Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
4/20/2015
MKSAP‐BASED NEPHROLOGY REVIEW
April 2015 Updated Version
RENAL FUNCTION MEASUREMENT
• There Are Direct And Indirect Methods
– Direct Methods
• 24 Hour Creatinine Clearances
– 20‐25mgUCr/KgBWt/day for men
– 15‐20mgUCr/KgBWt/day for women
• Radionuclide Scanning Methods
– Highly‐accurate without dye nephrotosicity
– “Gold‐standard” for determining instantaneous GFR and RBF
– Indirect Methods
• Curve‐fitting Estimators Of GFR Based On Serum Creat
– Most clinical labs now use the MDRD algorithm
CLINICAL MOMENT
• You are referred a 60‐year‐old healthy woman because her PCP did an MDRD estimated GFR and her GFR was “low” at 56ml/min.
–
–
–
–
–
–
Serum creatinine 1.0mg%
Urinalysis is normal; no hematuria or proteinuria
Vital signs are normal; no Hypertension
She is well, exercises 5d/wk and no FH of CRI
Meds: Calcium carbonate and a MVI
Physical exam: Appears younger than stated age and is athletic/muscular
1
4/20/2015
CLINICAL MOMENT, CONTINUED
• Which of the following tests would be most appropriate as a next step?
– Radionuclide stress test
– Repeat the estimate of the GFR using the Cockcroft‐Gault equation
– Repeat the estimation of the GFR using the Chronic Kidney Disease Epidemiology (CKD‐Epi) Collaboration equation
– Perform a 24‐hour urine collection for CrClnc
CLINICAL MOMENT, CONTINUED
• In a low‐risk, healthy person the e‐GFR tool used is important
– MDRD underestimates GFR at higher (normal) values
– Cockcroft‐Gault also underestimates GFR, with practically the same biases
– CKD‐Epi adjusts for younger patients with higher muscle mass
– 24‐Hour Urine Collections are Logistically Difficult and often inaccurate
– Radionuclide Studies are Most Useful When High Precision, Such as Prior to Transplant, are Needed.
URINALYSIS
•
•
•
•
The Albustix Detects Albumin, Almost Totally
The Bili Tab Picks Up Only Conjugated Bilirubin
The Peroxidase Tab Detects >2‐4 RBC/Hpf
Leukocyte Esterase Detects >3WBC/Hpf
– Most Common Cause Of Pyuria Is UTI
• Nitrites Are Produced By Gram‐Negative Bacteria, Not Gm‐Positives
• The Presence Of Both LE And Nitrites Is Highly‐
Suggestive Of A UTI/Absence Of Both Carries A Very High Negative Predictive Value
2
4/20/2015
URINE MICROSCOPY
• Always View in Phase‐Contrast Mode
• Casts Are Tamm‐Horsfall Protein (Uromodulin)
– They Contain Trapped Cells And Debris
– RBC Casts Suggest Glomerulonephritis
• >2‐4 RBC’s/HPF Is Abnormal
– Most Commonly Due UTI/Stones But Caution If Neoplasia Risk Is Present
– RBC’s Resembling Schistocytes, Acanthocytes, And Helmet Cells Are “Glomerular Hematuria” Distinct From Traumatic Hematuria
• Eosinophils Indicate Allergic, Atheroembolic, Parasitic, Or Small‐vessel Vasculitic Disease
• Wright Stain Misses Most; Hansel Stain Works Best
KIDNEY BIOPSY
• Carries ~1% Major Complication Risk
• Increased Risk If Only One Funcitoning Kidney Present
• Indicated If AKI Of Uncertain Cause Or Renal Transplant Dysfunction
• If Disease Evolution Is Atypical, May Point To Second Cause Amenable To Treatment
• Rarely Useful If Kidneys Are <8cm
• Contraindicated If:
– Bleeding Disorder Or Uncontrolled HTN
– Active UTI
– Hydronephrosis
URINE CRYSTALS
• Envelope/Dumbbell/Needle Non‐Bi‐Refringent
– Calcium Oxalate
– Hypercalciuria/Hyperoxaluria/Ca‐Oxalate Stones
– Filling Slide With Acidosis; Ethylene Glycol Ingestion
• Prism/Star‐like Non‐Bi‐Refringent
– Calcium Phosphate
– RTA1/Urin Ph>6.5/Tumor Lysis/Phosphate Nephrop
• Rhomboid/Rosetts Non‐bi‐refringent
– Uric Acid
– DM/Obesity/Gout/Hyperuricemia/UpH<6.0
– In Presence Of Uurate/Ucr > 1.0 Indicates Tumor Lysis
• Coffin‐lid
– Magnesium Ammonium Phosphate (Struvite)
– Indicates Chronic UTI With Urease‐producing Organism
• Hexagons
– Cystine
3
4/20/2015
HEMATURIA
• More Than 3 RBC/HPF Is Abnormal
– Round “Isomorphic” RBC Indicate Trauma/Tumor Or Benign Inflammation
– Schistocytes/Helmet Cells/Acanthocytes Are “Glomerular” Hematuria; Suggest Glomerulonephritis
• Noncontrast Helical CT Is Technique Of Choice For Stone Eval
• Tumor/Anatomic Evaluation
• Normal GFR: CT Urography With Contrast
• E‐GFR 30‐60 mL/Min; MRI Urography • E‐GFR<30mL/min; NO CONTRAST
PROTEINURIA
• Normal Is < 200‐250mg Total Proteinuria/Day
• Microalbuminuria Is 30‐300 Mg Alb/Gm Ucr/D
– If 2 Of 3 Samples Over 6mo Is Over That, Microalbuminuria Exists Per ADA
• Proteinuria Is Best Estimated By Random Urine Protein‐to‐creatinine Ratios
–
–
–
–
<0.1 Is Normal
0.2‐1.0 Is Tubular Proteinuria
1‐2 Is Glomerular Proteinuria
>2 Suggests Nephrotic Proteinuria
• Remember; Dipstick ONLY Detects Albumin!!
PROTEIN‐TO‐CREATININE RATIO
• Random Urine Test (Best First‐AM Void)
• Based On Concept That Protein/Creatinine Are Co‐Excreted:
– Normal Person Puts Out 1‐2Gm Creatinine/Day
– Normal Urine Protein is <200‐250mg/Day
– So, Normal Ratio is <200‐250/1000‐2000, or 0.1‐0.2
– 500 mg/Day Would Give a Ratio of 0.25‐0.5
– 1000 mg/Day Would Give a Ratio of 0.5‐1.0
– Nephrotic Proteinuria (>3500mg/Day) Would Give a Ratio of 1.7‐3.5
4
4/20/2015
FLUIDS AND ELECTROLYTES
• Osmolality & Tonicity
• Tonicity Is About Water: Volume Is About Sodium
Plasma Osmoloality is in mOsm/Kg H2O
The Normal is 275‐295 mOsm/Kg
Above These Limits, ADH is Released
Below These Limits, ADH is Progressively Inhibited
Osm= 2xNa(mEq/L)+ Gluc(mg/dL)+BUN(mg/dL)
18 2.8
– A Serum Osmolal Gap > 10mOsm/Kg is abnormal
– The Body Sacrifices Tonicity for Volume Defense
–
–
–
–
–
HYPONATREMIA
• Symptoms of Hyponatremia Are Nausea, Fatigue, and Headache.
