Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
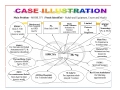
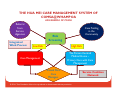
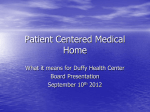
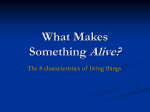
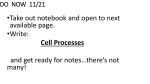
CONNECTING THE DOTS Building an Integrated Healthcare Community Essential Linkages Between Healthcare and LTC Peh Kim Choo Director, Hua Mei Centre for Successful Ageing Tsao Foundation 9/10 Dec 2014, Bangkok FOCUS: • Profile of a frail elder • The current healthcare experience • Essential linkages to building an integrated and productive care system © 2014. Tsao Foundation. Not to be reproduced or disseminated without permission. LONG TERM CARE: DEFINITION LTC refers to myriad services designed to provide assistance over prolonged periods to compensate for loss of function due to chronic illness or physical or mental disability Feder J, Komisar HL, Niefeld M.Long- Long term care in the United States: an overview. Health Affairs 2000 © 2014. Tsao Foundation. Not to be reproduced or disseminated without permission. A SAMPLE LIST OF COMMUNITY LTC SERVICES services (provided in recipients’ own homes) Personal care assistant service Personal attendant service Homemaker agency and personal care agency services Home hospice services Home delivered meals Home reconfiguration or renovation Medical services Transportation Cash payments or allowances managed by the consumer or a consumer representative to pay for above services •Services provided in congregate living settings that are expected to be the recipient’s home, such as assisted living, adult foster homes, small group homes, and residential care facilities • Cooking, housekeeping, mobility assistance, which are all services provided by personal care assistants and personal attendants or home health aides under HCBS (could be consolidated as restaurant service as well as in-home services in the resident’s unit) • Personal care (could include medication administration, medication) management • Activity program • General oversight and safety supervision • Wellness assistance and health monitoring • Palliative care •Services provided outside the recipient’s home (regardless of whether it is a private home or a group residential setting) • Adult day care • Day health care • Senior center programming •In-home • • • • • • • • • © 2014. Tsao Foundation. Not to be reproduced or disseminated without permission. WHO IS THE FRAIL ELDER? An elder who is : • likely age 75 or above • may be alone or living with family • likely to be cash strapped for services • fairly independent (though may not be safe) in ADL but likely to need help in IADL • likely to be in low mood • suffers from an average of 5.4 medical conditions including dementia and psychiatric problems • likely to have an average of 5-7 medications • family stress could be common © 2014. Tsao Foundation. Not to be reproduced or disseminated without permission. WHAT THEN ARE THE NEEDS AND ITS IMPLICATIONS Issues Multiple chronic medical conditions Implications • • • Need an overall medical/health care and education plan Need coordination and management with medical providers, essentially the health system to build stability Need different medical and allied health services such as PT, OT, speech therapy Complex medication regime, often poly pharmacy Medication noncompliance Need education and/or constant monitoring or complete medication management Compromised function leading to functional dependency • • • Need support in managing ADL and IADL Need means to access services Need build psycho-social support network Complex social circumstances and needs particularly, perhaps around financing, care and accessibility to healthcare and other necessary services • The elder’s physical and psychological adjustment to their condition The family’s adjustment to care needs of the elder The community’s adjustment to the number and needs of elders • • • • • © 2014. Tsao Foundation. Not to be reproduced or disseminated without permission. WHAT HAPPENS WHEN THESE ISSUES ARE NOT TAKEN CARE OF IN THE WAY IT NEEDS TO BE? Self • I am useless and a burden • We are not Family sure we can cope • Frequent hospitalization • Resource over-utilization Community • ‘Falling through the cracks’ © 2014. Tsao Foundation. Not to be reproduced or disseminated without permission. Accessibility Affordability © 2014. Tsao Foundation. Not to be reproduced or disseminated without permission. Quality – well being of elder and families The Issues: -Do we communicate, transit, integrate, flow seamlessly between one segment to another and amongst the segments? -Accountability – who is responsible for the care? -Do we all have the same goal? -How do we deal with the changing needs of the elder and his family across time? Hospitals Community Services © 2014. Tsao Foundation. Not to be reproduced or disseminated without permission. Home HEALTH LINKAGES 1: CARE MANAGEMENT (CARE COORDINATION) Care Coordination Ring Care Coordination Measures Atlas Advancing Excellence in Health Care • Agency for Healthcare Research and Quality Improving Primary Care Quality Indicators Updated June 2014 © 2014. Tsao Foundation. Not to be reproduced or disseminated without permission. AGENCY FOR HEALTHCARE RESEARCH AND QUALITY, USA : Defining Care Management: “the deliberate organization of patient care activities between two or more participants (including the patient) involved in a patient’s care to facilitate the appropriate delivery of health care