Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
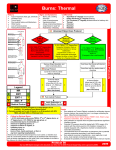
Initial Burn Care Lee D. Faucher, MD FACS Director UW Burn Center Associate Professor of Surgery & Pediatrics Objectives • Discuss burn pathophysiology • Outline treatment modalities • Understand why some treatments better than others What is a burn? • Cutaneous injury caused by heat, electricity, chemicals, friction, or radiation. First Degree Burns • • • • • Epidermis only No blisters Erythema Mild to absent systemic response Heals in 3-4 days Superficial partial thickness • • • • • • • Papillary dermis Blisters Homogenous pink Painful, hypersensitive Blanches Hair usually intact Does not scar, may pigment differently Sup 2nd degree Deep partial thickness • • • • • • • Reticular dermis Mottled red and white Not painful to pinprick or pressure Does not blanch Heals > 3 weeks Usually scars Need to excise and graft Deep dermal Full thickness burns • • • • • • • Into fat or deeper Red, white, brown, black, etc. Diminished sensation Dry, may be leathery Depressed Heals only from the periphery Always excise and graft Full-thickness Etiology Types of burns Where do burns occur Circumstances of injury Admissions by age % of admissions vs. burn size Inhalation injury diagnosis • Closed-space fire • Face burns Terminology • Inhalation injury “nonspecific” – Thermal injury • Upper airway – Local chemical irritation • Throughout airway – Systemic toxicity • CO Clinical diagnosis • History and physical – Exposure – Duration – Enclosed space • Diagnostic studies Other signs and symptoms • • • • • • • Lacrimation Cough Hoarseness Dyspnea Disorientation Anxiety Wheezing • Conjunctivitis • Carbonaceous sputum • Singed hairs • Stridor • Bronchorrhea Poison management = CO • 500 unintentional deaths each year • Persistent Neurologic Sequelae – May improve over time • Delayed Neurologic Sequelae – Relapse later Poison management = CO • Treatment – CO level means nothing to predict outcome – Length of hypoxia is the determining factor – Oxygen – HBO • No studies show benefit in treatment Pathophysiology • The main factor responsible for mortality in thermally injured patients • Carbon monoxide the most common toxin – 200 times greater affinity – Competitive inhibition with cytochrome P450 Reduction of CO 80 Room Air 100% Oxygen 3 ATM % CO 60 40 20 0 0 20 40 Time in Minutes 60 80 Objective data • Bronchoscopy – Edema – Infraglottic soot – Hyperemia – Mucosal sloughing • Sensitivity near 100% under IDEAL circumstances Grading of injury • No reliable indicators of progressive respiratory failures • No studies have found any correlation with initial findings and clinical outcomes and progress Resuscitation Field resuscitation • Start IV with LR, in burn OK – < 6 years = 125mL/hr – 6-13 years = 250mL/hr – >13 years = 500mL/hr Rule of Nines Lund and Browder Chart Area 0-1 yr. Head 19 Neck 2 Ant. Thorax 13 Post. Thorax 13 R. Buttock 2½ L. Buttock 2½ Genitalia 1 R. U. Arm 4 L. U. Arm 4 R. L. Arm 3 L. L. Arm 3 R. Hand 2½ L. Hand 2½ R. Thigh 5½ L. Thigh 5½ R. Leg 5 L. Leg 5 R. Foot 3½ L. Foot 3½ 1-4 yr. 17 2 13 13 2½ 2½ 1 4 4 3 3 2½ 2½ 6½ 6½ 5 5 3½ 3½ 5-9 10-14 yr. yr. 13 11 2 2 13 13 13 13 2½ 2½ 2½ 2½ 1 1 4 4 4 4 3 3 3 3 2½ 2½ 2½ 2½ 8 8½ 8 8½ 5½ 6 5½ 6 3½ 3½ 3½ 3½ 15 Adult 2 3 Total yr. 9 7 2 2 13 13 13 13 2½ 2½ 2½ 2½ 1 1 4 4 4 4 3 3 3 3 2½ 2½ 2½ 2½ 9 9½ 9 9½ 6½ 7 6½ 7 3½ 3½ 3½ 3½ Total IV access • • • • • < 15% TBSA – oral resuscitation 15 – 40% TBSA – one large bore IV > 40% -- two large bore IV’s IV’s should be in the upper extremities Suture IV’s started through burns Crystalloid solution • Ringer’s Lactate – [Na+] 130 mEq (serum 140 mEq) – Osmolality 272 mOsm (serum 300mOsm) • Advantages of crystalloid – Effective in maintaining perfusion – Costs less than colloids – Can be mobilized with a diuretic Resuscitation first 24 hours • Baxter formula – 4 mL/kg/% TBSA burned • Give ½ the volume in first 8 hours and other ½ over next 16 hours. If < 20kg • Same Baxter formula for LR • Add 4mL/kg of D5 ¼ NS – Infuse at constant rate, increase LR if needed for adequate urine output Monitor urine output • Place foley if > 20% TBSA • Urine output goal – 2 mL/kg/hr very young – 1 mL/kg/hr child – 0.5 mL/kg/hr adult • Diuretics are NEVER used to increase urine output • Increase urine output to > 100mL/hr if pigment present How to do this • Maintain continuous IV fluid replacements • AVOID boluses • Only bolus IV fluids if hypotensive Zones of burn injury Pain control Non-medication methods • Cover burns with plastic wrap – Wet dressings will stick and cause more pain – Other burn dressings are expensive and not necessary – Quik Clot is expensive and will not provide any patient benefit Ice Pack-----DO NOT USE EVER • DOES NOT – Reverse temperature – Inhibit destruction – Prevent edema • DOES – Delay edema – Reduce pain Medication • Medications – Opioids – Narcotics – Pain medications – IV Analgesia Summary • Airway • Circulation/Resuscitation • Pain control Questions?