Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
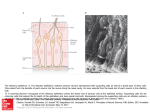
15a – Histo of Nose, Teeth, Throat I – McWho - - - Nose Functions o Olfaction o Respiration o Filtration of dust o Humidification and warming of inspired air o Reception and elimination of secretions from the paranasal sinuses and nasolacrimal ducts Nasal Cavity o Opens posteriorly into nasopharynx through choanae o Inferior 2/3rds = respiratory area o Superior 1/3rd = olfactory area o Opens anteriorly through nares Divided into two chambers by cartilaginous septum Each Chamber has two parts Vestibule – most anterior, dilated part – o Skin - Stratified squamous keratinized to nonkeratinized epithelium o Vibrissae filter inspired air o Sebaceous and sweat glands o Cartilage supports medial septum and lateral wall Nasal fossa – most posterior, narrow part o Respiratory epithelium – pseudo-stratified, ciliated, columnar w/ goblet cells o Bony shelf-like projections – conchae – extend from lateral wall o Superior concha covering by olfactory epithelium o Middle and inferior conchae covered by respiratory epithelium 5 Cell types of Respiratory Epithelium – all contact basement membrane o Ciliated columnar Most numerous ~300cilia/cell Move mucus w/ its trapped particulate matter toward pharynx or elimination. Immotile Cilia Syndrome – infertility in men and chronic respiratory –tract infections in both sexes. Immobility of cilia and flagella. Dynein deficiency – protein involved in ciliary movement o Goblet Second most numerous – narrow base and expanded apex. Contains large, light staining granules Hydrophilic glycoproteins – mucins Extracellularly mucus – viscous protective lubricating gel Population tapers off in terminal bronchioles Dried Nasal Mucus – Boogers - During sinus or lung infection – dried mucus also contains dead wbc’s. Rhinotilexomania – booger picking habit o Brush Apex contain mmicrovilli Base has afferent nerve ending Sensory receptors of general sensation – two types of brush cells recognized, second type thought to be a stem cell o Basal Small round stem cells Give rise to ciliated, columnar, goblet and brush Lie on basal lamina but DO NOT REACH lumen o Small granule Resemble basal cells Numerous granules Exhibit dnes activity – may modulate mucous and serous secretory activit o Smoker’s Respiratory Epithelium Undergoes metaplasia changing to stratified squamous – offers better protection. Decrease in ciliate columnar cells – decrease in movement of mucous Increase in goblet cells – protect against pollutants Congestion of smaller airways Smoker’s Melanosis – benign focal pigmentation of oral mucosa. Tends to increase significantly w/ tobacco consumption. Olfactory Epithelium – roof of nasal cavity o Covers superior conchae bilaterally and sends axons to brain via small openings in cribriform plate of ethmoid bone o Pseudostratified epithelium – Olfactory Epithelium Basal Stem Small spherical or cone-shapeed – form layer at the basal lamina Stem cells for the other two cell types Columnar support Columnar shaped with broad cylindrical apexes and narrower bases Mmicrovilli on free surface submerged in fluid layer Junctional complexes bind them to olfactory cells Role not well understood – express abundant ion channels whose function appears to be required to maintain a microenvironment conducive to olfactory function and survival. Bipolar olfactory neurons Dendrites at luminal ends – cilia specialized with receptors for odor molecules Binding ligands causes depolarization that passes along basal axons to olfactory bulb of brain - - - Distinguished from supporting cells by position of nuclei – between those of supporting cells and basal cells Dendritic end of each is apical (luminal) pole of cell – knoblike swelling with about a dozen basal bodies, long motile cilia with defective axopemes emerge and create surface area Azons of these neurons leave epithelium and unite in lamina propria – very small nerves that then pass through foramina in cribriform plate Lamina propria – possesses large serous glands of bowman – produce flow of fluid surrounding olfactory cilia and facilitating access of new odoriferous substances Rhinitis – inflammation of inner lining of nose – nasal mucosa due to allergens and non-allergens o Rxn can occur in eyes, nose, throat when airborne irritants trigger release of histamine Causes inflammation and fluid production in fragile linings of nasal passages, sinuses and eyelids Symptoms usually include – sneezing, congestion, runny nose, itchy nose, throat, eyes and ears Sternutation – Sneeze o Protective reflex triggered by a variety of stimuli o Most common stimuli – irritation of nasal mucosa – CN V by mechanical or chemical stimuli. Also, exposure to bright or blue light and male orgasm o Sudden explosive expulsion of air clears nasal passage of irritant o Sneezing center is in medulla oblongata at ventromedial margin of descending tract and nucleus (spinal nucleus) of CN V – includes