services. Organizing care involves the marshalling of personnel and other resources needed to carry out all required patient care activities, and is often managed by the exchange of information among participants responsible for different aspects of care.” © 2014. Tsao Foundation. Not to be reproduced or disseminated without permission. CARE MANAGEMENT IS: “The fundamental focus of case management is to integrate, coordinate and advocate for individuals, families, and groups requiring extensive services.” Bower, 1992 Care Management is a process that efficiently and effectively aligns client needs/issues with resources to meet personal/family, clinical and cost outcomes. Right services…right time…right place…right cost… …right outcome (The Center for Case Management) © Tsao Foundation. No unauthorised reproduction. Main Focus of Care Management • ASSESSMENT and PLANNING • COORDINATION and BROKERAGE • MONITORING • EVALUATION AN EXAMPLE OF CARE MANAGEMENT IN ACTION Mr. Ng, 61 years, Chinese divorcee when first admitted to Hua Mei Care Management Suffers from Stroke and Ischaemic Heart Disease Lives in one room rental on his CPF saving of $5,000 for 3 years until money ran out Rely on flat mate to buy food for him until their relationship became strained Cannot walk but can bottom shuffle and barely coping Admitted to hospital for illness, after which hospital MSW advised Nursing Home Placement because he was dependent on others for his Activity of Daily Living © 2014. Tsao Foundation. Not to be reproduced or disseminated without permission. ©Tsao Foundation. No unauthorized reproduction ©Tsao Foundation. No unauthorized reproduction ©Tsao Foundation. No unauthorized reproduction ©Tsao Foundation. No unauthorized reproduction ©Tsao Foundation. No unauthorized reproduction ©Tsao Foundation. No unauthorized reproduction ©Tsao Foundation. No unauthorized reproduction ©Tsao Foundation. No unauthorized reproduction ©Tsao Foundation. No unauthorized reproduction © 2014. Tsao Foundation. Not to be reproduced or disseminated without permission. Care Coordination Ring Care Coordination Measures Atlas Advancing Excellence in Health Care • Agency for Healthcare Research and Quality Improving Primary Care Quality Indicators Updated June 2014 © 2014. Tsao Foundation. Not to be reproduced or disseminated without permission. HEALTH LINKAGES 2: THE PERSON-CENTRED MEDICAL HOME (COMPREHENSIVE PRIMARY CARE) PRIMARY HEALTH CARE “Primary care is the level of a health services system that provides entry into the system for all new needs and problems, provides person-focused (not disease-oriented) care over time, provides care for all but very uncommon or unusual conditions, and coordinates or integrates care, regardless of where the care is delivered and who provides it. It is the means by which the two main goals of a health services system, optimization and equity of health status, are approached.” -Johns Hopkins Bloomberg School of Public Health Primary care is first-contact, continuous, comprehensive, and coordinated care provided to populations undifferentiated by gender, disease, or organ system. - Starfield, B “Is Primary Care Essential?”The Lancet Volume 344(8930) 22 October 1994 pp 1129-1133 © Tsao Foundation. No unauthorised reproduction. PERSON-CENTRED MEDICAL HOME • A medical home not simply as a place but as a model of the organization of primary care that delivers the core functions of primary health care • 5 Key components of PCMH • • • • • Patient-centered Comprehensive care Coordinated care Superb access to care A systems-based approach to quality and safety – Agency for Healthcare Research and Quality: PCMH Resource Center http://pcmh.ahrq.gov/portal/server.pt/community/pcmh__h ome/1483/what_is_pcmh_ © Tsao Foundation. No unauthorised reproduction. PRIMARY CARE IS: ‘One approach to decreasing fragmentation, improving coordination, and placing greater emphasis on the needs of patients is the patient-centered medical home (PCMH). Its components include patient-centered care with an orientation toward the whole person, comprehensive care, care coordinated across all the elements of the health system, superb access to care, and a systems-based approach to quality and safety.1 Ultimately, these components are intended to improve patient outcomes—including better patient experience with care, improved quality of care (leading to better health), and reduced costs.2 ‘ 1http://www.pcmh.ahrq.gov/portal/server.pt/community/pcmh__home/1483/what_is_pcm h_ for AHRQ’s definition of the PCMH. 2 See Berwick et al. (2008) for a discussion of this “triple aim” of better patient experience, improved population health, and reduced per capita costs. © Tsao Foundation. No unauthorised reproduction. THE PCMH CARE: Dan Duffy, M.D., School of Community Medicine, Tulsa, OK © Tsao Foundation. No unauthorised reproduction. THE HUA MEI CARE MANAGEMENT SYSTEM OF COMSA@WHAMPOA AN EXAMPLE OF PCMH Referral from Service Agencies Integrated Work Process Case Finding in the Community Risk Screening Low Risk High Risk The Person Centred Medical Home – Primary Care with Care Management Care Management Trained ParaCare Managers © 2014. Tsao Foundation. Not to be reproduced or disseminated without permission. Service Coalition Network ISSUES TO CONSIDER FOR IMPLEMENTATION: • Financing Framework • Training and Development of Manpower • Communication Platform • Siting within the Health Care System © 2014. Tsao Foundation. Not to be reproduced or disseminated without permission. THANK YOU