Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
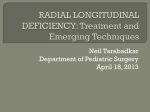
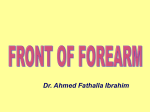
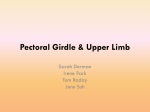
378 CHAPTER 9 The Upper Limb ligament of the elbow joint. It continues downward to enter the forearm between the two heads of origin of the flexor carpi ulnaris (see page 390). Branches The ulnar nerve has an articular branch to the elbow joint (Fig. 9.23). Profunda Brachii Artery The profunda brachii artery arises from the brachial artery near its origin (Fig. 9.45). It accompanies the radial nerve through the spiral groove, supplies the triceps muscle, and takes part in the anastomosis around the elbow joint. Superior and Inferior Ulnar Collateral Arteries The superior and inferior ulnar collateral arteries arise from the brachial artery and take part in the anastomosis around the elbow joint. laterally and the brachialis muscle medially. The roof is formed by skin and fascia and is reinforced by the bicipital aponeurosis. Contents The Cubital Fossa The cubital fossa (Fig. 9.47) contains the following structures, enumerated from the medial to the lateral side: the median nerve, the bifurcation of the brachial artery into the ulnar and radial arteries, the tendon of the biceps muscle, and the radial nerve and its deep branch. The supratrochlear lymph node lies in the superficial fascia over the upper part of the fossa, above the trochlea (Fig. 9.40). It receives afferent lymph vessels from the third, fourth, and fifth fingers; the medial part of the hand; and the medial side of the forearm. The efferent lymph vessels pass up to the axilla and enter the lateral axillary group of nodes (Fig. 9.40). The cubital fossa is a triangular depression that lies in front of the elbow (Figs. 9.47 and 9.48). Bones of the Forearm The forearm contains two bones: the radius and the ulna. Boundaries ■■ ■■ Radius Laterally: The brachioradialis muscle Medially: The pronator teres muscle The base of the triangle is formed by an imaginary line drawn between the two epicondyles of the humerus. The floor of the fossa is formed by the supinator muscle biceps brachii tendon biceps cubital fossa brachii bicipital brachioradialis aponeurosis cephalic vein basilic vein palmaris longus flexor digitorum superficialis flexor carpi radialis site fo palpati of radi artery flexor carpi ulnaris pisiform bone FIGURE 9.48 The cubital fossa and anterior surface of the forearm in a 27-year-old man. The radius is the lateral bone of the forearm (Fig. 9.49). Its proximal end articulates with the humerus at the elbow joint and with the ulna at the proximal radioulnar joint. Its distal end articulates with the scaphoid and lunate bones of the hand at the wrist joint and with the ulna at the distal radioulnar joint. At the proximal end of the radius is the small circular head (Fig. 9.49). The upper surface of the head is concave and articulates with the convex capitulum of the humerus. The circumference of the head articulates with the radial notch of the ulna. Below the head, the bone is constricted to form the neck. Below the neck is the bicipital tuberosity for the insertion of the biceps muscle. The shaft of the radius, in contradistinction to that of the ulna, is wider below than above (Fig. 9.49). It has a sharp interosseous border medially for the attachment of the interosseous membrane that binds the radius and ulna together. The pronator tubercle, for the insertion of the pronator teres muscle, lies halfway down on its lateral side. At the distal end of the radius is the styloid process; this projects distally from its lateral margin (Fig. 9.49). On the medial surface is the ulnar notch, which articulates with the round head of the ulna. The inferior articular surface articulates with the scaphoid and lunate bones. On the posterior aspect of the distal end is a small tubercle, the dorsal tubercle, which is grooved on its medial side by the tendon of the extensor pollicis longus (Fig. 9.49). The important muscles and ligaments attached to the radius are shown in Figure 9.49. Ulna The ulna is the medial bone of the forearm (Fig. 9.49). Its proximal end articulates with the humerus at the elbow joint and with the head of the radius at the proximal Basic Anatomy 379 capsule of elbow joint olecranon process radial notch of ulna a coronoid process triceps anc anconeus brachialis pronator teres head neck bicipital tuberosity biceps brachii biceps flexor pollicis longus supinator aponeurosis for extensor and flexor carpi ulnaris oblique cord supinator flexor digitorum flexor digitorum superficialis abductor pollicis longus profundus extensor pollicis longus pronator teres interosseous membrane flexor pollicis longus extensor pollicis brevis extensor indicis pronator quadratus aperture for anterior interosseous artery dorsal tubercle of radius brachioradialis styloid process styloid process capsule of wrist joint anterior surface posterior surface FIGURE 9.49 Important muscular and ligamentous attachments to the radius and the ulna. radioulnar joint. Its distal end articulates with the radius at the distal radioulnar joint, but it is excluded from the wrist joint by the articular disc. The proximal end of the ulna is large and is known as the olecranon process (Fig. 9.49); this forms the prominence of the elbow. It has a notch on its anterior surface, the trochlear notch, which articulates with the trochlea of the humerus. Below the trochlear notch is the triangular coronoid process, which has on its lateral surface the radial notch for articulation with the head of the radius. The shaft of the ulna tapers from above down (Fig. 9.49). It has a sharp interosseous border laterally for the attachment of the interosseous membrane. The posterior border is rounded and subcutaneous and can be easily palpated throughout its length. Below the radial notch is the supinator crest that gives origin to the supinator muscle. At the distal end of the ulna is the small rounded head, which