Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Learn more about Diabetes | PDF Hypoglycaemia
Hypoglycaemia - Low Blood Glucose level
Hypoglycaemia - a low blood glucose level - is a recurrent problem for many people with
diabetes, and it is frequently cited as being the main barrier to achieving good blood glucose
control in those people on insulin.
What's covered in these pages
What is Hypoglycaemia?
•
•
•
Who suffers from hypoglycaemia?
Why does hypoglycaemia occur in people with diabetes?
Can hypoglycaemia casuse death?
Short Term Effects of Hypoglycaemia
•
•
Signs and symptoms
Hypoglycaemia awareness
Treating Hypoglycaemia
•
•
•
Quick Fix Solution
Prevention is better than cure
Severe Hypoglycaemia
Nocturnal Hypoglycaemia
Long Term Effects of Hypoglycaemia
•
•
•
Fear of Hypoglycaemia
Loss of hypoglycaemia awareness
Changes in brain function
Normal Glucose Regulation and 'Counterregulation'
•
•
•
How does the body normally respond to a falling blood glucose level in people who do NOT
have diabetes?
'Counterregulation' in diabetes
Differences between men and women
Copyright © Karen Reed 2014
Learn more about Diabetes | PDF Hypoglycaemia
What is Hypoglycaemia?
Hypoglycaemia in people with diabetes is a low blood glucose level, causing a number of
unpleasant effects ranging from shaking, sweating and a racing heart beat, through to
behavioural changes, seizure and coma.
HYPOGLYCAEMIA (HYPO)
LOW BLOOD GLUCOSE LEVEL
less than 4.0 mmol/L
Tell people that you have diabetes
- it could save your life!
Carry Diabetic ID at all times...
Consider joining the MedicAlert program.
Or try some other form of
medical ID jewelry.
Who suffers from hypoglycaemia?
All people with any type of diabetes can potentially suffer mild forms of hypoglycaemia,
including symptoms related to a rapidly falling or lower than normal* blood glucose level.
However, significant hypoglycaemia is usually only suffered by those people taking insulin,
or drugs that increase insulin production/action, for the management of blood glucose.
* Some symptoms of hypoglycaemia can be felt at a normal or even
high-normal blood glucose level if you have been running high for a
significant period of time. Equally, a rapidly falling blood glucose
level can elicit symptoms of hypoglycaemia before levels drop
below 4 mmol/L.
Why does hypoglycaemia occur in people with diabetes?
Diabetes is generally associated with a high blood glucose level. However, when treated
with insulin, or tablets that increase natural insulin activity, diabetes becomes a delicate
balancing act, and, because of the multitude of factors that affect blood glucose levels, total
normalisation of blood glucose is just not possible.
Copyright © Karen Reed 2014
Learn more about Diabetes | PDF Hypoglycaemia
There are a whole host of factors that affect blood glucose levels and if these are not
precisely balanced with insulin reaching the bloodstream (either from the pancreas, or from
the injection site) on an hour-by-hour, minute-by-minute basis, then the blood glucose level
may fall outside the normal range. If it drops too low, hypoglycaemia results. People with
diabetes frequently refer to this experience as "having a hypo", "going hypo", “having a low”
or “going low”.
COMMON FACTORS THAT AFFECT BLOOD GLUCOSE LEVELS
Lowers blood glucose
Raises blood glucose
Insulin*
Sulphonylurea or
meglitinide tablets (see
"Tablets for Type 2's")
Exercise
Alcohol
*Massage, exercise, or a
warm bath may increase
insulin absorption from the
injection site and cause a
rapid lowering of blood
glucose
Food - especially
carbohydrates
Emotional stress
Illness, any infection
Pregnancy
Some medications
Dawn effect (a rising blood
glucose early in the
morning)
Variable effect on blood glucose level
Monthly periods in women
Some types of stress
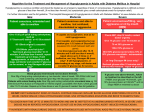
Common causes of hypos in people with diabetes therefore include the following:
•
•
•
•
•
Too much insulin
Too high a dose of diabetes tablets
Lack of food (carbohydrates)
Exercise
Alcohol
Copyright © Karen Reed 2014
Learn more about Diabetes | PDF Hypoglycaemia
Can hypoglycaemia cause death?
