Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
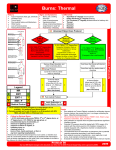
Burns and Thermal Injuries K. John Hartman MD FACS ACS-IA Chapter COT Vice Chair Trauma Medical Director Co-Director Surgical ICU Genesis Davenport 10JAN16 Provides several essential functions that are lost with burn injury. Functions include immunologic defense, fluid conservation, and temperature regulation. Important elements of skin include melanocytes and glands. Sweat-producing exocrine glands may become hypersecretory in healed areas after thermal injury. Injuries to tissues caused by contact with ◦ ◦ ◦ ◦ ◦ ◦ ◦ Dry heat Moist heat Electricity Chemicals Friction Radiant and electromagnetic energy. Thermal injuries are those burns caused by flame, hot objects, or hot liquids. Hypothermia and frostbite are other forms of thermal injury. Burns damage or destroy skin cells and may involve the subcutaneous tissues including, fat, muscle, and bone. The depth of injury is determined by the cause of the burn, chemical vs. electric vs. thermal, the temperature or energy to which the skin was exposed, and the duration of exposure. Depth combined with the extent of the burn, based on total body surface area (TBSA) burned and the patient's body weight, determine the severity of the injury More than 1.2 million people are burned in the United States every year Up to 75% are treated as out patients. From 2006 to 2012, 175,099 patient were admitted to Burn Centers Only motor vehicle collisions cause more trauma-related deaths Burn deaths occur after the injury or weeks later as a result of multisystem organ failure Seventy-two percent of all burns occur at home. Sixty-nine percent of burn patients are men. The mean age is 32 years old. Children under 5 years old account for 20% or cases. Adults over 60 years old account for 12% of cases. Seventy-five percent of all burn-related deaths occur in house fires. Other risk factors include low socioeconomic class and unsafe environments. Nonflammable children’s sleepwear. National Electrical Code decreasing oral commissure burns. Elevation of hot water heaters from the ground. Increased smoke alarm use. Mortality rate has improved for patients sustaining severe injuries. In 1949, in the United Kingdom first reported a 50% mortality rate for children 14 years old and younger with burns of 49% TBSA ◦ 50% mortality was reached for those 15 to 44 years old with burns of 46% TBSA, ◦ 45 to 64 years with burns of 27% TBSA, and those 65 years and older with burns of 10% TBSA. Latest studies reporting a 50% mortality rate for 98% TBSA burns in children 14 years old and younger, and 75% TBSA burns in other young age groups.[9] Flame—damage from superheated, oxidized air Scald—damage from contact with hot liquids Contact—damage from contact with hot or cold solid materials Chemicals—contact with noxious chemicals Electricity—conduction of electrical current through tissues First degree—injury localized to the epidermis Superficial second degree—injury to the epidermis and superficial dermis Deep second degree—injury through the epidermis and deep into the dermis Third degree—full-thickness injury through the epidermis and dermis into the subcutaneous fat Fourth degree—injury through the skin and subcutaneous fat into underlying muscle or bone Destroys only superficial layers of skin (epidermis). Physiologic functions of the skin remain intact. Manifestations include local pain, blistering, and erythema. The injury heals in 3 to 5 days without scarring. For large burns, hydration and symptom relief with non-narcotic analgesics may be recommended. Second-degree burns include two subtypes: superficial and deep partial thickness Superficial partial-thickness burns involve the epidermis and dermis. Pain and blistering occur. Heals in 21 to 28 days, and scarring may occur, depending on genetic tendency. Hair follicles remain intact. Deep partial-thickness burns involve the entire dermis. The injury is mottled, has dry blisters, and is relatively painless. Healing occurs in about 30 days spontaneously. Third-degree full-thickness burns involve the epidermis, dermis, and underlying subcutaneous tissue. Skin is charred and may appear black, white, or cherry-red. The wound is painless to touch. Skin grafting is indicated for wounds greater than 2 inches in diameter The wound is painless to touch. Fourth-degree full-thickness burns are rare. When they do occur, they are often fatal. The injury extends beyond the dermis and involves muscle, bone, or both. Safe distance STOP the burning The initial evaluation of the burned patient is the same as