Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
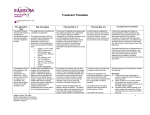
BRAIN TUMOUR OUTCOME MEASURES Amr Mohamed FRCS (Surg Neuro) Surgical Neuro-oncology Fellow North Bristol Trust Introduction ■ In 2011 in the UK, 9400 new patients were diagnosed to have brain tumour, that is 26/day. ■ 76% were under 75 years old. ■ The 4th group of cancers in the teenagers and young adults. ■ 34% astrocytomas and 21% meningiomas. 8 in 10 of the astrocytomas are GBM. ■ Estimates suggest that secondary brain, other CNS and intracranial cancers occur in at least 6% of all cancer patients, but this varies by the site of the primary cancer. “Cancer Research UK, http://www.cancerresearchuk.org/health-professional/cancerstatistics/statistics-by-cancer-type/brain-tumours#heading-Zero, Accessed November, 2015” Introduction ■ Around a fifth (19%) of people diagnosed with brain cancer in England and Wales survive their disease for five years or more (2010-11). ■ 4 in 10 (40%) people diagnosed with brain cancer in England and Wales survive their disease for one year or more (2010-11). ■ Brain cancer survival is highest for people diagnosed aged under 40 years old. ■ 6 in 10 people diagnosed aged 15-39 survive their disease for five years or more, compared with less than 1 in 100 people diagnosed aged 80 and over. ■ Brain cancer survival is improving and has doubled in the last 40 years in the UK. ■ In the 1970s, around 5 in 100 people diagnosed with brain cancer survived their disease beyond ten years, now it's around 3 in 20. “Cancer Research UK,http://www.cancerresearchuk.org/healthprofessional/cancerstatistics/statistics-by-cancer-type/brain-tumours#heading-Two, Accessed November, 2015” High Grade Glioma Specialist Nurse Pathway Seamless communication throughout the patients pathway with local & regional neuro-oncology treatment centres TYA SERVICE 16-24 YRS Emergency Surgery Clinic Appointment Surgeon / Oncologist or CNS Emergenc y NBT or Other Hospital Treatment / Surveillance Phase Treatment Decision Phase Diagnosis Phase MDT and PATH MDT GP referrals Palliative Care Management Oncology Treatment Radiotherapy Chemotherapy/ Clinical Trials Diagnostic Meeting Surgeon / CNS Elective Surgery Biopsy or Excision Palliative Care Management Follow up Phase Surveillance MRI Scan 3 monthly Post radiotherapy and Chemotherapy Further 2nd Line Chemotherapy Radiological Progression / MDT REVIEW Further Surgery Palliative Care Management Telephone Clinic Follow-up / Support Living Well Event Health Needs Assessment(s) Telephone Support Professional Follow up • • • • Patients awaiting surgery . Patients will have remote monitoring with surveillance scanning dictated by consultants / MDT opinion. Patients will be booked to Clinic to review with MRI results. Patients will be seen by Consultants after their surgery, with the CNS to discuss histology results and treatment plans. • • • Monitoring of patient s with active neurological problems – liaising with GP and other Community Support Teams. To discuss MRI results and MDT Outcomes with the patient over the phone. Symptom control alongside the Consultant Oncologist/ Consultant Neurosurgeon. Surveillance Monitoring • • • On Treatment Review Patients will be actively monitored and seen in clinic by a Consultant Oncologist with MRI at 3 monthly intervals. Advice and consultation for patients with residual symptoms and side effects from Oncological treatments. Designed by; B. Coghlan & L. Baldry & S. Bautista-Pike Neuro – Oncology CNS’s . January 2015. Palliative Care Management If Neuro-Surgery or Oncological treatments (i.e. Radiotherapy or Chemotherapy) are not feasible (whether in hospital or at home) referral to a local palliative care team at any stage of the pathway , is essential for management of symptoms and co-ordination of care. Low Grade Glioma Specialist Nursing Pathway Seamless communication throughout the patients pathway with local & regional neuro-oncology treatment centres Emergency Surgery Emergency Clinic Appointment Surgeon / CNS NBT / Other Hospital Treatment / Surveillance Phase Treatment Decision Phase Diagnosis Phase TYA Service for 16-24 Yrs MDT and PATH Oncology Diagnostic Meeting Palliative Management Professional follow up • • Surveillance MRI Scan 3/6/12 months MDT REVIEW CNS Telephone follow up Patients awaiting surgery . Patients will have remote monitoring with surveillance scanning dictated by consultants / MDT opinion. Patients will be booked to Clinic to review with MRI results. Patients will be seen by consultants after their surgery with the CNS to discuss histology and treatment plans Radiological/ Surgical Changes:transfer to High Grade Pathway • • Monitoring of patient s with active neurological problems – liaising with GP and other Community support To discuss MRI results and MDT Outcomes. with the patient over the phone. Symptom control alongside the consultant oncologist/ consultant neurosurgeon. Remote Monitoring/ discharge to GP Living Well Event Health Needs Assessment(s) Surveillance Monitoring Telephone follow up / Support • Professiona l Follow up Neurosurgery Not for surgery • • Living Well Event For Biopsy or Excision MDT GP referrals Follow up Phase • • • Patients will be actively monitored & seen in clinic by either the Neurosurgeon or Oncologist with MRI initially at 3 months , then 6 monthly for a year, then 1 yearly . Advice & consultation for patients with residual symptoms Patients transfer to High Grade Pathway on radiological /Surgical transformation of their tumour. Designed by B. Coghlan & L. Baldry & S. Bautista–Pike : Neuro-Oncology CNS’s. January 2015 Discharge to GP • Asymptomatic patients with stable disease after 10 years of surveillance will be discharged to their GP. How? ■ Different outcome measures: – – – – – – – – Karnofsky Performance Status Scale (KPS) WHO performance scale Modified Rankin scale (MRS) The FIM instrument (functional independence measure score) Disability Rating Scale (DRS) Barthel index Functional Assessment of Cancer Therapy-Brain (FACT-BR) The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Brain Cancer Module (EORTC QLQ-BN20) ■ The FIM, KPS, and DRS did not show significant correlation with the FACT-BR. ■ Conclusion: – Although patients make functional gains during and after inpatient rehabilitation, gains in QOL are not significant until 1 month post-discharge. – QOL does not appear to correlate well with functional outcomes. – Further, the KPS is less sensitive than the FIM and DRS in detecting change in functional status. Arch Phys Med Rehabil Vol 82, November 2001 Which one? What? ■ Quality of life (QOL) is a concept that encompasses the multidimensional well-being of a person and reflects an individual's overall satisfaction with life. ■ QOL is a broad term that involves several dimensions, including physical or functional status, emotional well-being, and social well-being. “Cella D, Chang CH, Lai JS, Webster K. Advances in quality of life measurements in oncology patients. Semin Oncol. 2002;29: 60-68” Why? ■ Measurement of Health Related Quality of Life (HRQL) in brain tumour patients is important because: – Brain tumours and brain tumour treatment usually affect physical, cognitive as well as emotional functioning. – Understanding of disease burden and for the impact of specific tumour treatment. “Heimans, Taphoorn. Impact of brain tumour treatment on quality of life. J Neurol 2002; 249(8):955-60” Physical well-being QOL Emotional well-being Social well-being Why? ■ Patients with primary brain tumors face serious challenges to their QOL. They have difficulties with general symptoms such as headache, anorexia, nausea, seizures, and insomnia. ■ These patients also face symptoms secondary to focal neurologic deterioration, including motor deficits, personality changes, cognitive deficits, aphasia, or visual field defects. ■ The overall symptom burden and disability for glioma patients are significant, especially in those with high-grade or recurrent disease “Heimans JJ, Taphoorn MJ. Impact of brain tumour treatment on quality of life. J Neurol. 2002;249: 955-960” “Osoba D, Brada M, Prados MD, Yung WK. Effect of disease burden on health-related quality of life in patients with malignant gliomas. Neuro-Oncology. 2000;2: 221-228” Treatment Factors Tumour Factors •Surgery •Biopsies do worse •RT •Affect cognition •Fatigue •CT •Medications •Location •size •Type •Psychology •Cognitive •Epilepsy Raymond Liu et al. Neuro Oncol 2009;11:330-339 Patient Factors •Studies focusing on brain tumor patient comorbidities and demographics and their effects on QOL are largely lacking QOL When? Preoperative Baseline ? Before RT / CT 1 month post-RT/CT With each surveillance scan Who is it for? ■ High grade tumours? ■ Other intracranial tumours? ■ – – – – – – – – – Low grade tumours? Young Longer survivors Complex symptoms setup Epilepsy Cognitive Frequent appointments Driving Dedifferentiation Often Unable to tap into hospiceservices often (even though they are for patients with a life limiting illness diagnosis) How? ■ Neuro-oncology MDT clinic (Baseline) ■ By a phone interview ■ Electronic on the BNOG / Somerset cancer register websites, etc ■ Electronic in the clinic on a tablet (prepare for a paperless hospital) ■ Conclusions “The QLQ-BN20 and the FACT-Br are both valid and reliable tools that have been used extensively in the primary brain cancer population. Choice between the two tools should consider each instrument’s individual strengths and weaknesses.” Why? • Approximately 55 different generic and targeted questionnaires and symptom indices • Range of questionnaires allow for greater disease, treatment or condition specificity • Easy to complete (most in 5-10 minutes) • Easy to administer as a computer-based/internet application • Demonstrated reliability, validity and sensitivity to change • Some questionnaires translated and pre-tested in over 50 languages • Special consideration for spiritual well-being, palliative care, and treatment satisfaction • More social well-being coverage • Written at the 4th Grade reading level (9-10 years old) Why? • Demonstrated equivalence in mode of administration (interview vs. self- administration) • Validated for use with special populations such as with the elderly and those living in rural areas • Appropriate for use in patients with a variety of chronic health conditions, and in the general population • Multiple scoring options: subscale scores, total score, and a Trial Outcome Index (TOI) • MID information available for several scales • Normative data available for various cancer and general population samples • Used by major cooperative clinical trial groups, international-industry sponsored research, other government/military funded research, and health practice self studies How ? ■ Free ■ www.facit.org Conclusion ■ The need to have an outcome measure ■ Economic impact ■ Audits, trials, research ■ Seamless, easy, validated tool ■ Integrated into software/websites