• As Hyponatremia Increases, Cerebral Edema Occurs, With Obtundation, Seizures, Coma, Hypoxia and Respiratory Arrest
• Hypertonic Saline is Indicated for Symptomatic Patients with Inappropriate ADH Secretion
• Fluid Restriction is Essential for Asymptomatic Patients With SIADH or Hypervolemic Hyponatremia
• Patients With Appropriate Hyponatremia Respond to Normal Saline.
• Acute Increase in Serum Na by 4‐6mEq/L in First 24hours Is Sufficient for Most
HYPERNATREMIA
• Causes Include Hypotonic Fluid Loss, Pure Water Loss, Diabetes Insipidus, and Hypertonic Fluid Inputs
• GI Losses, Diuretic Therapy, and Osmotic Diuresis Cause Hypernatremia in AssociationWith Hypovolemia
• Hypernatremic Correction Should Be no More Than 10mEq/L per day to Avoid Cerebral Edema
5
4/20/2015
CLINICAL MOMENT
• You admit a 63 year‐old male Veteran who arrived at the VAMC E.D. from a CNH. He weighs 88Kg.
• His history includes NIDDK Stage III chronic renal insufficiency (e‐
GFR is 38mL/min) and he has been noted to have NYHA Class III CHF.
• His serum sodium is 155mEq/L, his potassium is 3.6mEq/L, his BP is (162/78), his pulse is 100/min and regular. • His internal jugular pulse is 2‐3cm above the sternal notch lying flat, and his skin turgor is decreased (tenting of the skin is present). There are no rales on lung exam.
• He appears euvolemic to slightly hypovolemic to you. You agree with your senior Resident that the patient is free water deficient, (how much?) http://www.medcalc.com/freewater.html
• S/he asks “But if we give that much IV fluid, won’t we put him in worse CHF?”
CLINICAL MOMENT, CONTINUED
• He Is Free‐Water Deficient:
– Male; 60% of LBM is Water: 52.8 Liters
– Serum Sodium is 155mEq/L and Desired is 140
– Difference is 15mEq/L or ~10.5%
– Patient is 5.6Liters Down
• ~80% of Free Water Given IV Escapes Into the Tissues: ~1L Will Remain IV in 1‐2 Hours
• So, The Likelihood of Precipitating Worse CHF Is Very Small
HYPOKALEMIA
• Diuretic Use is the Most Common Cause
• Abnormal Skeletal and Cardiac Muscle Function are the Most Common Manifestations
• Urine Potassium/Creatinine Ratio >20mEq/Gm Indicates Renal K+ Wasting; ,15 Indicates Cellular Redistribution, Decreased Intake, or Extrarenal K+ Losses
• Patients With Large K+ Deficits & Muscle Abnl’s
Need I.V. KCl < 20mEq/hour in IVF Concentration of No More Than 40mEq/L.
6
4/20/2015
HYPERKALEMIA
• Definition is > 5.0 mEq/L in Serum
• Symptoms are Ascending Muscle Weakness, ICG Changes (Peaked T, Short QT, Incr PR, Wide QRS, Flat P, Then Sine Wave), Lethal Dysrhythmia, Paralysis.
• Diet is Factor Only When R.A. System Defect Is Present or GFR <20mL/min/1.73m2.
• Restricting Diet to 2500mg/day May Help
• I.V. Insulin with IV Glucose if BG<250mg%
• R.A.‐Suppressing Meds Require Dose‐Reduction or Discontinuation if K+ Remains >5.5mEq/L PHOSPHORUS ABNORMALITIES
• Normal is 2.5‐4.5 mg%
• Hypophosphatemia is Seen in ETOH Abuse, Critical Illness, and Malnutrition, Esp. When Hyperalimentation Is Employed.
• PO4,2mg% May Cause Muscle Weakness
• PO4< 1mg% May Impair Resp. Muscles, Cause Hemolysis, and Rhabdomyolysis
• I.V. Supplementation Is Indicated If Level is <1mg%
• May Be Very Elevated in Tumor Lysis Syndrome
ACID‐BASE
• The Primary Defect (Acidemia vs Alkalalemia) Is The Disorder Indicated by the pH; < or > 7.40
• If the HCO3 Is > 22‐24mEq/L There Is Metabolic Alkalosis/ If < 20‐22, There is Metabolic Acidosis
• If the pCO2 Is > 40mmHg, There is Respiratory Acidosis, If < 40, There is Respiratory Alkalosis
• Metabolic Acidosis Occurs When Serum Bicarbonate is Lost, Unbalanced Production & Consumption of Endogenous Acid, or I.V. Administration of Acid
• The Anion Gap (<10‐12mEq/L) Characterizes Nature of Metabolic Acidosis
• Presence of Low Serum Albumin or Unmeasured Cations
Such as Light Chains Causes a Decreased Anion Gap
7
4/20/2015
YOU CAN REMEMBER THIS
OR THIS
Condition
Expected Compensation
Metabolic Acidosis
ACUTE: pCO2 = (1.5) [HCO3} + 8
CHRONIC: pCO2 = {HCO3} + 15 Quick Check: pCO2 = Last 2 Digits of pH Failure of pCO2 to drop to expected value = complicating respiratory acidosis; excessive decrease of pCO2 = complicating respiratory acidosis
Metabolic Alkalosis
For each increase of 1mEq/L in HCO3, pCO2 increases 0.7mmHg
Respiratory Acidosis
ACUTE: 1mEq/L increases for each 10mmHg increase in pCO2
CHRONIC: 0.35 mEq/L increase in HCO3 for each 10mmHg incr pCO2
Failure of HCO3 to incr to expected value = complicating metabolic acidosis; excessive incr in HCO3 = complicating metabolic acidosis
Respiratory Alkalosis
ACUTE: Decr 0.2 mEq/L HCO3 for each 10mmHg drop in pCO2
CHRONIC: 0.45 mEq/L decr HCO3 for each 10mm decr in pCO2
Failure of HCO3 to decr to expected value = complicating metabolic alkalosis; excessive decr in HCO3 = complicating metabolic acidosis
ALGORITHM FOR DISSECTING A/B
•
•
•
•
•
•
•
•
•
•
•
•
Look at the ABG; the overall pH defines the defect; Acidemia is present if the pH is <7.38/ Alkalemia >7.42
Look at the serum bicarbonate; If it is <22mEq/L there is a metabolic acidosis, If >26mEq/L metabolic alkalosis
Look at the paCO2; If it is <38 there is a respiratory alkalosis, If >42mmHg there is a respiratory acidosis.
