Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Interactions Between Coagulation and Complement on Biomaterial Surfaces
THE HOST’S RESPONSE
•
Protein deposition on membrane
• Boundary layer/secondary layer
•
Cellular Activation
• Platelet/leukocyte aggregates
•
Immune stimulation
• Complement
•
Hypersensitivity reactions
• Residual ETO
•
Hemodynamic Effects
•
Contact phase formation of bradykinin
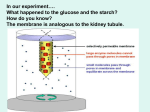
PROTEIN DEPOSITION
•
Deposition of protein occurs instantaneously
• A protein layer forms on the surface of the membrane as the levels of solution
phase proteins increase
•
Composition of adsorbed proteins depends upon membrane type
• Hydrophobic membranes tend to adsorb more proteins
•
Proteins adsorb and then detach until permanent adsorption and denaturing occurs
• This may result in the formation of a boundary layer
•
Protein adsorption determines cellular responses
•
Protein adsorption may serve as a way to successfully remove unwanted proteins
from patients or may negatively effect the diffusivity of the membrane
• Low MW-interleukins, inflammatory cytokines
• High MW-albumin, fibrinogen, IgG
PLATELET/LEUKOCYTE AGGREGATES
•
Platelets aggregate on membrane
surface resulting in further aggregation of
leukocytes
•
Aggregation causes activation of the
platelets as well as the leukocytes and
can result in release of platelet-derived
factors and cytokines
•
Results: superoxide release, cytokine
release and leukopenia
•
Superoxide release resulting from
chronic dialysis has been implicated
in atherosclerosis
•
Cytokine release and leukopenia
can result in general feeling of
malaise
UPenn
DIALYSIS
KIDNEY FUNCTION
•
The natural kidneys are bilateral fist-sized
organs located below the rib cage
•
Their functions include:
•
Excretion of detoxified compounds
•
Regulation of composition of body
fluids with respect to specific solutes;
e.g. Na+, K+, Ca2+
•
Regulation of acid-base balance
•
Regulation of body fluid volumes
•
Nonexcretory functions; e.g. secretion
of renin
In a 24 hour period the kidneys Clear ~ 15-20 grams of urea
and a similar quantity of other nitrogenous waste products of protein
and produce approx. 1.5-2 L of fluid
Kidneys Work Hard!
DETERMINING KIDNEY FUNCTION
The clinical manifestation of kidney disease is usually elevated circulating levels of
urea and creatinine in plasma. But not always…. since a malnourished patient with
poor renal function may have normal levels of urea and creatinine
For more detailed diagnosis, kidney function is reported in terms of clearance. For
any solute, clearance is defined as:
Clearance = Quantity Produced in Urine *
Blood Concentration
*over a known time interval
Clearance of urea or creatinine are easily measured.
A young, healthy adult has over-capacity of kidney function, usually about ten times
what is necessary. After age 30, renal function declines about 10% for each
remaining decade of life
Glomerular Filtration Rate is another indicator of renal function that
can be correlated with clearance
The GFR in humans remains quite constant at a value of about 125 ml/min
(normalized to a body surface area of 1.73 m2). This is remarkably high
(180 liters of plasma filtered per day, which is 60 times plasma volume,
15 times total ECF volume, and 5 times total body water)
Inulin, a starch-like polymer of fructose (5,000
daltons), is the substance of choice to measure GFR.
GFR = CIn = UIn V / Pin
Another substance used to measure GFR and is
of clinical importance is creatinine
Creatinine clearance gives a high estimate of GFR in
humans since it is secreted to a small extent.
KIDNEY DISEASE AND FAILURE
ACUTE AND CHRONIC
•
Pre-renal causes are due to
decreased blood supply to the
kidney.
•
Direct kidney damage
• Trauma
• Hypovolemia (low blood
volume) due to blood loss
• Autoimmune diseases
• Dehydration from loss of body
fluid (vomiting, sweating, fever )
• High blood pressure
• Diabetes
• Poor intake of fluids
• Infection
• Medication, for example,
diuretics ("water pills") may
cause excessive water loss.
• Medications
• Loss of blood supply to the
kidney due to obstruction of the
renal artery or vein
• Rhabomyolysis
• Sepsis
• Pain medications
• Statins???
Damage to the kidneys can result in either acute renal failure or chronic renal failure
ACUTE RENAL FAILURE
Acute renal failure may be treated with either medication alone or with a
combination of medication and dialysis and usually is reversible
Approximately 1% of patients admitted to hospitals have ARF at the time of admission,
and the estimated incidence rate of ARF is 2-5% during hospitalization.