It is rare, but yes - hypoglycaemia can cause death. Some reports suggest that as many as 24 % of deaths of people with Type 1 diabetes may have been attributed to hypoglycaemia
(1, 2). Deaths related to hypoglycaemia induced by certain sulphonylurea tablets have also
been reported (3, 4)
Short Term Effects of Hypoglycaemia
Glucose is the preferred fuel for the brain. However, the brain cannot make glucose, and
can only store a few minutes' supply in the form of glycogen - so it is entirely dependent on
a continuous supply of glucose via the bloodstream. When the level of glucose in the blood
falls below a certain level, the brain - the body's control centre - starts to malfunction.
Signs and symptoms
Signs of hypoglycaemia are recognisable clinical changes in an individual that are either
visible or measured. Symptoms of hypoglycaemia are descriptive terms for what the person
experiences. Signs and symptoms are caused by the direct and indirect effects that low
blood glucose levels have on the nervous system.
The table on page 5 shows how symptoms are classified by the medical profession. As a
person with diabetes, your main objective is to recognise the symptoms early on, do a blood
glucose test to verify that your blood glucose is low, then take appropriate action as quickly
as possible.
Hypoglycaemia awareness
Recognising the signs and symptoms of diabetes is "hypoglycaemia awareness". If you
realise that your blood glucose level is starting to fall and you take action to correct it (i.e. have some glucose, see below) then, apart from some inconvenience, all should be well.
However if you fail to realise that your blood glucose level is dropping until it gets too a very
low level, then we call this a loss of hypoglycaemia awareness. This may make you
susceptible to severe hypoglycaemia, which can be dangerous and is potentially lifethreatening.
If you are unable to detect mild hypoglycaemia from symptoms alone, you should:
•
•
•
•
•
•
Increase the number of times you test your blood glucose each day
Consider snacking more often or eating more regular meals
Always test your blood glucose level before driving or using potentially dangerous
equipment
Discuss the situation with your diabetes healthcare team
Educate your friends, relatives, and co-workers about hypoglycaemia so that they can
recognise the condition
Keep a glucagon injection kit to hand (see 'severe hypoglycaemia' below)
Copyright © Karen Reed 2014
Learn more about Diabetes | PDF Hypoglycaemia
CLASSIFICATION OF
SYMPTOMS OF HYPOGLYCAEMIA
INDIRECT EFFECTS
DIRECT EFFECTS
Neurological responses
Physiological responses
Result of the perception of physiological
changes caused bythe activation of the
autonomic nervous system triggered by
hypoglycaemia
Result of direct effects of low blood glucose
on the brain - limits neuronal metabolism i.e. the nerves are starved of glucose
"Autonomic" or "NEUROGENIC"
symptoms
•
•
•
•
Sweating
Shakiness
Palpitations
Hunger, or a compulsion to eat
"NEUROGLYCOPENIC" symptoms
•
•
•
•
•
Confusion
Drowsiness
Uncharacteristic behaviour
Difficulty with speech
Loss of coordination
In addition, some symptoms come under the rather vague heading of "GENERAL
MALAISE" - these include:
•
•
Headache
Nausea
Treating Hypoglycaemia
Quick Fix Solution
The treatment for a low blood glucose level is simple - Glucose! You can use glucose powder
or tablets. (Don't be confused by the term 'dextrose' - it's the same thing as glucose.) 10 or
15g of glucose should be taken immediately. Then wait 5 minutes before having some other
form of carbohydrate - biscuits, or a muesli bar, for example.
It's a good idea to keep some blood glucose boosters with you at all times. Glucose tablets,
jelly beans, and hard candies are compact, portable, and last a long time in desks, purses,
lockers, and glove compartments.