However, also look at the expected paCO2 from the bicarbonate in metabolic acidosis, which is [(1.5) [HCO3} + 8]. if the measured paCO2 is lower than the expected paCO2, there is a component of under‐ventilation (respiratory acidosis).
Figure the anion gap (AG); if it is >10 there is an unmeasured anion present in the blood. The gap may widen in azotemia to as much as 12‐14mEq/L without having to invoke additional anions. Albumin affects the anion gap and the gap should be corrected for the albumin as follows:
Corrected anion gap= Observed anion gap + 0.25x (normal albumin ‐ observed albumin)
Since anions are ionic partners of H+ or its equivalents, an anion gap is a sign of acidosis; add the corrected anion gap to the observed serum bicarb: that is what bicarbonate would be if the anion gap was not present.
Look at the serum sodium &chloride. They should move together with hemodilution or hemoconcentration: ‐Normal serum sodium range at VAMC: 135‐145mEq/L ‐ Normal serum chloride range is 101‐111mEq/L
If the serum sodium is above or below the normal range, the chloride should move with it. If the serum sodium is <135mEq/L, determine the difference (135mEq/L – Observed serum sodium); the chloride should have moved the same amount down from 101mEq/L. If the actual serum chloride is higher than it should be, there is an additional non‐gap (hyperchloremic) metabolic acidosis
If the serum sodium is >145mEq/L, determine the difference (Observed serum sodium‐135mEq/L); the chloride should have moved up by the same amount up from 111mEq/L. If the actual serum chloride is higher than that, suspect an additional non‐gap (hyperchloremic) metabolic acidosis
8
4/20/2015
GAP‐INCREASED METABOLIC ACIDOSIS: MORE COMPLEX THAN “MUDPILE”
•
•
•
•
•
Advanced Kidney Disease (Generally NIDDK 4 +)
Ketoacidsis of Any Cause (Alcohol or Diabetes)
D‐Lactic Acidosis (GI Blind Loop/Overgrowth)
Ethylene or Diethylene Glycol Poisoning
Type “A” Lactic Acidosis (Hypoperfusion)
– Severe Anemia, CO Poisoning, Cardiogenic, Septic or Hemorrhagic Shock, Hypoxia
• Type B Lactic Acidosis – Medications or Toxins (Many)
• Polyglutamate Acidosis (Crit.Ill, Poor Nutr, CKD, Veg)
• Salicylate Toxicity
SPECIAL GAP‐INCR MET. ACIDOSES
• Defined as Lactate Concentration > 4mg/dL
• Ethylene Glycol and Methanol Poisoning Have Severe Anion Gap Increases Associated With serum Bicarb <10mEq/L and an Osmolal Gap > 25mOsm/Kg
• Isopropyl Alcohol Does Not Cause an Anion Gap, But It Does Cause an Osmolal Gap, Unlike Methanol and Ethylene Glycol
• Fomepizole Inhibits Alcohol Dehydrogenase and Prevents Toxic Acid Metabolite Formation; It is Used in Ethylene Glycol and Methanol Toxicity
NORMAL ANION GAP ACIDOSES
• Kidney Fails to Excrete Normal 1mEq/Kg Acid
• G.I. Tract Losses of Bicarbonate
• Ureteral Surgery With Ileal or Other Urinary Diversion
• Retention of H+ Derived From Organic Acids Excreted as Sodium Salts
– Failure to Buffer in Distal Tubule With Ammonia
– Failure of Distal Tubule to Maintain H+ Gradient
– Urine Anion Gap = [Na+]+[K+]‐[Cl‐] • If Negative In Metabolic Acidosis, NH4+ is Present
• If Positive In Metabolic Acidosis, Inadequate NH4 is Being Produced: e.g.: Classic RTA
• http://www.youtube.com/watch?v=uFvHqBiZ71k
9
4/20/2015
RENAL TUBULAR ACIDOSIS
http://www.youtube.com/watch?v=lEIjCPehGKg
• Type I: Distal – Primary Tubular Injury or Disorder
•
•
•
•
Urine pH > 6
Potassium Wasting/Hypokalemia
Renal Stones and Nephrocalcinosis
Corrects With Potassium Citrate, 1mEq/KgBWt/day
• Type II: Proximal
– Proximal Tubule Spills Bicarbonate
• Urine pH <5.5 in Presence of Systemic Acidemia
• Context of Fanconi Syndrome, Low‐MW Proteinuria, Phosphaturia, Glycosuria (Ricketts and Myeloma Associations Cause More Bone Dis.)
– Hard to Correct; Prox Tubule Spills Any Bicarb Given
• May Need to Give Thiazide Diuretic to Enhance Re‐Absoprtion
• Type IV: Distal Hyperkalemia
– Hypoaldosteronism (Urine pH < 5.5); Lower K+ Corrects Acidosis
– Tubular Injury (Urine pH > 6.0); No Correction With Lower K+
METABOLIC ALKALOSIS
http://www.youtube.com/watch?v=ni‐J1bll8m4
• May Be Saline‐Responsive or Saline‐Resistant
• Net Loss of Acid or Retention of Bicarbonate
• Usually Associated With States of Increased Aldosterone
and Hypokalemia
• If Hypertension and Increased ECF, Aldo Elevated & Renin
Suppressed, Aldo Inhibitors (Spironolactone) Can Be Used
• Severe CHF With Symptomatic Edema and Increased Effective Blood Volume Respond to Acetazolamide
(Carbonic Anhydrase Inhibitor)
• Bartter/Gitelman Syndromes
– Rare, Inherited; Mimic Effects of Loop Diuretics/Thiazides, Respectively
– Hypo‐Mg++; Muscle Cramps, Postural Hypotension, Weakness
RESPIRATORY ACIDOSIS
• Results From Decreased Minute Respiratory Volume
– PaCO2 Rises, with Resulting Rise of Carbonic Acid
• Any Intrinsic Pathology Decreasing Gas Exchange Can Also Cause Respiratory Acidosis
• Fastest Way to Fix Acidosis is to Increase the Ventilation
• Hypoxia Usually Accompanies Resp Acidosis;
– Focus on Correction of Hypoxia
– If pH Drops Below 7.2 When Hypoxia Corrected, Mechanical Ventilation is Probably Needed
10
4/20/2015
RESPIRATORY ALKALOSIS
• This is a Common Acid‐Base Disorder With a High Mortality
• Salicylate Poisoning is the Most Important Cause
– Mental Status Changes, Tachypnea, and Accompanied by an Increased‐Anion‐Gap Acidosis
• If Accompanied by Lactic Acidosis, Think Sepsis or Severe Liver Disease
• This Disorder Decreases Cerebral Blood Flow, So Hyperventilation Can Decrease Cerebral Edema
CLINICAL MOMENT
• A 32‐year‐old male comes to your E.D. complaining of 3 months of progressive leg weakness, to the point for the past day he can no longer walk. There is no diarrhea or weight loss. He has had dry eyes, dry mouth, and arthralgias. He is no no medications.
