Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
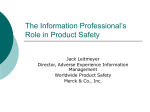
IND Annual Reporting at a Glance Kristi Wiser, Quintiles, Inc., Kansas City, MO ABSTRACT INTRODUCTION An Investigational New Drug (IND) Application is a request for authorization from the Food and Drug Administration (FDA) to administer an investigational drug or biological product to humans. During a new drug’s early development, the sponsor’s primary goal is to determine if the product is reasonably safe for initial use in humans. An IND Annual Report is required to be submitted in yearly intervals within 60 days of the anniversary date of the IND effective date. This report is required annually until the final Clinical Study Report for studies filed under the IND has been submitted to the FDA or the IND has been withdrawn. Some of the IND Annual Report required information includes a brief summary status of each study in progress or completed during the previous year and the safety of the drug as defined by adverse event tables and listings. A more complete description of the process for developing an IND Annual Report is found in the poster. IND Annual Reporting (IAR) Phase Test Population Chemistry Laboratory Screening Enzymes Cell Cultures Tissues Small animals Preclinical Animals (>1species) Phase 1 I N D S U B M I S S I O N Figure 1: Overview of U.S. Drug Development Process 20-100 healthy volunteers G G G G G What does IND mean? When is an IND initiated? How does an IND fit into drug development? What is required in an IAR? Where does Statistical Programming fit in the IAR process? CHARACTERIZATION Investigational New Drug (IND) Once the preclinical stages including the required short term animal studies have been completed, the drug is ready to be moved into human testing. Before this can happen permission for human research must be obtained by submitting an IND application to the FDA. An IND application is a request for authorization from the Food and Drug Administration (FDA) to administer an investigational drug or biological product to humans. The following table outlines the drug development process and defines where an IND fits into this process. Phase 2 100-300 patient volunteers Phase 3 1000-3000 patient volunteers N D A S U B M I S S I O N FDA Review Product Release Evaluate: Manufacturing Safety & effectiveness data Distribution Proposed labeling Advertising Education Safety reporting Phase 4 studies IND ANNUAL REPORT (IAR) before the report is due to the FDA. This notification defines the reporting period and all studies to be included. Within 60 days of the anniversary date that the IND went into effect, a sponsor is required to submit a brief report of the progress of the investigation. This takes place annually until the final Clinical Study Report (CSR) for studies filed to the IND have been submitted to the FDA or until the IND has been withdrawn. Foreign studies involving the same drug that are not being conducted in the U. S. are not required to be submitted to the IND. This brief report concentrates on the safety of the drug and is known as the IND Annual Report (IAR). The following section will define the required sections included in an IAR. IAR SECTIONS Section 1: Individual Study Information G Status of each study in progress or completed during the previous year G Subject recruitment including total number of subjects planned, enrolled (including screen failures), completed, withdrawn and active in study G Demographics tabulated by age group, gender and race Section 2: Summary Information: G AE Incidence tables by preferred term, system organ class and decreasing frequency G Listing of Expedites (unexpected SAEs related to the study drug that does not appear in the investigator brochure) in the past year G Listing of subjects who died G Listing of subjects who withdrew from the study due to an adverse event G New Information on Drug Actions G Pre-Clinical Summary G Manufacturing Changes G Microbiological Changes Section 3: General investigative plan for next year G Rationale G Indications G General Plan G Planned Trials/Expected Subject Recruitment G Anticipated Risks of Particular Severity Section 4: Investigator Brochure Section 5: Phase I protocol modifications made Section 6: Summary of foreign marketing experience Section 7: Outstanding business Components of sections 1 and 2 are generally produced by Statistical Programming/Biostatistics and the following is written from that perspective. PROCESS FOR PRODUCING COMPONENTS OF SECTIONS 1 AND 2 OF AN IAR The sponsor’s Regulatory Affairs Coordinator will send notification of a pending IND annual report 120 days Table 1 Demographics for The first step the statistical programmer takes is to notify the data coordinator(s) or clinical manager that is responsible for one or more of the studies. After receiving this notice the data coordinator(s) or clinical manager needs to identify the status of each study (database finalized, ongoing, outsourced, etc.). If