Copyright © Karen Reed 2014
Learn more about Diabetes | PDF Hypoglycaemia
Depending on what caused the hypoglycaemia and when you will eat your next meal, you
may need to have an extra starchy snack - a sandwich or cereal bar, for example - to keep
you going.
If a person is unable (or unwilling) to treat the hypoglycaemia themselves, then help may be
needed in the form of a glucagon injection. Glucagon is a natural hormone, which raises the
blood glucose level by encouraging the liver to release glucose into the bloodstream. It can
be injected by a friend or family member, or, in the worst-case scenario, by a paramedic.
"Prevention is Better Than Cure"
In order to prevent hypoglycaemia whenever possible, it is necessary to understand why it
happens and when it is most likely to happen: then you should be able to take appropriate
action to keep your blood glucose level above 4 mmol/l.
Hypoglycaemia has many causes:
•
•
•
•
•
Too much insulin or diabetes medication - these treatments stimulate the cells to remove too
much glucose from the blood.
Too little food, particularly carbohydrates - if you don't eat regularly, you may not consume
enough food to keep blood glucose levels within the normal range. Delayed or missed meals
are the most common cause of hypoglycaemia.
Too much exercise - exercise uses up blood glucose.
Drinking alcohol - alcohol lowers blood glucose levels. Usually, as blood glucose levels fall,
the liver releases stored glucose into the bloodstream. But alcohol interferes with this
process. It is particularly dangerous for people with diabetes to drink on an empty stomach.
Blood glucose levels can fall so fast so quickly that you may lose consciousness quite
suddenly.
Pregnancy - pregnancy often makes women less aware of hypoglycaemia. Pregnancy also
involves eating for two, which may require substantial changes in food intake and insulin
doses.
Hypoglycaemia is most likely to occur:
•
•
•
•
•
Just before meals, when blood glucose is naturally low
During or after strenuous exercise
When insulin is peaking
When you suspend your usual daily routines, particularly if your alcohol intake increases
while your food intake falls
At night, particularly if you've been more active the day before, eaten less or consumed
alcohol during the evening
Regular testing of your blood glucose level
is key to understanding and preventing hypos.
Copyright © Karen Reed 2014
Learn more about Diabetes | PDF Hypoglycaemia
Severe hypoglycaemia
Severe hypoglycaemia is usually defined as that 'requiring assistance from another person'.
It is usually necessary to trest severe hypoglycaemia with glucagon (see "Treating Hypos"
above).
Nocturnal Hypoglycaemia
Nighttime hypoglycaemia can be a problem for some people if they do not wake up.
Common signs include damp sheets and pyjamas, nightmares, crying out in sleep, or feeling
tired, irritable or confused on waking. A high early morning blood glucose level sometimes
indicates hypoglycaemia during the night - the liver is stimulated to release glucose and
'overcompensates'.
To minimise risk of nighttime hypoglycaemia, test your blood glucose level periodically
between 2 and 3 a.m. Determine how your level relates to your food, exercise, and insulin
or medication the previous day and adjust them accordingly.
* Fits are quite common in young children, especially if hypoglycaemia occurs during the
night. Don't worry - this is not epilepsy and generally causes no serious damage. As children
grow older the fits become less frequent and most children grow out of them altogether.
Longer Term Effects of Hypoglycaemia
In the long term, hypoglycaemia may repeatedly reduce or interefere with physical and
mental functioning, with the potential to significantly affect social functioning.
Psychologically, hypoglycaemia - particularly severe hypoglycaemia - can have devastating
effects in the long run.
Fear of Hypoglycaemia
Hypoglycaemia can be an unpleasant experience, and as a result some people suffer anxiety
or fear of hypoglycaemia (FoH). This is a clinically recognised condition (8) and may be quite
widespread amongst people with diabetes. Some people may go to extreme lengths in order
to avoid having hypoglycaemia (e.g. missed or reduced insulin injections). Poor metabolic
control and emotional/psychological problems inevitably result from (FoH).