• On physical his VS are normal, and his BMI is 22. There is diffuse weakness in his legs (3/5), without atrophy or tenderness.
CLINICAL MOMENT, CONTINUED
Test
Albumin
Value
4.5g/dL
Blood Urea Nitrogen
14 mEq/L
Calcium
9.1mg/dL
Sodium
139 mEq/L
Potassium
1.9 mEq/L
Chloride
116 mEq/L
Bicarbonate
13 mEq/L
Serum Creatinine
1.0 mg/dL
Magnesium
2.2 mg/dL
Phosphorus
3.6 mg/dL
Total Protein
8.9 g/dL
Urine Anion Gap
Positive
Urinalysis
Spec Grav 1.013, pH 7.0, no glucose, trace protein, no heme, no leukocyte esterase, no nitrites, Urine Anion Gap: Positive
Renal Ultrasound
Bilateral nephrocalcinosis
11
4/20/2015
CLINICAL MOMENT, CONTINUED
• Which of the Following Is The Most Likely?
– Laxative Abuse
– Gitelman Syndrome
– Distal (Type I) Renal Tubular Acidosis
– Proximal (Type II) Renal Tubular Acidosis
IT’S DISTAL (TYPE I) R.T.A.
• Normal Anion Gap Acidosis and Hypokalemia
• Causes Include AutoImmune Diseases Like the Sjogren’s This Patient Has Symptoms Of
• Rheumatoid Arthritis, and Drugs Like Lithium Or Amphotericin Can Also Cause It
• Hypercalciuria and Hypergammaglobulinemia Are Also Associated.
• Gitelman’s Is Autosomal Recessive Condition With Hypokalemia and Metabolic Alkalosis
• Laxative Abuse Is Characterized by a Negative Urine Anion Gap
• Proximal (Type I) R.T.A. Is Due to Proximal Tubular Bicarb Spilling, with Hypokalemia, Glycosuria, Metabolic Acidosis, Renal Phosphate Wasting, but The Urine pH is Less Than 5.5 When Equilibrium Has Been Reached In the Absence of Alkali Therapy, and Nephrocalcinosis is Uncommon.
HYPERTENSION
• The Greatest Single Contributor to Cardiovascular Disease, Premature Death and Disability from C‐V Disease, Worldwide
• End‐Organ Damage Occurs to the Brain, the Myocardium, and the Kidneys
– Arteriolar Narrowing in the Eyegrounds
– Presence of an S4 on Cardiac Auscultation, and an Enlarged, Forceful PMI
– Proteinuria and Decreased GFR Without Hematuria
• Secondary HTN Accounts for <10% of All HTN
– Kidney Disease Is The Most Common Cause
12
4/20/2015
BLOOD PRESSURE MEASUREMENT
• Patient At‐Rest for 5 Minutes/ No Caffeine or Nicotine for at Least 30 Minutes
• Arms Supported at Heart Level
• Auscultatory Method Preferred; If Oscillometric
Method Used, No fabric or Clothing Between Skin and Cuff Sensor. Also, Oscillometric Cuffs are Not Accurate for Irregular Pulse Patients!
• Use Correct Cuff Size (Bladder Covers 80%)
• Inflate Cuff 20‐30mmHg Above SBP
• Deflate at ~2mmHg/Second
• Record First Korotkoff Sound and Disappearance
• Average at Least Two Measurements
CLINICAL MOMENT
• 42 Year‐Old Male Follows Up With You For His Hypertension.
• 3 Weeks Ago His BP Was (152/94). He Doesn’t Recall any Prior Checks. There is No ASCVD History, and He is On No Meds.
• On P.E., He is Afebrile, BP is (150/96) Seated, Standing (158/100) Pulse is 80/min and Regular, Respirations 16/min, BMI 28. On Retinal Exam You Notice Three AV‐Crossing Defects (“Nicking”). The Remainder of the P.E. is Normal.
• All Labs; BMP, CBC, Lipid Profile, U/A Are Normal.
CLINICAL MOMENT, CONTINUED
• What is the Most Appropriate Thing to Do Next?
– Get an ECG
– Perform a Plasma Aldosterone/Plasma Renin Ratio
– Start Him on Atenolol
– Obtain 24‐Hour Ambulatory BP Monitoring Study
13
4/20/2015
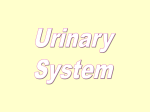
INITIAL EVAL OF ELEVATED BP
• The First thing to Do Is To Get an ECG
– You Are Looking for Secondary BP Changes: LVH, Ischemia, Old MI Signs
• Normal U/A Without Proteinuria is Good Sign
• Drug Treatment by JNCVII; Rx If BP>(140/90) on Multiple Measurements, But Beta‐Blockers Are Not First‐Line for Most
• ABPM is Reasonable If Elevated BP is “White Coat”, Less Likely In This Case
• Secondary Hypertension Workup in Atypical Cases; Younger, Refractory, Strong Family History of Secondary HTN, Spontaneous Hypokalemia. This Patient Has No Such Indications.
JNCVII EVALUATION ALGORITHM
JNCVII VERSUS “JNCVIII”
• JNCVIII: “There is strong evidence to support treating hypertensive persons aged 60 years or older to a BP goal of less than 150/90 mmHg and hypertensive persons 30 through 59 years of age to a diastolic goal of less than 90 mmHg
• However there is insufficient evidence in hypertensive persons younger than 60 years for a systolic goal, or in those younger than 30 years for a diastolic goal, so the panel recommends a BP of less than 140/90 mmHg for those groups, based on expert opinion.”
14
4/20/2015
HYPERTENSION: ADDITIONAL
• Ambulatory 24‐Hour BP Measurements Provide the Best Estimate of Cardiovascular Risk; Nocturnal BP Values are Important
• ABPM is Also Indicated in Diagnosing White‐
Coat Hypertension.
• Electronic BP‐Measurement Devices May Measure SBP Slightly Lower and DBP Slightly Higher Than Auscultatory Methods Would.
HYPERTENSION: CATEGORIES
CLASSIFICATION
OFFICE BP (mmHg)
24‐HOUR ABPM (mmHg) Averaged Over a Full 24‐Hour Recording
Normal
<120/80
<125/75
Prehypertension
120‐139/80‐89
(125‐130/75‐80)
Stage 1 Hypertension
140‐159/90‐99
>130/80
Stage 2 Hypertension
> 160/100
‐
HYPERTENSION: TREATMENT
• Lifestyle Modification Is Considered First‐Line:
–
–
–
–
Weight Loss
Reducing Sodium Intake
Aerobic Exercise 30 Minutes Each Day, 3x/Week
Reduced ETOH Consumption
• JNCVII Recommended Medical Treatment When SBP>140/90 in Patients <80 YOA, and 150mmHg If >80 YOA; JNCVII Increased SBP Limit to 150mmHg in Patients over 60 Years of Age
• If SBP Must Be Reduced >20mmHg or DBP>10mmHg, Combination Therapy Will Usually Be Required.