any trauma patients and follows the ABC of airway, breathing, and, circulation. As part of the initial resuscitation, vascular access is obtained through unburned tissue if possible, if not place the iv through burned tissue. Remove all clothing and jewelry to stop the burning process and prevent injury from edema. Inhalation injury ◦ One third of all major burns ◦ Mortality is more than double that of cutaneous burns. ◦ Isolated inhalation injuries do not result in high mortality. ◦ Combination of inhalation injury and cutaneous thermal injury creates a double insult. Suspect Inhalation injury if: ◦ ◦ ◦ ◦ ◦ ◦ ◦ Face or Neck burns Singeing of facial hair Carbonaceous sputum Oralpharynx erythema Hoarseness Closed space blast or fire Carboxyhemoglobin greater than 10%. Upper airway rather than in the lower airway because the oropharyngeal cavity has a substantial capacity to absorb heat Constitutes an important indication for intubation Mandatory to control the airway before airway edema develops during resuscitation Diagnosis is achieved with direct laryngoscopic visualization of the oropharyngeal cavity Upper airway thermal burns usually manifest within 48 hours after injury, Airway swelling can be expected to peak at 12 to 24 hours after injury. True upper airway burn will likely require airway protection for 72 hours Injury to the tracheobronchial tree and the lung parenchyma results from combustion products in smoke and, under unique conditions, inhaled steam Irritants in smoke can cause direct mucosal injury, leading to mucosal slough and bronchial edema, bronchoconstriction, and bronchial obstruction. May progress to pulmonary edema, pneumonia, and acute respiratory distress syndrome (ARDS) Can be confirmed by bronchoscopy or xenon-133 ventilation-perfusion scan Inhalation injury is identified and treated as necessary with intubation and or bronchoscopy. Other traumatic injuries are identified and treated appropriately In burns greater than 20% TBSA, a nasogastric tube is place to decompress the stomach and eventually begin early enteric feedings. Fluid resuscitation follows based on one of several formulas that calculate the fluid needed for the first 24 hours based on the TBSA burned and the patient's body weight. After the acute management, pain management, wound management, nutrition, and rehabilitation are addressed. 1. Partial thickness burns greater than 10% TBSA 2. Burns involving the face, hands, feet, genitalia, perineum, or major joints 3. Any full-thickness burn 4. Electrical burns, including lightning injury 5. Chemical burns 6. Inhalation injury 1. Burns in patients with preexisting medical disorders that could complicate management, prolong recovery, or affect outcome 2. Any patient with burns and concomitant trauma (such as fractures) in which the burn injury poses the greater immediate risk of morbidity and mortality. 3. Burned children in hospitals without qualified personnel or equipment to care for children 4. Burns in patients who will require special social, emotional, or long-term rehabilitative intervention. History: 36 y/o female with 57%TBSA, mostly third degree thermal burns of face, neck, both hands, forearms, arms, shoulders; both legs and thighs, buttocks and anterior abdominal wall. TOI ~1015L 4 Oct. MOI - Patient a Social Scientist embedded in 2/2. Unit attacked and petrol poured over patient and set alight. Extinguished in stream contaminated with sewage. Evidence of upper airway burn on intubation. No radiological evidence yet of true inhalation injury. Rewarming and fluid resuscitation ongoing using Parkland formula. Intubated and ventilated. Right subclavian central venous access and left long saphenous peripheral venous access. Admitted to ITU. Surgery: 1200L 4 Oct. Debridement and dressing of burns. Bilateral escharotomies of digits, hands, and forearms. Recommend URGENT aeromedevac to closest burn facility able to handle this level of injury. Specific Blood Pressure not obtainable currently due to nature of injuries but is deemed stable per physician on duty. Good urine output. Arterial cannulation will be attempted following rewarming. Blood gases are venous sample. Burn shock is a life-threatening process that occurs in the acute phase after major burn injury. Massive fluid leak from capillaries results in intravascular hypovolemia, extensive edema, hemoconcentration, and reduced urine output. Capillary leak resolves about 24 hours after injury. Fluid replacement is the primary treatment objective during burn shock. TABLE 22-2 -- Resuscitation Formulas Formula Crystalloid Volume Colloid Volume Free Water