adjacent reticular formation and nucleus solitarius o Two phases Nasal phase – afferent limb consists of ethmoidal CNV and olfactory CN I nerves that project to medulla. Efferent limb consists of preganglionic fibers to greater petrosal nerve CCN VII and the sphenopalatine ganglion CN VII that innervate glands and bv in nose, resulting in secretion and edema, further stim of mucosa and more impulses to sneezing center Respiratory Phase – commences when critical number of inspiratory and expiratory neurons are recruited by sneezing center. Recruitment of these neurons increases activity in vagus, phrenic and intercostal nerves. Consequences – Eye closure deep inspiration pharyngeal closure forceful expiration dilation of the glottis explosive air release through mouth and nose expulsion of mucus and irritants Epistaxis – Nosebleed o Relatively common – rich supply of blood to nasal mucosa o Kiesselbach Area – anterior 1/3rd of nose. - - Site of anastomosis of arterial supply of nasal mucosa Bleeding may be arrested by applying pressure on the region or by packing the nasal cavity w/ cotton Associated w/ infections and hypertension Spuring of blood results from rupture of arteries Mild epistaxis may be result of nose picking which tears veins in vestibule of nose Paranasal Sinuses o Frontal o Ethmoid Most commonly associated in children sinusitis o Sphenoid o Maxillary Most commonly associated in adult sinusitis – very high osteum – difficult to drain. o Role is debated, but some functions likely Reduce skull weight Increase resonance of voice Provide buffer against blows to face Insulate sensitive structures like dental roots and eyes from rapid temp fluctuation in nasal cavity Humidify and heat inhaled air Regulations of intranasal and serum gas pressures Immunological defense o Sinusitis – inflammation of mucous membrane of any sinus Swelling obstructs sinus openings, preventing mucus from draining normally facial pain Blocked sinuses create moist environment easier for infection to take hold Can’t drain, become pus filled – nasty discharge Taste Buds detect at least 5 broad categories of tastants o Metal ions – salty o Hydrogen – sour o Sugars and related organic compounds – sweet o Al;kaloids and toxins – bitter o Glutamate aa – umami – savory All parts of tongue are sensitive to all kinds of tastants, however some areas are more sensitive to certain taste qualities Tip = sweet Lateral surfaces = salt and sour Posterior = bitter 15b – Histo of Nose, Teeth, Throat II – McWho - - Oral Cavity o Two Parts Oral Vestibule – slit like space between teeth and buccal gingival and lips and cheeks Oral Cavity Proper – where food and drinks are tasted and savored and where mastication and lingual manipulation of food occur o Tongue Extreme mobility Intrinsic – alter shape of tongue Extrinsic – move tongue in/out and side to side Covered by mucous membrane Roles Mastication, taste, swallowing, articulation, oral cleansing Terminal Groove – divides tongue into lingual tonsil and anterior part o Tongue Papillae - gestation Filiform – most numerous, entire surface of tongue Conical-Feathery shape Keratinized epithelium Scrape food off of surface NO taste buds Fungiform Resemble mushrooms Interspersed among filiform papillae – most numerous at apex and sides Contain taste buds Foliate Small posterolateral folds, appear as vertical furrows Contain taste buds Circumvallate or Vallate Least numerous and largest – 7-12 large circular papillae surrounded by moat like trenches Just anterior to terminal groove o Ducts of serous salivary von ebner glands – drain contents in to moat Secretion continuously flows over taste buds – removal of food particles from vicinity of taste buds so that new stimuli can come Secrete lipase – prevents hydrophobic layer over taste buds that would hinder function Taste – olfactory, taste and somatosensory = flavor o Olfaction – odors that result for odorous substances aerolized in environment o Taste – sensation evoked by stimulation of taste receptors in oropharyngeal cavity o Somatosensory – experience of lavor by detecting irritating components in smells like ammonia or the “hot” in spicy food like peppers – thermal, tactile, common chemical sense – relayed to brain via CN V - - Taste Buds – Ovoid structures – 50-75 cells, w/in stratified epithelium of tongue and oral mucosa o 7-10 day lifespan – 50% light o Others – slender supportive – DARK, immature, function poorly understood o Basal stem cells – divide and give rise to two other types o Base of each bud rests on basal lamina and is entered by afferent sensory axons that form synapses on the gustatory cells o Microvilli project through and opening called taste pore o Molecules (tastants) dissolved in saliva contact microvilli through pore and interact w/ cell surface taste receptors Teeth o Numbered from top R L, then bottom L R o 2-1-2-3 (molars) 32 total o Primary = 2-1-2 (no molars) 20 total Enamel – covers crown portion – hardest surface