• If ASCVD is Present, Dropping DBP<70mmHg May
Increase MI Risk.
15
4/20/2015
RENAL‐VASCULAR HYPERTENSION
• Younger (Usually Female) Patients With Fibromuscular HTN Benefit from PCTA
• Older Patients With Atheromatous Renal‐
Vascular Disease Benefit from Aggressive Risk‐
Factor Management and Medical Treatment First, and Only Benefit From PCTA If These Have Failed.
• Resistant HTN Is Defined as Hypertension Which is Refractory to Three Medications, One of Which Is a Diuretic
SPECIAL POPULATIONS
• Women
– Same Overall Responses to Meds/Lifestyle Change
– AVOID ACEI’s/ARB’s If There is Childbearing Chance!
• Diabetes
– Aim for 130/80 Goal
– Intensive Meds May Lead to Decrease in GFR
• Black Patients
– Worse Target organ Damage at All BP Levels
– ACEI Better at Slowing Kidney Disease Rate Than B‐Blocker or Ca‐Channel Blocker • Older Patients
– SBP <150mmHg
• Cardiovascular Disease
– Do Not Lower DBP <70mmHg to Avoid Cardiovascular Events
CHRONIC TUBULOINTERSTITIAL Nephritis (TIN)
• Affect Tubulointerstitial Compartment of Kidney, and Not the Glomeruli
• Are Associated With Sub‐Nephrotic (<2.0 Gm/Day) Proteinuria, Mostly Low‐Molecular‐
Weight Proteins
• Renal Ultrasound Typically Shows Small, Atrophic Kidneys
16
4/20/2015
CAUSES OF T.I.N.
Autoimmune (Sarcoid,Sjogren,SLE,Anti‐TBM)
Balkan Endemic Nephropathy
Heavy Metal Nephropathy
Hereditary (Medullary Cystic,Mitochondrial)
Infections (BK,Brucellosis,CMV,EBV,Fungi,TBc, Legionella,Toxoplasmosis)
• Malignancy‐Related
• Medications (NSAIDs,Cy‐A/Tacro, Chinese Herbs (Aroistolochic Acid), Lithium, Cyclo‐oxygenase‐2 Inhibitors) <VIOXX>, “Goody Powder”)
• Obstruction: Prostate in Men/Repro System in Women
•
•
•
•
•
GLOMERULAR DISEASES
• Many Processes Cause Similar Changes Through Final Common Pathways
• Can Be Clinically Classified as Nephritic or Nephrotic:
– Nephritic (RBC’s, RBC Casts, Proteinuria <3.5Gm/Day, Decreased GFR)
– Nephrotic (>3.5Gm Proteinuria/Day, Decr Serum Albumin, Edema, Elevated Lipids)
PRIMARY NEPHROTIC SYNDROME
• Focal and Segmental Glomerulosclerosis (FSGS)
– 35‐45% Become Frequently‐Relapsing Corticosteroid‐
Dependent or ‐Resistant
• Membranous Glomerulopathy (MGN)
– High Rate of Spontaneous Remission; Rx With Immunosuppressives Should Be Cautious
– Anti‐Phospholipase A‐2 Receptor Antibody (“Anti PLA2R” Is Considered Diagnostic for Primary MGN
• Minimal‐Change Glomerulopathy
– Alternate‐Day Prednisone Is Best Treatment
• Fibrillary and Immunotactoid Glomerulopathies
– 60% Are Associated With Lymphproliferative Disorders
17
4/20/2015
SECONDARY NEPHROTIC SYNDROME
• Diabetes (Tight HGBA1c Control, ACEI/ARB, HTN Control are Keys)
• Amyloidosis (Best Dx is Fat‐Pad Biopsy)
• Multiple Myeloma (20% of AL‐type Have Multiple Myeloma or Other Lymphoproliferative
Disease)
• HIV‐Associated (Unique “Collapsing” FSGS)
• Hepatitis B (Most Commonly Presents as Membranous GN)
NEPHRITIC SYNDROME
• IgA Nephropathy (Berger’s Disease)
– Can be Primary, or Secondary to HIV, Chronic Liver Disease, Inflammatory Bowel Disease (IBD), or Celiac Disease
• Membranoproliferative Glomerulonephritis
– Hepatitis C (Usually With Mixed Cryoglobulinemia) , Other Chronic Indolent Infections, Autoimmune Disease (SLE), IBD, Hepatitis B (With Polyarteritis
Nodosa), Essential Cryoglobulinemia, or Malignancies
• Systemic Lupus Nephritis (Six Types)
• Anti‐GBM Disease(Linear IF Deposits on GBM Against Globular Domain Antigen on Collagen IV)
– If both Lungs and Kidneys Involved, is “Goodpasture”
NEPHRITIS, CONTINUED)
• Pauci‐Immune Crescentic Glomerulonephritis (PICG)
– One Used to be Called “Wegener’s”, But That Eponym Is Now Disused
– Proteinase‐3 or Myeloperoxidase‐ANCA Associated
– Concurrent Asthma and Eosinophilia is Called “Churg‐Strauss” Type
• Cryoglobulinemic Vasculitis
– Hep C, HIV, Lymphoproliferative Disorders, Plasma Cell Dyscrasias
– Membranoproliferative Pattern on Biopsy
• Thrombotic Microangiopathy
– Fever, Hemolytic Anemia, Consumptive Coagulopathy, thrombocytopenia, Neurologic Findings, Kidney Failure
– TTP (Decr vonWillibrand cleaving ADAMTS13 or Large VWF)
– HUS • Typically Caused by Enteric pathogens E.coli O157:H7and Shiga‐Like Toxin
• A Form Without Either May be Associated With HIV Infection
18
4/20/2015
CLINICAL MOMENT
• A 32‐Year‐Old Woman With Urinary Frequency Is Being Evaluated by You. She Denies Dysuria, Chills, Fevers, Nitesweats, and is Otherwise Apparently Healthy. She Takes a Daily MVI.
• On Physical Exam, She is Afebrile (37oC/98.7oF), BP is 149/97 mmHg, Pulse is 74/min, Respirations 18/min. BMI is 24.5. Rest of P.E. Is Normal.
• Dipstick UA Shows pH 5.5, 1+ Blood, 1+ Protein, With Negative Leukocyte Esterase. On Urine Microscopy You See RBC’s With Projections, Cuts, and “Bites” Taken Out of Them. CLINICAL MOMENT, CONTINUED
• Which Is the Most Important Next Diagnostic Test?
