Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
SPRAIN
OF
THE
PISIFORM-TRIQUETRAL
Report
A.
MCEWEN
Formerly
Perhaps
the
tenosynovitis.
flexor
first
ulnaris
was
made,
further
investigation.
suggest
uncommon
that
SMITH,
Surgical
satisfactory
the
carpi
stimulated
fusion,
least
In
Senior
Registrar,
patients
but
in
their
of
the
in
painful
conditions
of
the
series
a diagnosis
of
tenosynovitis
to respond
tests
patients
in a busy
suffering
surgical
aching
in
from
out-patient
herein
joint
The
pain
and
insertion
was
either
of flexor
in
the
Duration
symptoms
Age
18
a period
to
operative
patholog’
brought
on
carpi
ulnaris
Side
affected
Mode
onset
Right
or
was
made
worse
by
indicated
of
this
of
Plaster
2 months
Exploration
15.8.50
Re-exploration
22.6.51
Fusion
without
tion
Excision
24.10.51
of pisiform
No relief
Relieved
Temporary
internal
fixa-
10.1
20
1 year
Left
Insidious
Plaster
Operation
4 weeks
refused
30
3 weeks
Right
Followed
fall
Plaster
6 weeks
Fusion
with
internal
31.4.52
28
3 months
Left
Blow
on
wrist
Fusion
with
30.11.51
internal
fixation
18
4 years
Right
Blow
on
wrist
Fusion
with
30.11.51
internal
fixation
fifth
finger,
The
clinical
women
in
a direct
blow
and
on
between
one.
Four
the
front
the
of
that
in
interfered
with
examination
the
patient
the
was
a constant
work
unable
finding
pain.
Date
last seen
No
I.
to
29.8.52
improvement
13.8.52
5. 1 1.52
4.9.52
and
of
thirty,
The
disability
patients
and
injury,
patients
medial
was
improvement
Relieved
of the
lift
24.12.52
Relieved
a history
in all
6.1.53
union
Relieved
eighteen
Three
3 months
improvement
fibrous
Temporary
fixation
of
for
No improvement
Relieved
10.4.51
wrist.
Table
especially
of greatest
Relieved
24. 1 .50
gave
of weakness
summarised
but
ages
patients
complained
are
workers
so severe
clinical
each
a fourth
features
manual
was
were
Painful
1.52
10 weeks
of pisiform
affected
exertion,
site
seen
described
Result
Treatment
Insidious
were
was
CASES
Plaster
Excision
patients
as the
bone
pain
I
OF
Followed
fall
was
pisiform
The
Right
six
of the
years.
1 year
On
true
of
the
measures
response
the
that
of
conservative
the
of two
28
from
618
of
2 years
two
pain
is
region
during
TABLE
in the
usual
and
is
wrist
FEATURES
persistent
SUMMARY
All
to the
described,
pisiform-triquetral
department
character,
lifting.
hand
Infir;narv
this
CLINICAL
heavy
Royal
condition.
Six
as
ENGLAND
Edinburgh
failure
The
Cases
NOTTINGHAM,
diagnosis
four
sprain
of Six
JOINT
had
two
tended
a fail
referred
on
to
in Case
dominant
from
pain
fingers
except
the
two
heavy
be
3.
and
to
the
lifting.
most
severe
In Case
4 the
a teapot.
pain
THE
on
JOURNAL
resisted
OF
flexion
BONE
AND
of
JOINT
the
wrist,
SURGERY
SPR..IN
greatest
the’
ill
hea’’
object
the’
tests
pain
nliiaris
insertion
of
pail)
tile
was
l)e
triqu(’tral
were’
the’
duration
round
proi)al)le
tile
pain
joint,
anol
au
in
tllat
tile’
two
case’s
tile’
allaestilesia.
the’
chronicity
this
test
was
Ill
into)
I1OI1t’
of
of
pOsitid)ll
1)olle
pisiforni
by
spraiil
diol
011
of
Three’
llad
tilt
C1l
e)f the
crepitus.
joint
cariii
source’
deviation
of
affectc’eI
l)atie’Ilts
The
uliiar
of
flexor
pisiform
rc’lie’f
radioio!)gical
a
these
of tile
of.
