Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
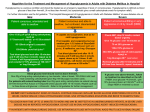
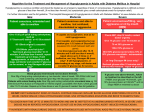
Paediatric Clinical Guideline 9.1 Endocrine: Hypoglycaemia Short Title: Full Title: Date of production/Last revision: Hypoglycaemia in infants and children: Aetiology, investigation and treatment Guideline for the management of hypoglycaemia in infants, children and young people: Aetiology, investigation and treatment Nov 2007 Explicit definition of patient group to which it applies: This guideline is intended for infants outside of the neonatal period (i.e. >28 days) children and young people up to the age of 19 years who do not have a diagnosis of diabetes or other established metabolic disorder. Name of contact author Dr Becky Smith, Paediatric SpR Dr Tabitha Randell, Consultant Paediatrician Ext: Revision Date Nov 2010 This guideline has been registered with the Trust. However, clinical guidelines are 'guidelines' only. The interpretation and application of clinical guidelines will remain the responsibility of the individual clinician. If in doubt contact a senior colleague or expert. Caution is advised when using guidelines after the review date. Hypoglycaemia in infants and children: Aetiology, investigation and treatment Scope of Guideline This guideline is intended for infants and children outside of the neonatal period (i.e. >28 days) who do not have a diagnosis of diabetes or other established metabolic disorder. There is a separate neonatal guideline available from the Neonatal Unit. Definition Hypoglycaemia refers to the inadequacy of circulating levels of blood glucose and is defined as a laboratory blood glucose measurement of < 2.6mmol/l. Hypoglycaemia may be associated with clinical symptoms and signs or be asymptomatic. Background Hypoglycaemia in children beyond the neonatal period is relatively common accounting for 1 in 500 hospital admissions. The majority of these will be in patients with known diabetes. In children with no previously identified cause for hypoglycaemia up to 30% of cases are due to defects in fatty acid oxidation. Prolonged or recurrent hypoglycaemia, especially when associated with symptoms and clinical signs can cause long term neurological damage or death. Thus, prompt recognition and treatment are essential. Becky Smith Page 1 Nov 2007 Paediatric Clinical Guideline 9.1 Endocrine: Hypoglycaemia Symptoms The following are typical symptoms and signs of hypoglycaemia but please be aware that this list is not exhaustive and a blood sugar should be checked in any unwell child. Neonate Pallor Sweating Tachypnoea Jitteriness Apnoea Hypotonia Feeding difficulties Irritability Abnormal Cry Convulsions Infant and older child Anxiety Tremor Palpitations Weakness Nausea and vomiting Hunger Abdominal Pain Headache Confusion Coma Visual disturbance Convulsions Emergency management and Investigation of Hypoglycaemia History Age Feeding History Birth history and weight Neonatal jaundice Tolerance to fasting/ illness Drug ingestion Family history and parental consanguinity Becky Smith Page 2 Signs Features of sepsis Hepatomegaly Encephalopathy Optic atrophy / cataracts Genitalia appearance Skin pigmentation Nov 2007 Paediatric Clinical Guideline 9.1 Endocrine: Hypoglycaemia Management of A B C BM < 2.6 mmol/L Insert cannula Initial bloods (see list) Send lab glucose to confirm Put urine bag on to collect next urine passed DO NOT DELAY CORRECTION OF HYPOGLYCAEMIA WHILST AWAITING CONFIRMATION OF LABORATORY GLUCOSE IV Access? Yes No IV Bolus 10% dextrose 5mls/kg Drowsy? No Yes <1year - milk feed >1 year – 60ml lucozade Give im glucagon 0.5mg <3yr 1mg >3yr If not immediately able to recommence feeds/or if unwell - commence an IV glucose infusion using 10% dextrose/0.45% saline at a rate of 2.4 –4.8ml/kg/hr Recheck BM at 5 min interval until blood sugar stable >3mmol If unable to maintain BM >3mmol must have IV access BM < 2.6mmol/l Check cannula patent repeat 5ml/kg bolus 10% dextrose Increase rate up to 6ml/kg/hr 10%/0.18%dextrose saline Increase percentage dextrose in infusion -Central venous access if >12.5% dextrose If adrenal insufficiency suspected give Hydrocortisone 4mg/kg max. 100mg iv and inform consultant on call Monitor U&E’s regularly (see IV fluid guidelines) Becky Smith Page 3 BM>2.6mmol/l Continue maintenance fluids, if commenced Gradually reintroduce feeds IF BM falls to less than 3 mmol/l within 60 mins of a feed use continuous feeds Check pre-feed blood sugar If continuing IVI monitor U&E’s regularly (see IV fluid guidelines) Nov 2007 Paediatric Clinical Guideline 9.1 Endocrine: Hypoglycaemia Investigations for Hypoglycaemia Labels can be printed from NOTIS using the order set ‘Hypoglycaemia’ A specimen collection set is available as a package in the Emergency Department and on the Paediatric wards ONE x Fluoride oxalate (GREY) tube to be sent for: o o o o o o Glucose Lactate Plasma free fatty acids and ketones Beta hydroxybutyrate Alanine Carnitine THREE x Lithium heparin (GREEN) tube to be sent for: o Ammonia (single tube, inform lab as urgent and take to lab immediately) o Cortisol o Insulin and c-peptide o GH o Amino acids o U&E o LFT o Alcohol o Salicylates o Capillary Blood Gas Blood Cultures Urine (20mls sample required) dip for urine ketones and send for reducing substances organic and amino