– Urine Culture
– Urine Protein‐to‐Creatinine Ratio and Serum Creatinine
– Kidney Biopsy
– Renal Ultrasound and Cystoscopy
URINE P/Cr AND SERUM CREATININE
• The Patient Has “Glomerular” Microscopic Hematuria; Dysmorphic Erythrocytes on Phase Contrast Microscopy
• After Determining That There is Significant Proteinuria
and Abnormal Creatinine, Next Steps Are Determining Complement Levels, Auto‐Reactive Antibiodies
(ANCA’s, FANA, Anti‐GBM, ASO), Hepatitis B and C Panels.
• If the RBC’s Were Non‐Glomerular, The Next Step Would Have Been Renal Ultrasound and Cystoscopy
• There is No Indication of Urinary Tract Infection
19
4/20/2015
GENETIC DISORDERS: ADPCKD
• Autosomal Dominant Polycystic Kidney Disease
– Most Common Inherited Kidney Disorder
– Mutations of PKD1 (85%) and PKD2 (15%)
– Kidney Ultrasound is Screen: Age>30 No Cysts Is Highly Predictive of Patient NOT Having Disease
– A Single Cyst in Patient’s <30 YOA With Family History is Specific
– Decr GFR Occurs in 3rd or 4th Decade of Life
– Pain, Infection of cysts, Kidney Stones, Cysts in Pancreas, Liver, Thyroid, Hernias, Seminal Vescicles, and Diverticulosis
– If PCKD‐Positive Family Member with Intracranial Bleed or Aneurysm, Must Screen With MRI for Brain Aneurysms
– If Hypertensive, Treat With ACEI’s
GENETIC DISORDERS: ARPCKD
• Autosomal Recessive Polycystic Kidney Disease
– Rare: Presents Early in Life With Massive Kidney Enlargement
– Mutation is in Fibrocystin Gene on Chromosome 6
– Progressive Renal Failure, Often With Hepatic Fibrosis and Portal Hypertension
– One‐in‐Four Chance of Transmission to Offspring
GENETIC DISEASES: TUBEROUS SCLEROSIS COMPLEX (TSC)
• Neurocutaneous Disorder: Many Organs Affected:
–
–
–
–
–
Benign Hamartomas of Kidney, Brain, Skin, Other
Angiomyolipomas and Kidney Cysts are Common
Cysts Cause Pain and Sometimes Hemorrhage
Renal Cell Carcinoma In 1‐2% of Adults With TSC
Diagnosis: Major Features (One Required)
• Facial Angiolipomas, >3 Hypomelanotic Macules, Renal Angiomyolipomas, Retinal Hamartomas
– Diagnosis: Minor Features (Two Required)
• Nonrenal Hamartomas, Multiple KidneyCysts, Enamel Pits on Teeth/Gingival Fibromas
20
4/20/2015
GENETIC DISEASES: ALPORT SYNDROME
• Sensorineural Hearing Loss, Lenticonus and Retinal Flecks in the Macula & Mid Periphery
• X‐Linked in 80%, Autosomal Recessive in 15%, Autosomal Dominant in 5% • More Common in Men; Women Have Milder Form • Absence of Type IV Collagen in Skin or Kidney Biopsy
GENETIC DISEASES: THIN GBM
• Variety of Inherited Conditions With Hematuria
– Up to 5% of Population May be Affected
– Often Discovered in Childhood
– Distinguished From Alport Syndrome
– Heterogenous Mutations Affecting Type IV Collagen So Skin Biopsy Will Show Reduced Collagen IV
– Prognosis is Excellent With HTN, Proteinuria Control GENETIC DISEASES FABRY’S
• X‐Linked Deficiency of Alpha‐Galactosidase‐A
• Manifestations Come From Deposition of Globotriaosylceramide (Gb3) in Lysosomes
• Urine Concentrating Defects, Proteinuria, CKD, Burning Peripheral Neuropathies, With Angiokeratomas in the Groin
• Accelerated ASCVD Is Notable Association
• Replacement Therapy With Human Recombinant Alpha‐Galactosidase‐A Is Available and Works (At a Cost of $150,000 Annually)
21
4/20/2015
CLINICAL MOMENT
• A 35 Year‐Old Woman Has Recently Been Diagnosed with APCKD By Renal Ultrasound. Her Mother Had PCKD, Hypertension and Eventual Renal Failure Requiring Peritoneal Dialysis. She Died of a Stroke. • The Patient’s Hypertension is Managed With LOSARTAN and METOPROLOL.
• On P.E. BP is 132/82mmHg, Pulse is 67/min. You Find No Flank Pain or Dependent Edema. • Lab: Serum Creatinine 1.2mg%; Urine P/C Ratio is 0.15, and Urine Microscopy Shows 5‐10 Normal RBC’s /HPF
CLINICAL MOMENT, CONTINUED
• Which of The Following Is the Most Appropriate Next Step:
– Non‐Contrast Abdominal CT Scan
– 24‐Hour Urine Collection for Protein
– Genotype Testing for APCKD Subtype
– Brain M.R.A.
M.R. ANGIOGRAM
• The Positive First‐Degree Family History of CVA Strongly Indicates Screening The Patient For Aneurysm
• Could Substitute a High‐Resolution CT Angio
• 24‐Hour Urine Collection is Not Needed; You Already Have a Urine P/C Ratio
• Genotype Testing Is Not Routine; It is Expensive and Hard to Get; and Won’t Change Management
• Abdominal CT Won’t Help At This Point; You Have the Diagnosis‐‐‐Later Screening for Malignancy My Give It a Role
22
4/20/2015
ACUTE KIDNEY INJURY
• Three Types:
– Pre‐Renal
– Intrinsic/Parenchymal
– Post‐Renal
– Occurs Within Hours to Weeks of Inciting Insult
“RIFLE” CRITERIA (2002)
Stage
GFR Criteria
Urine Output Criteria
SCr incr 1.5-2 times baseline UO < 0.5 mL/kg/h < 6 hr
or GFR decreased >25%
Injury
SCr increased 2-3 x baseline UO < 0.5 mL/kg/h >12 h
or GFR decreased >50%
Failure
SCr increased >3 x baseline
UO < 0.3 mL/kg/h 24 h
or GFR decreased 75%
or anuria for 12 h
or SCr ≥4 mg/dL; (oliguria)
or acute rise ≥0.5 mg/dL
Loss
Persistent renal failure: >4 wk
of Func- loss of function (requ dialysis)
tion
ESRD
Complete function loss >3 mo)
Risk
Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute renal failure - definition, outcome measures, animal
models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute
Dialysis Quality Initiative (ADQI) Group. Crit Care. Aug 2004;8(4):R204-12. [Medline]. [Full Text].
AKIN CRITERIA (2004)
•AKIN advised that the term acute kidney injury (AKI) be used
•Represents full spectrum of renal injury, from mild to severe, with latter
having increased likelihood for unfavorable outcomes such as loss of function
or ESRD.