is diagnostic
tile
tilese
the
held
i)Otil
the
tilat
localisation
accompanied
ailaesthetic
Patie’Ilt
Iii
suggested
comj)lained
tue
111
on
movenlent
O)f local
that
the’
supination.
accurate
nlo\’emellt
as
\s’hell
full
this
More
trioluetruni
Pain
elicited
in
and
1xtssi\’’
619
JOINT
also
lesion.
character
relaxed.
illjt’ctie)ll
forearm
bone,
of the
same’
on
are
‘as
tue
pisiform
site
laterally
given
ail\’
the
the
Pain
\Vitil
disco)very
of
niuscles
of
deviation.
hand
the
displact’d
tile
ulnar
ceiltred
followe’d
\Viiell
\Vii()
of
PISIFORM-TRI#{231}UETRAL
THE
outstretched
e’licite’d
no)rmallv
i’t’-e’al
the
-as
trieluetruni
htiio1
1)osition
in
OF
tile’
piso-
Pttit’nt5
of
for
pitill
e’xaniillatiOll
ai)nornlalit\’.
TREATMENT
I
11
\j\\.
of
aiid
iI1lIiiOl)iliSItiOIl
of
the
phiysi#{176}tlie’rtpy,
condition
aild
l)e’rtti\’e’
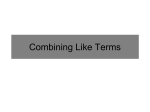
FiG.
Case-
4
--Ru(l
iographu
thi ree
iilolithis
ittt(’Iilj)tS
flexor
\‘e’re
cari
ro’lief
O)f tij)
(‘ast’
I arthiro(I(’sis
sililpl\’
(‘xCise’ei,
to
three’
to
iii
fibrous
11111011
and
‘Flit’
ne’rve’
the’
was
tissue,
\\‘iliCil
symptonis
IllOIlth.
re’fuse’(l
\\‘lle’Il
B,
NO.
an(l
4, 5, aiid
4,
uviiiuEu
in
i)otil
‘as
1)isiforni
good
Ilt’Ce’SSitate’d
riding
she
it was
to
proloiige’ol
iiidicatt’d.
I 11
vith
i)e
In
delaye’(l
coiitiiiiied
by
its
(‘ase
led
a nie’tallic
to
2 the’
painful
a
was
pisiforni
iiivolve’nient
of
ulnar
the’
relief.
enough
iiavo’
ill
t’re’
surface’s
iilsertiilg
to
justify
paul
operation
in
iIllIiiol)ilisatio)ii
to
‘l’hert’fort’
O)pe’ratio)Il
relief.
follovt’d
avoiti
to
attaCiiillg
‘l’eniporar’
rc’curred.
the
for
slip
bone’.
‘l’iie’ joint
ho)ped
severe’
the’
‘liic1i
pltster
was
i)Ilt
for
vorse
on’
after
a l)ie’yo’le’.
6 treatnle’nt
l94
was
by
I
(‘ase’
the’
1
(
te’IlOIiIloCIS
ove’r
svlllptollis
Rut
ol)eration
tO)
inll)ro)venle’ilt
later
tile
was
second
tiit’
freely
uIlde’rtaken.
joint.
excised
Collside’re’dl
months
sixte’e’n
for
re’Ce)very
a
\\‘e’re’
flision
glide’
\\‘LS
vrist
was
hut
shooving
dividiIlg
to
case’s
use’ol,
the’
tO)
Ienlj)orar\-
it.
St’e’ll
lifting,
Iii (‘ca’s
36
result
3 the’
lftit’Iit
fixation
the’
h’
joint
joillt
prxiniitv
ultiiiiate’l’
scar
carr\-iilg,
VoL.
close’
( ase
il-i
Iii
but
r(’51)Olld
ju )iIit
tendoii
pisifrIll-tri(1ue’tral
110 iiiteriial
final
affected
the
to
to be
operation
I uie’tral
leaving
follove’d,
the’
suoli
the’
re’st
niontiis
audi
lnl’
to
pisiforiii,
tile
of
foreign
excised.
Illadle’
ulnaris
failure’
se’ellie’d
I
a fter
pusiforiii-triu
t’,Vo)
its
illte’r\’t’Iltioll
excision
of
the’
joint
surfaces
aIlol
internal
fIxatioll
620
A.
by
a metal
the
screw
firm
and
screw.