acids Guthrie card blood spot - for acylcarnitine. Glucose Infusion Calculator Glucose rate in mg / kg / min = % dextrose solution x ml/hr Weight x 6 To make up dextrose solutions of different concentrations add Final dextrose concentration required 10% 12.5% 15% 20% Becky Smith Add 37ml of 50% dextrose to a 500ml bag of dextrose 5% / 0.45% saline Available from Pharmacy ( no saline in bag will need U&E monitoring) Available from pharmacy Page 4 Nov 2007 Paediatric Clinical Guideline 9.1 Endocrine: Hypoglycaemia Fasting Provocation Test for hypoglycaemia A fasting provocation test is occasionally indicated to help establish a diagnosis. This should never be completed without consulting a paediatric endocrinologist and a separate protocol is available for this. Interpreting the Results of the Hypoglycaemia Screen Low Ketones Fatty acid oxidation defects Fatty acid: 3 hydroxybutyrate level >2 suggests Fatty acid oxidation defect Raised Insulin Hyperinsulinism of infancy Beckwith- Weidman syndrome Pancreatic islet cell adenoma Insulin poisoning Maternal diabetes Hyperammonia Maple syrup urine disease Proprionic acidaemia Methylmalonic acidaemia Tyrosinaemia Liver dysfunction Hyperinsulinism Metabolic acidosis Fatty acid oxidation defects MCAD, LCAD Defects in ketogenesis Sepsis Glycogen storage disorders Organic acid disorders Deranged LFT's Sepsis Liver disease Glycogen storage disease Galactosaemia Fat oxidation defects Hereditary fructose intolerance Low cortisol Adrenal insufficiency Congenital adrenal hyperplasia ACTH deficiency/ Hypopituitarism Low sodium + High Potassium Adrenal disorders GH deficiency Panhypopituitarism Isolated GH deficiency Raised lactate Metabolic liver disease Prolonged convulsion Glycogen storage disorders Sepsis Urine Specific amino or organic acid disorders Acylcarnitine Abnormal in fatty acid oxidation defects Becky Smith Page 5 Nov 2007 Paediatric Clinical Guideline 9.1 Endocrine: Hypoglycaemia Discharge Plan for Patient Admitted with Recurrent Hypoglycaemia Prior to discharge please ensure the following have been completed: Ensure dietetic input to agree a written management plan for the parents to take home (see sample attached) Check the family know how to treat hypoglycaemia with polycal solution / 60ml lucozade / 3 dextrose tablets as age appropriate and have im glucagon if needed Obtain an OPTIUM Blood Glucose monitor (from the diabetic nurse cupboard, keys on CSSU, or from Pharmacy) and ensure the family have been trained in how to use it. Prescribe any necessary medications, specialised feeds and the OPTIUM glucose strips and thin lancets needed to operate the blood glucose monitor Provide a written discharge summary for the GP including the information about treatments and the blood glucose monitor supplies that will need to be provided on a repeat prescription by the GP. Arrange out-patient follow-up with the paediatric endocrine team. Summary Hypoglycaemia is a common finding in paediatrics and should be investigated and treated promptly. All unwell children should have a blood sugar level checked. Children with a blood sugar reading <2.6mmol/l should be treated according to the above flow chart with appropriate investigations and ideally an intravenous dextrose infusion. Care needs to be taken to monitor serum electrolyte levels as well as the glucose regularly Children with a reduced level of consciousness should not be given oral treatment or feeds. All children should be observed until they have achieved a period of stable normoglycaemia on their usual feed regime. Becky Smith Page 6 Nov 2007 Paediatric Clinical Guideline 9.1 Endocrine: Hypoglycaemia Management Plan for Home Management of Hypoglycaemia (Low blood sugar levels) This management plan is for............................................................... Low blood glucose (hypoglycaemia) levels Less than .......... mmol/l Ideal blood glucose range .......... mmol/l - .......... mmol/l Usual symptoms are: Treatment to be given if blood sugar reading is low: Recheck blood sugar level after If blood sugar still low If blood sugar level now normal What to do when unwell If your child still has a low blood sugar that has not responded to treatment or if you have any queries please contact ………………………………………………………………………………………… IF YOUR CHILD IS UNCONCIOUS, FITTING OR DOES NOT RESPOND TO THE TREATMENT ABOVE CALL 999 AND ASK FOR AN AMBULANCE. Becky Smith Page 7 Nov 2007 Paediatric Clinical Guideline 9.1 Endocrine: Hypoglycaemia References 1. 2. 3. 4. 5. 6. 7. Morris AAM; Thekekara A; Wilks Z; Clayton PT; Leonard JV; Aynsley-Green A; Evaluation of fasts for investigating hypoglycaemia or suspected metabolic disease. Archives of Disease in Childhood. 1996;75(2):115-119 Wong CP; Forsyth RJ; Kelly TP; Eyre JA: Incidence, aetiology and outcome of nontraumatic coma: a population based study. Archives of Disease of Childhood. 2001;84(3):193-199 Bonham JR. Investigation of hypoglycaemia in childhood. Ann Clin Biochem 1993;30:238-247 Aynsley-Green A. Glucose, the brain and the paediatric endocrinologist. Hormone Res 1996;46:8-25 Glycaemic emergencies. BNF June 2004 Hypoglycaemia of the newborn. Review of the literature. WHO 2006 National metabolic biochemistry network. Guidelines for the investigation of hypoglycaemia in infants and children. November 2004. Becky Smith Page 8 Nov 2007