in body 95% hydroxyapatite – 5% organic material and water – tyrosine rich glycoproteins – amelogenins and enamelins Amenoblasts – make enamel, die before tooth erups, body cannot repair enamel Susceptibility to acidic pH is basis for dental caries – dry rot Dentin – makes up bulk of tooth Forms bulk of tooth Second hardest surface 70% hydroxyapatite 30% organic material and water – type 1 collagen w/ associated proteoglycans and glycoproteins Odontoblasts – make dentin, remain viable for life of tooth, can be repaired, located at periphery of pulp Cement – covers root portion Outer layer of roots, overlies dentin Anchors periodontal ligament to roots of tooth Approximately as hard as bone 50% hydroxyapatite 50% organic material and water – type 1 collagen w/ associated… Cementoblasts – make cementum, viable for life of tooth Pulp Cavity – consists of soft gelatinous connective tissue w/ nerves and blood vessels Center of tooth Covered by dentin Bv’s and nerves Loose connective tissue Continous w/ root canal and apical foramen Odontoblasts occupy periphery of pulp cavity Periodontal Ligament Located between cementum of root and bony alveolus Hold tooth in place Act as shock absorber Composed of dense, irregular collagenous connective tissue Mainly type I collagen, ends embedded in alveolus and cementum – sharpey’s fibers Alveolar bone – is bony socket of jaw bones that house roots of tooth o Associated Structures of Teeth Gingiva Mucous membrane firmly bound to periosteum of jaw bones Composed of stratified squamous epithelium covering Dense, irregular collagenous connective tissue core Attached to enamel by Junctional epithelium Thin wedge shaped stratified squamous nonkeratinized epithelium Gingival Sulcus – between enamel and gum, depth may indicated periodontal disease Depth of gingival sulcus measured during clinical dental exams is an important indicator of potential periodontal disease Periodontal Gum Disease – o Gingivitis – gum inflammation o Periodontis – damage to soft tissue and bone that support teeth. o Plaque build up tartar o Dental Caries, Pulpitis and Tooth Abscesses Decay of hard tissues of tooth results in formation of caries Tx involves removal of the decayed tissue and restoration of anatomy of tooth with dental material Neglected caries invade and inflame pulp cavity Invasion of pulp by deep carious lesion infection and irritation of tissues Pulp is rigid space, swollen tissues cause considerable pain – toothache If untreated, the small vessels in root canal may die from pressure of swollen tissue and the infected material may pass through apical canal and foramen into periodontal tissues Infective process develops and spreads through the root canal to alveolar bone producing abscess Pus from an abscess of a maxillary molar tooth may extend into nasal cavity or maxillary sinus Roots of maxillary molar teeth are closely related to floor of sinus - As a consequence, infection of the pulp cavity may also cause sinusitis or sinusitis may stimulate nerves entering the teeth and simulate a toothache o Extraction of Teeth Wisdom teeth – often impacted, can cause problems, pain Must be careful not to injure alveolar nerves during extraction Fauces – Throat o Throat is the passage from the mouth to the pharynx Bounded – Superiorly by the soft palate Inferiorly by the root of the tongue Laterally by the palatoglossal and palatopharyngeal arches Isthmus of the fauces is Short constricted space that establishes the connection between o Oral cavity proper and oropharynx Bounded o Anteriorly by the palatoglossal fols o Posteriorly by the palatopharyngeal folds o Pharynx Transitional area between oral cavity and respiratory and digestive systems Roles – food to digestive system, air to respiratory system Extends from – base of skull to inferior border of cricoid cartilage Divide into three parts Nasopharynx – lined w/ respiratory epithelium Oropharynx* Laringopharynx* o *Lined by stratified nonkeratinized squamous epithelium o Clinical use of the term Fauces includes the following structures Esophagous/Larynx – voice box/Trachea – windpipe/Tonsils o Tonsillitis is inflammation of the tonsils – mostly viruses, most common in younger folks Signs and symptoms include Swollen tonsils Sore throat and difficulty swallowing Most cases of tonsillitis are caused by infection with a common virus, but a bacterial infection also may cause Because appropriate treatment for tonsillitis depends on the cause, it’s important to get a prompt and accurate Dx Surgery to remove tonsils, once a common procedure to Tx tonsillitis is usually performed only when tonsillitis occurs frequently, doesn’t respond to other Tx or causes serious complications o Strep Throat – a bacterial infection in the throat and tonsils Sudden, severe, pain swallowing, fever > 101, swollen tonsils and lymph nodes; white or yellow spots on back of a bright red throat; may also have a HA and belly pain 2-5days incubation; 3-7 days goes away w/ or w/out Tx