In
1)ecame
the
I1tient
ofoperalion-The
cartilage’s
are
excised.
the
drill
and
the
triquetrum
joiiit
to
Tile
do) heavy
pisiform
equal
the
to
for
patients
montlls
work
n
that
tile
operation,
lateral
through
of
completely
after
the
its
triquetruni.
seven
were’
re’he’ved.
i)ut
side
exact
.-\. screv
of
is
cilo)sen.
pisifr111
and
to
avoid
sufficit’nt
lt’Ilgth
Afte’r
to
returne’d
6-Coniparative
after
vork
in
cartilage,
to
tile’
penetrate’
the
operatioll
wrist
under
thre’e
months.
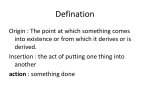
I sllo\vs
Figure
the
2
nloVerflent
operation.
\Ote
at
shigilt
aild
half
a
months
after
of dorsiflexion
capsule,
and
synovial
wrist
nionthis
extension
the’
at
Fusion
4.
Case
iii
(Fig.
membrane
three’
wrists
of
wrist.
operation
of the
both
limitation
right
three
articular
splitting
weeks.
FIG.
limitation
S
l.eft
(‘ase
slight
Case’
remained
the’ e’xpe)se-d
centre
Rig/ut
result
In
fusion
a farm.
from
is drilled
into
in plaster
symptoms
nine
is al)l)roacilt’dl
joint
a depth
three
removed
to
SMITH
the
patients
was
continued
is immol)ilised
Results-All
three
and
continued
Technique
bone,
all
loose
ME.
Histological
2).
revealed
no
of tile
pisifornl
examination
gross
results
of
in
excised
the
pathology.
DISCUSSION
Wood
act
as
as
Jones
a prime
a special
one
of
muscles
the
narrow
has
ring.
proximo-distally.
muscle
muscles
wrist
in that
a separate
The
analysed
the
antagonist,
fixation
fixation
of the
triquetral,
(1941)
mover,
joint
Both
of
the
pisiform
of
the
wrist
it gains
synovial
permits
these
function
of the
synergist,
passive
movements
fixation
for
the
joint.
partial
cavity
or
It
flexor
carpi
action
of
differs,
ulnaris
Iii its
muscle.
muscle,
latter
abductor
digiti
hovever,
from
the
insertion
into
a joint.
This
joint,
surrounded
by
a thick
cajsule
in
movement
are
in a lateral
greatest
in
TilE
direction
the
JOURNAL
and
position
OF
of
BONE
whicll
max’
capacity
it acts
quinti,
and
other
fixation
the
the
pisiformshape
active
movement
ulnar
deviation,
AND
JOINT
as
of
SURGER\’
a
SPRAIN
when
the
and
accessory
ligaments
piso-metacarpal,
abductor
attachment
ejuinti
the
to
bone
is resisted
by
its
and
special
Thus
the
ulnar
force
It
for
that
periods
of up
to
it was
because
of
patients
who
a joint
the
of withstanding
excision
of the
expose
(1947)
deep
Dupont
capsule
sex
incidence
and
by
the
strain
equal
briefly
to the
a case
Meyers
(1939).
patients.
of the
pisiform
bone
the
had
bilateral
reported
joint.
All
preliminary
the
three
in
procedure.
and
described.
he treated
that
once
the
pisiform
been
treated
had
failed
so
in
and
by
to
a
by
adjacent
of fifty
were
was
a week.
described
of calcification
plaster
it
only
of
has
patients
patients
immobilisation
Although
here
be given
cases
this
wrist
retinaculum
which
laxity
the
of
the
joint.
twelve
three
basis
flexor
prolonged
aged
of
of local
make
insertion,
be
four
described
On
condition
ligamentous
(1951)
injection
irrevocable
it could
in a boy
(1952)
Jenkins
to
that
four
conception
the
of the
ulnaris
resolve
the
symptoms
and
to the
carpi
treatment
pisiform
Phalen
two
flexor
in
This
by
it is an
to
precipitated
pillars
reference
physiotherapist
pisiform-triquetral
; in
one
of the
of painless
of
of the
patients
fail
Alternatively
have
prevents
four
might
pisiform-triquetral
one
the
in a plaster
in the
injury
permanently
the
bone
Treatment
sprain.