Copyright © Karen Reed 2014
Learn more about Diabetes | PDF Hypoglycaemia
Recognising and accepting the prolem is the first step in overcoming FoH. Blood glucose
awareness training and cognitive behavioural therapy can help to improve the situation.
Support from family and friends helps too.
Loss of hypoglycaemia awareness
As a rule, warning signs of a hypo are experienced as the blood glucose level starts to drop.
These might include sweating, shaking or hunger. It has been noted in many cases that
gradually, over a period of years, these warning signs start to come on later. This means that
the blood glucose may fall very low before the individual becomes aware of the situation
and realises that he/she needs to take glucose. People with hypoglycaemia unawareness
may suffer from repeated severe hypos, and may be at risk of fitting or unconsciousness.
It's a vicious circle!
Hypoglycaemia itself can have the effect of reducing
hypoglycaemia awareness - in effect this means that
once you've had a hypo, you're more likely to have
another one.
To get out of the vicous circle blood glucose levels
may need to be kept slightly higher than you would
otherwise aim for - in order to avoid hypoglycaemia.
After a few days warning signs should return to
normal.
Factors relating to loss of hypo awareness are considered in more depth in the section on
page 9, 'Normal Glucose Regulation and Counterregulation'
Changes in brain function
Recently another long term problem associated with hypoglycaemia has come to light.
Some people who have had Type 1 diabetes for many years seem to have suffered from
damage to the frontal lobes in the brain and this is thought to be related to frequent or
severe episodes of hypoglycaemia over time. As a result, these people appear to suffer from
lack of concentration, poor judgment, a loss of reasoning and a reduced ability to interact
with other people.
Many such people also have signs of the more well-defined complications outlined above; it
is possible that nerve damage in particular, might add to the problem.
Recurrent severe hypoglycaemia in young children has also been reported to affect learning
and development to some extent in certain individuals. However, on a positive note, a study
Copyright © Karen Reed 2014
Learn more about Diabetes | PDF Hypoglycaemia
carried out in Australia (5) suggested that "seizures/coma at a young age does not
necessarily result in gross cognitive or behavioural impairment."
Finally, although severe prolonged hypoglycaemia can potentially cause some degree of
permanent brain damage, it is rare - complete recovery is the general rule (6).
Normal Glucose Regulation and 'Counterregulation'
How does the body normally respond to a falling blood glucose level in people who do
NOT have diabetes?
People who do not have diabetes rarely encounter significant hypoglycaemia, even after
prolonged fasting. This is because the body has an excellent defence mechanism - called
counterregulation - which is triggered as the blood glucose level falls below a certain
threshold.
So, normally, as the blood glucose level reaches this glycaemic threshold (see box), the
automatic production of the hormones glucagon and epinephrine (adrenalin), act to raise
the blood glucsoe and a normal blood glucose level is quickly restored.
GLYCAEMIC THRESHOLDS FOR HYPOGLYCAEMIA
Counterregulation activated in
people who do NOT have
diabetes
3.8 mmol/L
(healthy young
adult)
Onset of symptomatic responses
3.0 mmol/L
Onset of brain ('cognitive')
dysfunction
2.8 mmol/L
Counterregulation in people who do NOT have diabetes prevents the blood glucose from
falling to levels low enough to cause symptoms. (Counterregulatory responses in people
who DO have diabetes are actually responsible for a number of the symptoms experienced.)
Copyright © Karen Reed 2014
Learn more about Diabetes | PDF Hypoglycaemia
'Counterregulation' in diabetes
In peole with diabetes, the counterregulatory response is impaired, particularly in those
poeple with Type 1 diabetes. Research suggests that after about 5 years of being diagnosed
with Type 1 diabetes, most people will have a defective glucagon response to
hypoglycaemia. This means that the liver does not top up the falling blood glucose level as it
should normally do. Further, with repeated episodes of hypoglycaemia, the epinephrine
response can become blunted and this is associated with loss of hypoglycaemic awareness,
i.e. loss of warning signs. Interestingly, reports suggest that this effect may be greater in
men than in women.