Approximately 95% of consultations with nephrologists are related to AKI.
The mortality rate estimates vary from 25-90%.
The in-hospital mortality rate is 40-50%; in intensive care settings,
the rate is 70-80%.
KIDNEY FAILURE
Kidney failure, as opposed to kidney disease, occurs when the kidneys can no
longer support life. Patients first become symptomatic when clearance falls to about
10% of normal levels. (Urine production is usually maintained in early-stage kidney
disease; most often, the composition, rather than the quantity, of the urine is
abnormal). Patients become severely ill at 5% of capacity. Absent therapeutic
intervention, life can sustain itself only for 2-4 weeks after kidney function ceases or
falls much below about 5% of normal.
Patients with end stage kidney disease have three treatment options:
•
Hemodialysis
•
Peritoneal Dialysis
•
Transplantation
What functions are compensated for by dialysis
and how are other kidney functions regulated?
DEMAND FOR RENAL REPAIR AND
REPLACEMENT
Why use biomaterial-based devices?
Many times tissues and even organs can repair on their own
When this is not possible, the best alternative is a transplant
of native tissue.
There are two significant problems with this, however.
Lack of acceptable donors
Potential host rejection of the transplant along with
chronic immunosuppression therapy
THERAPY CHOICES
•The choice between hemodialysis and
peritoneal dialysis is up to the patient.
•In the United States, < 10% of all patients
elect peritoneal dialysis, but the number is
much larger in many other countries.
• No convincing and clearcut difference in
either morbidity or mortality has been
demonstrated between the two options.
•In practice, most patients rely upon their
doctor’s recommendations.
•Opinions differ on what informs the
physician’s perspective.
Harvard.edu
Dialysis versus Peritoneal Dialysis
Merck, Inc
VASCULAR ACCESS
• Difficulty with establishing
vascular access inhibited
the use of dialyzers for
treatment of chronic
kidney failure
• The Quinton-Scribner shunt
(1960)
• Creation of arterio-venous
fistula (1966) by Brescia et
al.
Since patients are usually treated 3X/week, access to the vasculature
is critical.
There are a few ways to maintain continual access
A surgeon creates an AV fistula by connecting an artery
directly to a vein, frequently in the forearm.
Connecting the artery to the vein causes
more blood to flow into the vein.
As a result, the vein grows larger and stronger,
making repeated needle insertions for
hemodialysis treatments easier
The formation of an adequate fistula make take up to 1 year.
This type of vascular access is successful
Another option is implantation of an artificial vascular graft
This type of access may be more appropriate for patients who have
small vessels and do not form adequate fistulas
Access
Access
Access
Access
Once vascular access has been established, the patient
is connected to the dialyzer set up
EARLY DIALYZERS MOVE FROM VERY LARGE UNITS TO
FAIRLY SMALL HOLLOW FIBER UNITS
Capillary Artificial Kidneys
(Hollow Fiber Dialyzers): 1964-1967
Cordis Dow Seratron
Dialysis Machine: 1979
The early dialyzer designs included coil dialyzers. These coil designs were
composed of 1-2 long membrane tubes coiled around a plastic core. Major
issues were the limited surface area and non-uniform flow of dialysate
Parallel plate dialyzers are
composed of sheets of membranes
mounted on support screens and
stacked. There are multiple
parallel channels of
flow along the membranes.
This increases performance
and provides thinner channels
of dialysate and blood.
These have been used relatively
successfully although
the size of the device has
been a limiting factor
SINGLE PATIENT UNITS WITH PRE-STERILIZED HOLLOW
FIBER DIALYZERS
HOLLOW FIBER CAPILLARY DIALZERS
• Most effective
• Low volume/high efficiency
• Low resistance to flow
• Blood flows through lumens of
fibers and dialysate flows
around the outside of the fibers
• Low priming volumes required
• Easier reuse
Components of this set up can be broken down into the fluid cycler,
dialyzer membrane and cartridge and the dialysate fluid
http://www.youtube.com/watch?v=-ZX7bsI2F9U
http://www.youtube.com/watch?v=Rfvegx6tzQ0
Fluid Cycler
Dialyzer
Hollow fiber-low volume, high efficiency, low resistance
to flow
Blood flow rate=200-350 ml/min
Dialysate flow rate=500ml/min
Most mass transport occurs by
diffusion
Pressure 100-500 mmHg higher
on blood side
2-4 L fluid removal
n engl j med 357;13
www.nejm.org 1318
september 27, 2007
–A flowing stream of blood is placed in contact with a membrane.