has projecting from its medial aspect the styloid process (Fig. 9.49). The important muscles and ligaments attached to the ulna are shown in Figure 9.49. Bones of the Hand There are eight carpal bones, made up of two rows of four (Figs. 9.51 and 9.52). The proximal row consists of (from lateral to medial) the scaphoid, lunate, triquetral, and pisiform bones. The distal row consists of (from lateral to medial) the trapezium, trapezoid, capitate, and hamate bones. Together, the bones of the carpus present on their anterior surface a concavity, to the lateral and medial edges of which is attached a strong membranous band called the flexor retinaculum. In this manner, an osteofascial tunnel, the carpal tunnel, is formed for the passage of the median nerve and the flexor tendons of the fingers. The bones of the hand are cartilaginous at birth. The capitate begins to ossify during the first year, and the others begin to ossify at intervals thereafter until the 12th year, when all the bones are ossified. A detailed knowledge of the bones of the hand is unnecessary. The position, shape, and size of the scaphoid bone, however, should be studied, because it is commonly fractured. The ridge of the trapezium and the hook of the hamate should be examined. 380 CHAPTER 9 The Upper Limb C L I N I C A L N O T E S Fractures of the Radius and Ulna Fractures of the head of the radius can occur from falls on the outstretched hand. As the force is transmitted along the radius, the head of the radius is driven sharply against the capitulum, splitting or splintering the head (Fig. 9.10). Fractures of the neck of the radius occur in young children from falls on the outstretched hand (Fig. 9.10). Fractures of the shafts of the radius and ulna may or may not occur together (Fig. 9.10). Displacement of the fragments is usually considerable and depends on the pull of the attached muscles. The proximal fragment of the radius is supinated by the supinator and the biceps brachii muscles (Fig. 9.10). The distal fragment of the radius is pronated and pulled medially by the pronator quadratus muscle. The strength of the brachioradialis and extensor carpi radialis longus and brevis shortens and angulates the forearm. In fractures of the ulna, the ulna angulates posteriorly. To restore the normal movements of pronation and supination, the normal anatomic relationship of the radius, ulna, and interosseous membrane must be regained. A fracture of one forearm bone may be associated with a dislocation of the other bone. In Monteggia’s fracture, for example, the shaft of the ulna is fractured by a force applied from behind. There is a bowing forward of the ulnar shaft and an anterior dislocation of the radial head with rupture of the anular ligament. In Galeazzi’s fracture, the proximal third of the radius is fractured and the distal end of the ulna is dislocated at the distal radioulnar joint. A B FIGURE 9.50 Fractures of the distal end of the radius. A. Colles’ fracture. B. Smith’s fracture. The Metacarpals and Phalanges There are five metacarpal bones, each of which has a base, a shaft, and a head (Figs. 9.51 and 9.52). The first metacarpal bone of the thumb is the shortest and most mobile. It does not lie in the same plane as the others but occupies a more anterior position. It is also Fractures of the olecranon process can result from a fall on the flexed elbow or from a direct blow. Depending on the location of the fracture line, the bony fragment may be displaced by the pull of the triceps muscle, which is inserted on the olecranon process (Fig. 9.10). Avulsion fractures of part of the olecranon process can be produced by the pull of the triceps muscle. Good functional return after any of these fractures depends on the accurate anatomic reduction of the fragment. Colles’ fracture is a fracture of the distal end of the radius resulting from a fall on the outstretched hand. It commonly occurs in patients older than 50 years. The force drives the distal fragment posteriorly and superiorly, and the distal articular surface is inclined posteriorly (Fig. 9.50). This posterior displacement produces a posterior bump, sometimes referred to as the “dinner-fork deformity” because the forearm and wrist resemble the shape of that eating utensil. Failure to restore the distal articular surface to its normal position will severely limit the range of flexion of the wrist joint. Smith’s fracture is a fracture of the distal end of the radius and occurs from a fall on the back of the hand. It is a reversed Colles’ fracture because the distal fragment is displaced anteriorly (Fig. 9.50). Olecranon Bursitis A small subcutaneous bursa is present over the olecranon process of the ulna, and repeated trauma often produces chronic bursitis. rotated medially through a right angle so that its extensor surface is directed laterally and not backward. The bases of the metacarpal bones articulate with the distal row of the carpal bones; the heads, which form the knuckles, articulate with the proximal phalanges (Figs. 9.51 and 9.52). The shaft of each metacarpal bone is slightly concave forward and is triangular in transverse section. Its surfaces are posterior, lateral, and medial. There are three phalanges for each of the fingers but only two for the thumb. The important muscles attached to the bones of the hand and fingers are shown in Figures 9.51 and 9.52. The Forearm Skin The sensory nerve supply to the skin of the forearm is from the anterior and posterior branches of the lateral cutaneous nerve of the forearm, a continuation of the musculocutaneous nerve, and from the anterior and posterior branches of the medial cutaneous nerve of the forearm (Fig. 9.38). A narrow strip of skin down the middle of the posterior surface of the forearm is supplied by the posterior cutaneous nerve of the forearm. The superficial veins of the forearm lie in the superficial fascia (Fig. 9.39). The cephalic vein arises from the lateral side of the dorsal venous arch on the back of the