•AKIN proposed the following criteria for AKI:
•Kidney function reduction within 48 hrs defined as absolute serum creatinine
increase of ≥0.3 mg/dL (≥26.4 μmol/L) or
•≥50% increase in serum creatinine of (1.5-fold from baseline) or
•Urine output reduction (oliguria of < 0.5 mL/kg/h for >6 h)
•These differ from RIFLE in several ways.
• The RIFLE criteria are defined as changes within 7 days.
• AKIN criteria suggest using 48 hours.
• AKIN classification includes less severe injury and also avoids using
glomerular filtration rate as a marker, because there is no dependable way to
measure glomerular filtration in AKI.
• These diagnostic criteria proposed only after volume status has been
optimized and urinary tract obstructions has been excluded in oliguria.
23
4/20/2015
GENERAL POINTS
• An Exhaustive History For Inciting Factors Is Required
• Urine Studies and Urilalysis Can Differentiate Between Pre‐Renal and Obstructive Causes
• A Renal Ultrasound Is the Preferred Method to Determine if Post‐Renal Obstruction is Present
– However, in Diffuse Abdominal Tumor Studding, the Ureters and renal Pelves Can Be Tacked Down and Not Dilate
DISTINGUISHING PRE‐RENAL INJURY
Fractional Excretion Of
Level Suggesting Pre‐
Renal ?Altered by Diuretics?
Sodium
<1%
YES
UREA
<35%
NO
URIC ACID
<10%
NO
Feature
Considerations
High BUN/Creatinine Ratio
May Also occur With Corticosteroid Use, Severe Catabolic State, and G.I. Bleed
Clinical Signs of Decreased Extracellular Volume
No Jugular Venous Pulse Supine, Skin Tenting, Tachycardia, Orthostatic BP Drop
Hydration with Normal Saline
Should Result in Reversal of Clinical and Chemical Signs Quickly; Can Lead to Gap‐
Negative Metabolic Acidosis
INTRINSIC/PARENCHYMAL DISEASE
• Acute Tubular Necrosis (ATN)
– Usually Nephrotoxin or Hypoperfusion/Ischemia
– Rising Creatinine, High Urine Sodium, High FeNa, Muddy Brown Dark Granular Casts in Urine, Isosthemiuria (Urine Osm near 300mOsm/Kg or Specific Gravity 1.010)
– Recovery Variable; Depends on Start Point, Age
• Non‐Oliguric (>500mL Urine/day) Better Than Oliguric
24
4/20/2015
RADIOCONTRAST RENAL INJURY
• Defined as Incr Scr 0.5mg/dL or 25% Incr @48Hr
• Risks Are Any Prior Injury, Chronic CHF, Diabetes, Intra‐Aortic Balloon Pump, Age>80 Years, Proteinuria, Dehydration
• Prevention is: Pre‐Hydration With NS (n‐
Acetylcysteine and Bicarbonate Administration Aren’t Proven to Help With Iodinated Radiocontrast Agent Toxicity), Minimal Dose of Iso‐Osmolar or Low Osmolarity Radiocontrast
• MRI Gadolinium Contrast: Associated With Nephrogenic Systemic Fibrosis ‐‐‐ Avoid
PIGMENT NEPHROPATHY
• Hemoglobin and/or Myoglobin in Renal Tubules
• Massive Hemolysis, Rhabdomyolysis
• Urine Positive for Heme, But No RBC’s
• Serum Myoglobin is Elevated
• Look for Golden Casts, Signs of Tissue Destruction or Hemolysis
• Hydration is Key; Bicarbonate Benefit Not Proven
ACUTE INTERSTITIAL NEPHRITIS
• Classic Presentation is Fever, Rash and Eosinophilia With Rising Serum Creatinine; Full Picture Is Only Seen in 10%
• Typically Caused By Hypersensitivity Reaction to Medication
• Look for a Medication Started Within Prior 7‐
10 Days
• Discontinue Suspected Agent(s), Evidence for Corticosteroid Benefit Limited, & Only If Started Early
25
4/20/2015
OTHER ACUTE KIDNEY INJURIES
•
•
•
•
•
•
•
•
•
•
•
•
•
•
HUS/TTP
Vancomycin Toxicity
IgG Preparations
Phosphate Nephropathy (Oral & Bowel Preps)
High‐Dose Vitamin C (Via Oxalate Toxicity)
ORLISTAT (“Xenical” ®Roche; Tetrahydrolipstatin for obesity)
Carambola (Star Fruit) Juice
Post‐Gastric Bypass Surgery (Oxalate Toxicity)
Increased Intra‐Abdominal Compartment Pressure
Cardiorenal Syndrome (Five Types; Comb Renal/Cardiac Dysfx)
Atheroembolic Disease (Stuttering Scr, Distal Emboli, Eos)
Severe Acute Liver Disease (HRS; Una<10, Min Uprot, Oliguria)
Tumor Lysis Syndrome (Hydration Without Bicarb, & Dialysis)
Myeloma Cast Nephropathy (Tubular Casts With Obstruction)
KIDNEY STONES:TYPES
• Calcium (80% of All Stones)
– Oxalate (Acid Urine Insol)>Phosphate (Alk. Insol)
– Hypercalciuria (Hyperparathyroid, Excess VitD, RTA)
• Struvite (10% of All Stones)
– Magnesium Ammonium Phosphate
– Caused by Bacteria Splitting Urea to Ammonia (Proteus/Klebsiella)
• Uric Acid (10% of All Stones)
– Alkalinzing Urine Dissolves Them – Allopurinol Helps if Gout Present or if Urine UA>1gm/D
• Cystine (VERY RARE)
– Crystals Have Unique Hexagonal‐Stack Shape
– Alkalinize Urine/Give Penicillamine or Tiopronin
KIDNEY STONES: MANAGEMENT
• Non‐Contrast Helical CT is First Step
• Ureteral Relaxation With Tamsulosin or Nifedipine
May Help Expulsion
• If Stone Won’t Pass, Percutaneous Urostomy and Extracorporeal Shock Wave Lithotripsy May Be Required (But ESWL Can Cause Injury)
• 24‐Hour Urine Collection for Chemical Stone Components (Ca, Oxalate, Phosphate) and Inhibitors (Citrate, Magnesium)
• Periodic Re‐Imaging and Dietary Counseling
26
4/20/2015
KIDNEY IN PREGNANCY
• Increased Renal Blood Flow, Lowered BP, Small Increase in Proteinuria, Decreased Serum Creatinine All Happen in Pregnancy
• Dilation of Renal Collecting System May Simulate Obstruction
• BP Should Be Maintained Below 150/100mmHg—
Possibly Lower if C.R.I. Present
• Discontinue Renin‐Angiotensin Blockers Prior to Attempts to Become Pregnant & Don’t Use During Pregnancy!