–A flowing stream of isotonic saline is placed on the other side of the membrane.
–The natural tendency of solutes is to equilibrate, i.e. to reach the same concentration on both
sides of the membrane, by the process known as diffusion. Urea, creatinine and other
impurities flow from the blood to the saline. Electrolytes aren’t removed because they are
already present in saline. Proteins and blood cells are too big to fit through the membrane.
–Water filters through the membrane because of trans-membrane pressure difference.
HEMODIALYSIS
THERAPY FORMAT-SUMMARY
1
P
A
T
I
E
N
T
500 ml/min
Blood
Dialysate
200 ml/min
–Patient is dialyzed for 3-5 hours, 3 times a week. Treatment is usually conducted in a free
standing Dialysis Center
–Each treatment session removes 1-3 liters of fluid and 50 ± 20 grams of uremic toxins.
–Blood is systematically anti-coagulated with heparin during treatment.
Hemodialysis
therapy format-summary
Dialysate is essentially a bicarbonate-buffered mixture of electrolytes at their normal
plasma concentration.
Blood and Dialysate flow rate, temperature, and pressures are all monitored and
controlled by a microprocessor-driven “fluid cycler.”
The blood contacting pathway is fully disposable and comprises needles, disposable
PVC tubing, and hemodialyzer.
Blood Flow varies from 300-400 ml/min. (just under a pint a minute) Dialysate is around
500-800 ml/min.
Dialysis is generally not uncomfortable; the most common adverse symptom is a sharp
drop in blood pressure leading to nausea & cramps.
Types of Membranes
Early membranes included regenerated cellulose and cellulose nitrate
although these membranes were associated with significant immune stimulation
in the patients
Modified cellulose (cellulose acetate), cellulose synthetics, and other polymers
such as polyamide, PMMA and polysulfone have replaced the original
cellulose membranes
Nucleophiles
TYPES OF MEMBRANES
•
•
•
Regenerated Cellulose (Cuprophanes)
•
Hydrophilic/form hydrogels in presence
of water
•
Low cost, high mechanical strength,
effective diffusive transport of small
solutes
•
Limited transport of middle mw solutes,
unstable nucleophilic groups,
complement activation and leukopenia,
hypersensitivity
Modified Cellulose
•
Cellulose acetate
•
Derivatized cellulose (Hemophan®)
Synthetic
•
Engineered thermoplastics (PS, PA,
PAN/PVC)
•
Hydrophobic
•
Solid structures with open void spaces
•
Less activating to complement, less
restrictive to middle and high mw
molecues
•
High cost, high hydraulic permeability
HYPERSENSITIVITY AND
HEMODYNAMICS
“First use syndrome”-Inflammation and Hypersensitivity
Toxins-ETO (sterilization) residuals
Plasticizers-Membrane mfg
Leachables-Membrane mfg
Post-perfusion syndrome (neucleophiles)
Contact phase activation
Bradykinin is formed due to contact with
the membrane
Bradykinin system activated
by Factor XII (clotting cascade)
Vasodilation
Anaphylaxis
POST-PERFUSION SYNDROME
CONTACT PHASE ACTIVATION
BRADYKININ GENERATION
POTENTIATION BY ACE INHIBITORS
Systemic inflammatory
response
Acute lung failure
Sepsis
Multi-organ failure
ECMO
ARTIFICIAL SUPPORT FOR THE HEART AND LUNGS FOR PROLONGED PERIODS OF TIME
• ECMO first developed in 1972 with initially marginal results.
• The first neonatal ECMO case – 1976; clinical trials in 1978 halted due to
high efficacy and need for therapy
• Primarily used for neonates and pediatrics but recently being used more
often for adult ARDS patients
Permselect.com
Polypropylene hollow fibers similar to dialysis (hydrophilic)
Bridge to Recovery
Bridge to Transplant
Bridge to VAD
COMPLICATIONS
•
Thrombosis and emboli formation
•
Bleeding and dissection of vessels
•
Seizures due to hemorrhage
•
Stroke
•
Pneumothorax
•
Metabolic complications due to acid-base balance (CO2 concentrations)
•
Sensory-neural complications
•
Developmental delays
http://www.elsonet.org/index.php/resources/videos/vi
ewvideo/22/elso-centers-of-excellence/ecmocentrum-karolinska.html