Parkland 4 mL/kg per % TBSA burn None None Brooke 1.5 mL/kg per % TBSA burn 0.5 mL/kg per % TBSA burn 2.0 L Galveston (pediatric) 5000 mL/m2 burned +1500 mL/m2 total None None These are used as guidelines for the initial fluid management after burn. The response to fluid resuscitation should be continuously monitored, and adjustments in the rate of fluid administration should be made accordingly. TBSA, total body surface area. The emergent phase is the time between the end of burn shock and closure of the wound to less than 20% TBSA. Wound management, nutritional support, and surgical grafting of full-thickness wounds are the priorities of treatment during the emergent phase. Cardiovascular: Low cardiac output may occur in response to unknown myocardial depressant factors. Respiratory: Inhalation injury can cause airway obstruction, carbon monoxide poisoning, and hypoxia. Acute respiratory distress syndrome is a serious complication of burn injury characterized by refractory hypoxemia. Metabolic: Release of catecholamines in response to burn stress is associated with an increased heart rate, increased oxygen consumption, and increased serum glucose. A hypermetabolic state is maintained by hypothalamic thermoregulation. Gastrointestinal: Adynamic ileus lasts for about 3 days after burn injury. The liver may increase production of clotting factors. Immune: Inflammation is initiated by burned tissue and results in the release of cytokines that mediate increased capillary permeability and vasodilatation. In general, immune system depression is predominant with decreased leukocyte migration and poor opsonization. Cellular: Dysfunction of energy-requiring cellular processes, such as pumping of ions, results in widespread cellular swelling and altered membrane potentials. Electrical shock is associated with injury deep within the body, particularly injury involving low-resistance tissue such as blood vessels and nerves. Cardiac arrest, coagulation of blood within the vessels, and renal damage secondary to myoglobinuria are serious consequences of electrical injury. Severe short-term memory loss, ataxia, and sensory deficits may occur as a result of neuronal damage. Carbon monoxide (CO) poisoning, Upper airway thermal burns, Inhalation of products of combustion. Most common cause of death in inhalation injury Carbon monoxide has a 200 times greater affinity to hemoglobin than oxygen Oxygen–hemoglobin dissociation curve loses its sigmoidal shape and shifts to the left Levels of CO greater than 60% are usually fatal 80 minutes for a person breathing room air to reduce the CO level of 60% to a safer level of 20%. The addition of 100% oxygen can reduce that time to 20 minutes Wound management is necessary to prevent bacterial colonization of the wound and subsequent septicemia. Early surgical wound management is essential. Topical antibiotics are used because systemic antibiotics cannot reach the wound because of a lack of blood supply. Early surgical excision and skin grafting are the treatment of choice for deep burns. Excision procedures result in significant blood loss requiring blood transfusions. Skin grafts are taken from a healthy portion of the patient's own skin. Temporary grafts (e.g., cadaver skin, synthetics, pig skin) may be used to cover the wound until an autograft can be completed. Silver Sulfadiazine Mafenide Bacitracin Neomycin Polymixin Mupirocin 0.5% Silver nitrate 5% Mafenide acetate 0.025% Sodium hypochlorite 0.25% Acetic acid OpSite Biobrane Trancyte Integra Xenograft (pig skin) Allograft (homograft, cadaver skin) The rehabilitation phase begins when the burn is reduced to less than 20% TBSA. Problems during this phase include skin contracture and excessive scarring. Healing is complete at 6 months to 1 year. Positioning in extension and range-ofmotion exercises are important to prevent contracture Mildest form of cold injury. Pain, Pallor, Numbness or effected area. Reversible with warming. Does NOT result in tissue loss. Injury due to freezing of tissue. Intracellular ice crystal formation. Get reperfusion injury with warming of the tissue. Leads to tissue loss. Degree of injury same as for burns Trench foot, long term exposure to wet conditions with temperature just above freezing Put on dry socks Drink warm fluids Rewarm body part in 40Degree C (104 degree F) water until pink color and perfusion return. Avoid dry heat Save as much tissue as possible. Do NOT open blisters. Prevent infection. Elevate the extremity. Leave open to the air. Avoid pressure spots. Wait several weeks prior to debridement to determine viability of tissues.