Counterregulatory responses in people who have diabetes are related to a number of
the symptoms experienced. Blunting of these responses in diabetes reduces the level
of blood glucose at which symptoms are experienced and this is associated with the
development of 'hypoglycaemia unawareness'.
Hypoglycemia-associated autonomic failure (HAAF) is a functional disorder distinct
from classic diabetic autonomic neuropathy. It is a dynamic phenomenon that can be
induced (by prior hypoglycemia) and reversed (by avoidance of hypoglycemia) and is
manifested clinically by recurrent iatrogenic hypoglycemia.
The combination of reduced counterregulatory mechanisms and hypoglycaemia
unawareness significantly increases the risk of severe hypoglycaemia.
Differences between men and women
Women have been shown to have significant reductions in the critical counterregulatory
hormones, glucagon and epinephrine, together with blunted rates of endogenous glucose
production, compared to men. When fasting, women's blood glucose levels fall lower than
men. So why is it that women with Type 1diabetes don't suffer hypoglycaemia more often
than men? The DCCT data have shown that, if anything, women have a reduced risk of
severe hypoglycemia during intensive therapy compared to men. Researchers in Tennessee
(7) suggest that:
1) antecedent hypoglycemia produces less blunting of counterregulatory responses to
subsequent hypoglycemia in women relative to men;
2) two episodes of antecedent hypoglycemia can overcome the greater SNS response to
hypoglycemia usually found in men; and
3) the reduced susceptibility of women to the blunting effects of antecedent hypoglycemia
may be the mechanism explaining why, despite inherently reduced SNS counterregulatory
responses, female type 1 DM patients have a similar prevalence of hypoglycemia compared
to men.
Copyright © Karen Reed 2014
Learn more about Diabetes | PDF Hypoglycaemia
References
1. Cryer PE. Hypoglycemia. Pathophysiology, Diagnosis and Treatment. New York, Oxford
University Press, 1997.
2. Laing SP, Swerdlow AJ, Slater SD, Botha JL, Burden AC, Waugh NR, Smith AW, Hill RD,
Bingley PJ, Patterson CC, Qiao Z, Keen H. Diabet Med. 1999 Jun;16(6):466-71.The British
Diabetic Association Cohort Study, II: cause-specific mortality in patients with insulin-treated
diabetes mellitus.
3. Campbell IW. Hypoglycaemia and type 2 diabetes: sulphonylureas. In 'Hypoglycaemia and
Diabetes:Clinical and Physiological Aspects'. Frier B, Fisher BM Eds. London, Edward Arnold,
1993; p387-92.
4. Gerich JE. Oral hypoglycemic agents. N Engl J Med. 1989 Nov 2;321(18):1231-45 [Erratum
in:N Engl J Med 1990 Jan 4;322(1):71]
5. Strudwick SK, Carne C, Gardiner J, Foster JK, Davis EA, Jones TW. Cognitive functioning in
children with early onset type 1 diabetes and severe hypoglycemia. J Pediatr. 2005
Nov;147(5):680-5.
6. Cryer PE, Davis SN, Shamoon H. Hypoglycemia in diabetes. Diabetes Care. 2003
Jun;26(6):1902-12.
7. Davis SN, Shavers C, Costa F. Gender-related differences in counterregulatory responses
to antecedent hypoglycemia in normal humans. J Clin Endocrinol Metab. 2000
Jun;85(6):2148-57.
8. Wild D, von Maltzahn R, Brohan E, Christensen T, Clauson P, Gonder-Frederick L. A critical
review of the literature on fear of hypoglycemia in diabetes: Implications for diabetes
management and patient education. Patient Educ Couns. 2007 Sep;68(1):10-5. Epub 2007
Jun 19.
Copyright © Karen Reed 2014