HYPERTENSION IN PREGNANCY
• Anti‐HTN Rx is Warranted Only to Limit Maternal end‐Organ Damage With Severe HTN
• Gestational Hypertension Develops After 20 Weeks (No Proteinuria or Other End‐Organ Dx)
• Pre‐Eclampsia is HTN and Proteinuria After 20 Weeks: If Severe, See Thrombocytopenia, Rising Scr, Elevated Liver Enzymes, Anti P‐L Abs
• Meds (In Order of Preference); Labetalol, Methyldopa, Sustained‐Release Nifedipine, Hydralazine
OTHER ISSUES IN PREGNANCY
• Women Can Carry to Term on Dialysis and With Transplants
– Hemodialysis Needs to Be Increased from ~12 to ~20 Hours Per Week to Cope With Increased Metabolic Demands
– Ideally Wait 1‐2 Years After Transplant to Conceive
• Diabetic Women on ACEI’s or ARB’s Must Have Them Stopped Before Becoming Pregnant 27
4/20/2015
CLINICAL MOMENT
• A 29‐Year‐Old Woman Comes to You for Pre‐
Conception Counseling. A Year Ago IGA Nephropathy Was Diagnosed by Renal Biopsy. She is Subjectively Well, Has No Other Medical Problems, and Is On No Meds.
• On P.E., Her BP is 138/85, Her Temperature is Normal, Pulse is 62/min, Respirations Are 17/min. Cardiovascular and Pulmonary Exams Are Normal.
• At the Time of Biopsy, Her Creatinine was 1.0mg%. Urinalysis Today Shows 15‐25 RBC/HPF and 1+ Protein on Dipstick
CLINICAL MOMENT, CONTINUED
• What Should Be Done Next?
– Re‐Measure the Serum Creatinine Level
– Measure the IgA Level
– Obtain a 24‐Hour Ambulatory BP Measurement
– Repeat the Kidney Biopsy
RE‐MEASURE THE CREATININE
• Current GFR Is the Best Guide to Pregnancy Risks, Such As Pre‐Eclampsia, Eclampsia, and Intra‐Partum/Post‐Partum Decrease in GFR
• CKD Stage III Or Higher Is a Major Risk Factor
• Level of Proteinuria At Pregnancy Start Does Not Predict Later Complications
• Measuring IgA Levels Does Not Add Information
• She Has Pre‐Hypertension; A 24‐Hour ABPM Will Not Add Information on Pregnancy Risks
• Although Risk May Differ With Different Types of Renal Pathology, Repeat Biopsy is Useless/Benefit‐Risk Missing
28
4/20/2015
CHRONIC KIDNEY DISEASE
• 13% of Population Have One Form or Other
NIDDK Stage
GFR ml/min/1.73 M2
Description
% U.S. Population
1
>90
Normal or Incr GFR; Without Kidney 2
Damage
2
60‐89
Slight Decrease of GFR, with Evidence of Other Kidney Damage
3
3
30‐59
45‐59
Moderate Decrease of GFR With or Without Other Kidney Damage
8
3A
3B
30‐44
4
15‐29
Severe Decrease of GFR, With or Without Other Kidney Damage
0.4
5
<15
End‐Stage Kidney Disease
0.2
CHRONIC KIDNEY DISEASE; FEATURES
• Anatomic or Functional Impairment of GFR for 3 Months or More
• Screening is Necessary for Persons At‐Risk for CKD, Such as Diabetes, Hypertension, Family History, Cancer, G‐U Abnormalities, Autoimmune Diseases, and Heavy/Multiple Medication Use
• Measure Serum Creatinine Level, estimate GFR. Perform Urinalysis With Microscopic Exam
PREVENTING CKD PROGRESSION
• Control Hypertension: 130/80
• Use ACEI/ARB Agents When Not Inappropriate
– AcCOMPLISH Showed Combination Dihydropyridine Ca‐
Channel Blocker With ACEI Was Superior to ACEI‐Plus Thiazide
• Monitor Serum Potassium, Phosphorus, HCO3
• Avoid Over‐Diuresing Patients in Late Stage III Through Stage 5
• Treat Progressive Acidosis With Bicarbonate
• Avoid Nephrotoxins
• Minimize Proteinuria With ACEI/ARB, and (With Caution!) Spironolactone)
• Restrict Proteins With Caution to Avoid Malnutrition
29
4/20/2015
CKD: CONCERNS
• CKD is the Most Important Non‐Traditional Risk Factor for ASCVD: All Advanced CKD Are at Increased Risk
– Smoking Cessation, Weight Loss to Lean, treat Dyslipidemias
• Bone Disease
– Vitamin D Deficiency (Check 25‐HydroxyVitD) – Check Phosphorus Level and Treat if Elevated
• (CaxPO4>55 is Vascular Calcification Risk)
• Dietary Restriction of PO4 and Oral Binders: Ca Acetate/Sevelamer/Lanthanum
– Check Intact‐PTH Level
• Too High, Get Osteitis Fibosa Cystica / Too Low; Adynamic Bone
– Bisphosphonates Used For Osteoporosis Not OK in CKD
• Anemia
– Normal Iron Stores Are the First Consideration
– Checking EPO Levels Usually Not Helpful
– Erythropoietic Stimulating Agents ONLY If HGB<10 and Iron Normal
CKD: OTHER CONCERNS
• Imaging: No or Minimal Iodinated Agents, and NO GADOLINIUM IMAGING AGENTS If GFR<30
• Vaccination: Pursue Aggressively, But NO LIVE‐
VIRUS VACCINES Closer than 3 Months to Transplant
• Many CKD Patients Have Acquired Renal Cysts; they Can Cause Pain, Bleeding or Develop Malignancies
• Avoid I.V. Lines and Needlesticks When Possible; If Must Draw Blood/Have I.V., Use Hands
• Begin ESRD Planning One Year Prior to Anticipated Dialysis; Discuss ALL Options
– These Include Doing Nothing, HD/PD, Home/In‐Center
TRANSPLANT
• Immunosuppression is Required: Graft Tolerance is Not Yet an Established Option
• Cyclosporin‐A/TACRO (Calcineurin Inhibitors) Are Nephrotoxins & Can Cause Transplant Damage, Hypo‐
magnesemia and Hyperkalemia
• Beware of Medications With Interaction With CYP3A4 Enzymes
• Post‐Transplant Infections in First Year
–
–
–
–
Polyoma BK Virus CMV/EBV
Toxoplasmosis
Other “Hidden” Viruses (Shingles/Herpes)
• Cancers – Skin, Lung, Bowel and Other Common/Usual Tumors
– Lymphoma of the CNS
30
4/20/2015
TRANSPLANT: ADD’L ISSUES
• Original Kidney Disease May Recur
– Focal Segmental Glomerulosclerosis is Common
– Thrombotic Microangiopathies (Esp With Cy‐A)
– Diabetic and IGA Nephropathies
• Cardiovascular Disease May Progress
• Re‐Start Vaccinations 6 Months After Transplant, EXCEPT NO LIVE‐VIRUS VACCINES!
• Watch for Signs of Non‐Compliance/Non‐
Adherence As Complacence Sets In.
31