Furthermore
only
that
and
in older
osteoarthritis
pressure.
yielded
commented
patient
of
angle.
of
expected.
described.
pain
an
capsule
pisiform
produced
procedures
it removes
to a sprain
to
between
at
the
condition
by
relief
the
is a fusion
to
has
it
the
relieve
relief
nerve
described
and
to
the
merely
predisposes
and
the
chronic.
may
operative
likely
Osteochondritis
pisiform
the
ulnar
literature
He
(1946)
Schmier
the
the
the
to the
of twelve.
the
gives
referred
both
of
become
on
by
muscles
position
muscles
be
the
tendency
of these
any
fixation.
induced
trauma
In
the
their
supinated
This
pull
opposing
to
through
forearm
the
might
relieve
joint
so
the
the
heavy
massage.
painful
girl
of
and
treatment
pisiform
A search
by
joint
only
capable
Cyriax
by
to
the
directly
of muscles.
hand.
its
sprain
possessed
failed
the
increasingly
of plaster
of
of injury
by
is thrown
origin
; but
of the
on
piso-hamate,
muscles
with
ulnaris
a chronic
months
gives
group
carpi
carpal,
opponens
lifting
methods
a synovitis
weakness
of
movement
ordinary
a half
a history
into
may
pull
of
bone
and
deviation
is weak
transverse
hvpothenar
is pulled
immobilisation
gave
the
flexor
range
and
is supported
pathology
the
capsule
Thus
inadequate
anaesthetic
and
two
tried.
where
pathology
muscle,
pisiform
the
act
the
radial
the
flexor
the
muscular
by
pisiform
by
in full
the
immobilisation
the
short
In
the
If this
namely
distally
opposing
is considered
whom
in
the
joint.
adequate
only
deviation
of
piso-triquetral
in
fixation
opposite
full
the
retinaculum.
to be pulled
is approximately
this
to
621
JOINT
bone,
Distally
indirectly
flexor
PISIFORM-TRIQUETRAL
pisiform
relaxed.
and
tends
THE
of the
are
digiti
pisiform
OF
to
over
with
excision
of
alleviate
the
symptoms.
SUMMARY
Sprain
‘ ‘
the
of
tenosynovitis
tests
of
pisiform
of the
‘ ‘
described.
the
The
triquetral
flexor
stability
to
I wish
Mercer
the
wrist
carpi
disability
pisiform-triquetral
joint
with
the
to thank
Mr Hector
W.
for his hell)
and
advice.
joint
ulnaris
in
most
is
preferred
least
Porter
is
a
cases
clinical
from
that
excision
to
permission
to
entity.
which
is such
to
disturbance
for
definite
muscle
it can
operation
of
the
It
be
structures.
investigate
these
anti
a
the
Fusion
because
patients.
as
by
is justifiable.
pisiform
related
presents
distinguished
it
restores
Professor
\\‘alter
REFERENCES
CYRIAX,
J. (1947)
DUPONT,
R.
(1946)
S. A.
JENKINS,
33-B,
and
Soft
: Laxit#{233} ligamentaire
(1951)
Tissue
Injuries.
bilat#{233}rale
: Osteoarthritis
of tile
du
London
: Hamish
pisiforme.
Pisiform-Triquetral
Revue
Joint.
Hamilton
Medical
d’Orthop#{233}die,
Journal
of
Bone
32,
Books.
260.
and
Joint
Surgery,
532.
F. Wood
JONES,
Tindall,
and
G.
PHALEN,
34-A,
(1941)
: The
Principles
of Anatomy
as seen
in the
Hand.
Second
edition.
London
: Baiiii#{232}re,
Cox.
S.
(1952)
: Calcification
Adjacent
to
tile
Pisiform
Bone.
Journal
of
Bone
and
Joint
Surgery,
579.
SCHMIER,
A.
and
Surgery,
VOL.
: Rheumatism
Joint
36 B,
A.,
NO.
and
MEYERS,
21,
M.
789.
4, NOVEMBER
1954
P.
(1939)
: Bilateral
Osteochondritis
of
the
Pisiform.
Journal
of
Bone