedicled turnover sternal flaps based on the IMA Ninkoviv (PRS 2003) described revascularised sternal turnover. In a later followup letter, the authors experienced major complications. They recommend that the procedure not be used as a routine for treating pectus excavatum deformity Complications i. Major 1. bleeding 2. cardiac perforation 3. parodoxical respiration – floating sternum 4. pneumothorax 5. chest wall constriction due to lack of chest wall growth following the procedure in children 6. sternal necrosis /dehiscence 7. sternal osteomyelitis ii. Minor 1. keloid scarring 2. recurrence 3. sinus tracts from fixation 4. over/under correction iii. Related to sternal bar 1. displacement 2. migration into peritoneal cavity 3. embedded into myocardium Minimally Invasive Nuss technique (Donald Nuss J Pediatr Surg 1998) Observed that the anterior chest wall was malleable particularly in children (ie in emphysema, asthmatics) Lip Teh January 2006 Timing: best for pediatric patients Technique involves placement of a convex steel bar under the sternum through a small lateral thoracic incision i. transverse incision 2.5 cm long made on the lateral chest wall between the anterior and posterior axillary lines. ii. Skin tunnels are raised anteriorly and the intercostal space is entered using a Kelly clamp which is slowly advanced across the mediastinum immediately under the sternum under thorascopic control. iii. dissection is carried over to the contralateral chest iv. umbilical tape is passed through this tunnel, and a custom premolded metal bar is passed between the two sides v. occasionally 2 bars are needed vi. fixation to lateral chest wall vii. stabilization bar may be required if there is still a tendency for rotation (vertical metal bar attached to the extrathoracic ends of the transverse bar) Post op i. Average length of stay is 4-7 days ii. bending at the hip, heavy lifting and slouching are not allowed for the first month iii. contact sports are to be avoided for at least 3 months bar generally remains implanted for 2 years excellent and good results reported at 93% and 96% best results in children aged 8-12 Complications (up to 20%) i. displacement of the retrosternal stainless steel support bar (10%) 1. up to 10% in early series 2. more prone with teenagers 3. reduced incidence with stabilizer bar (2.5%) ii. cardiac perforation 1. 1 reported case prior to use of thoracoscope Lip Teh January 2006 Pectus Carinatum Pigeon chest Epidemiology 1 in 1700 M>F 4:1 Pathogenesis abnormal costochondral overgrowth of unknown cause. pectus excavatum and carinatum may be two different morphologic manifestations of the same disease. o If the overgrowth of the costal cartilages generates a downward, inward force, it produces pectus excavatum; o if the force is outward, pectus carinatum is the result. Associated with Noonans syndrome 25% have a positive family history of chest wall deformities Clinical Most children present during puberty and worsen with periods of growth Most are asymptomatic, although some develop a restrictive chest pattern or emphysema Mitral valve prolapse seen in 97%, less commonly rhythm and contractility problems (more likely in chondromanubrial subtypes) Usually symmetrical (65%) Investigations CXR PFT if concerned about clinical symptoms and the appearance of the chest wall on examination ECG, ECHO Classification Morphological types 1. Type 1: chondrogladiolar (chicken breast or keel chest) a. more common type b. middle and lower portions of the sternum are particularly prominent and arch forward. c. The costal cartilages are concave and usually symmetrically depressed, accentuating the sternal prominence. 2. Type 2: chondromanubrial (Pouter pigeon breast) a. less common and more complex b. upper portion of the sternum is anteriorly prominent and the body of the sternum has a steep depression posteriorly. c. A final anterior deflection of the distal sternum gives the characteristic Z shape to the sternum on a lateral view. Lip Teh January 2006 3. Type 3:lateral pectus carinatum Chondrogladiolar Management Nonsurgical dynamic chest compressors and body casting o more successful for this than for excavatum o ideal candidate is a motivated skeletally immature child with a mild deformity. Surgical Modified Ravitch open sternochondroplasty o Exposure of the sternal deformity by subperiosteal dissection and elevation of pectoralis major muscles bilaterally. o V-shaped transverse osteotomy performed high on the sternum above the level where the abnormal forward curvature begins. o The osteotomy is through the anterior table of the sternum leaving the posterior lamina intact. o The resection is done in the intercostal space rather than at the sternocostal junction. o Below the transverse osteotomy, the involved cartilages are resected subperiosteally. o Pectoralis muscles are brought together across the midline and sutured to one another o A second transverse osteotomy is required for chondromanubrial types. Chiselling off the protuberant portion of the strernomanuberial junction is required. o Type 3 may need simple resection of involved cartilages only. Kobayashi endoscopic approach (PRS 1997) Lip Teh January 2006 Cleft Sternum Rare – 0.15% of chest wall deformities Range from complete clefting to minor V shaped defects, to sternal foramina Associated with facial hemangiomas (33%) Classification (Ravitch) 1. cleft sternum alone without associated anomalies. This defect can be: o superior cleft (the most common) o inferior cleft o complete bifid sternum. 2. cleft sternum associated with vascular dysplasia. 3. true ectopia cordis (partial or complete extramediastinal displacement of the heart) associated with cleft sternum, cardiac lesions, and other midline malformations. 4. Cantrell's pentalogy with a combination of cleft or absent sternum, ventral diaphragmatic defect, midline ventral abdominal defect, communication between the pericardial and peritoneal cavities, and cardiac lesions timing of the operation is controversial. o most authors suggest an early operation (within the first month of life) for 1. in symptomatic infants with recurrent chest infections and heart failure 2. to restore the bony protection of the sternum to vital mediastinal structures 3. to eliminate paradoxical motion of the chest and hence provide normal intrathoracic pressures 4. to remove the stigma of large, visible contour deformity 5. early repair is technically simple, with easy approximation of the sternal edges due to compliance of the chest wall. Repair is best achieved in the neonatal period, when the chest wall is most compliant, and compression of underlying structures is minimal. Methods: o Primary closure Only possible in neonates but pectus excavatum may develop later in life Lip Teh January 2006 can be reinforced with pectoralis major flaps, which are elevated and apposed anteriorly to protect the primary repair and reduce the lateral distraction forces exerted by anomalous pectoralis insertion o Sliding chondrotomies with partial clefting partial resection of the first, second, and third costal cartilages, disruption of the sternoclavicular junction, and closure of the sternal bars with stainless steel wire o pectoralis major myoplasty o free split corticocancellous iliac bone graft from inner table covered with an islanded pectoralis major muscle flap (Biswas BJPS 2001) o Autograft options: costal cartilage, rib, iliac crest, parietal skull, and tibial periosteum. o Alloplasts: stainless steel mesh, Marlex, acrylic, silicone elastomer, and Teflon - associated with tissue reactions resulting in bradycardia and/or hypotension and an increased risk of infection. An important note with local muscle flaps is that IMA may be absent thus turnover pec major and superiorly based rectus flaps may be unreliable.