the study was reported in the previous IAR as finalized (database closed) then verification needs to made as to whether there has been any changes or modifications to the database in the past year. If the study was finalized in the past year, the database to be used for reporting must be identified. For ongoing studies that will not be closed by the date the database is due for reporting, a plan needs to be set into place to provide the data needed by the due date. The data needs to be as clean as possible (adverse events, demographics, informed consent, dosing dates, treatment data) and all adverse events need to be coded if possible. When the data is clean and coded, a snapshot (copy) of the data will be taken and used to report the ongoing study. It is very important for the data coordinator or clinical manager to identify the dictionary being used to code the adverse events for each study. It is possible for one IAR to have studies coded to multiple dictionaries. Producing tables and listings for ongoing studies can be challenging. Not only can adverse events be uncoded at the cutoff date, but there can also be missing dates needed to make specific determinations or subjects not included in a dataset because the specific case report form data has not been received or entered. Ongoing studies can be problematic when reporting on blinded data. The remedy is to report the frequencies of adverse events in one column titled “Blinded Med” or “Double Blind Med” until the study is finalized and the data is unblinded. After the data specifications are in process, the existence of a project team developing the Clinical Study Report (CSR) needs to be determined. Perhaps tables and listings have been produced that could be used in the IAR. If tables and listings are available, this eliminates duplicate work and also allows the data to be provided in the same format to the FDA as in the CSR. If no CSR tables or listings have been produced then the programmer or biostatistician responsible for the IAR will need to produce the required tables and listings. Once the tables, listings and memo (defines studies included and any special instructions) are complete the report is then sent to the sponsor’s Regulatory Affairs coordinator and other responsible individuals. The following are examples tables. The first table is included in section 1 of the IAR and the remainder of the tables are included in section 2. Protocol XXXXXXXXX --------------------------------------| | | |-------------------------------+-----| |AGE (years) |0 – 15 | 11| | |---------------+-----| | |16 - 64 | 199| | |---------------+-----| | |>= 65 | 101| |---------------+---------------+-----| |GENDER |Male | 124| | |---------------+-----| | |Female | 187| |---------------+---------------+-----| |RACE |White | 170| | |---------------+-----| | |Black | 81| | |---------------+-----| | |Asian/Oriental | 43| | |---------------+-----| | |Multiracial | 17| --------------------------------------- IND ANNUAL REPORT pref02t.lst 20DEC01 Table 2.1 INCIDENCE (FREQUENCY) TABLE OF ADVERSE EVENT PREFERRED TERMS FOR FINALIZED PROTOCOL XXXXXXXXX ___________________________________________________________________________ ADVERSE EVENT PLACEBO ACTIVE DRUG N=133 N=130_____ CODED TERM N PCT N PCT ___________________________________________________________________________ UPPER RESPIRATORY INFECTION 32 24.1% 33 25.4% DIARRHEA 18 13.5% 39 22.3% NAUSEA 15 11.3% 21 16.2% HEADACHE 11 8.3% 17 13.1% INFECTION 7 5.3% 14 10.8% RASH 11 8.3% 13 10.0% DIZZINESS 7 5.3% 11 8.5% COUGH INCREASED 7 5.3% 11 8.5% BLURRED VISION 3 2.3% 10 7.7% DYSPEPSIA 6 4.5% 9 6.9% ACCIDENTAL INJURY 9 6.8% 8 6.2% ALOPECIA 5 3.8% 8 6.2% SINUSITIS 7 5.3% 7 5.4% HYPERGLYCEMIA 8 6.0% 6 4.6% HYPERTENSION 4 3.0% 6 4.6% GASTROINTESTINAL DISORDER 2 1.5% 6 4.6% LIVER FUNCTION TEST ABNORMAL 2 1.5% 5 3.8% VOMITING 5 3.8% 3 2.3% ASTHENIA 4 3.0% 3 2.3% NEUROPATHY 4 3.0% 3 2.3% RHINITIS 3 2.3% 3 2.3% ABDOMINAL PAIN 9 6.8% 2 1.5% __________________________________________________________________________ PATIENTS WITH ONE OR MORE ADVERSE EVENTS 119 89.5% 117 90.0% ADVERSE EVENTS FOR THIS TABLE ARE CODED USING THE HARTS DICTIONARY. IND ANNUAL REPORT body02t.lst 20DEC01 Table 2.2 INCIDENCE (FREQUENCY) TABLE OF ADVERSE EVENT PREFERRED TERMS WITHIN EACH BODY SYSTEM FOR FINALIZED PROTOCOL XXXXXXXXX ___________________________________________________________________________ ADVERSE EVENT PLACEBO ACTIVE DRUG N=133 N=130 BODY SYSTEM ____________ ____________ CODED TERM N PCT N PCT ___________________________________________________________________________ DIGESTIVE SYSTEM 51 38.3% 70 53.8% DIARRHEA 18 13.5% 27 20.8% NAUSEA 11 8.3% 14 10.8% GASTROENTERITIS 3 2.3% 10 7.7% DYSPEPSIA 4 3.0% 9 6.9% GASTROINTESTINAL DISORDER 2 1.5% 6 4.6% LIVER FUNCTION TEST ABNORMAL 2 1.5% 5 3.8% VOMITING 5 3.8% 3 2.3% MOUTH ULCERATION 3 2.3% 3 2.3% SORE THROAT 1 0.8% 3 2.3% GASTROINTESTINAL PAIN 2 1.5% 2 1.5% SORE MOUTH 2 1.5% 2 1.5% ULCERATIVE STOMATITIS 0 0.0% 2 1.5% STOMATITIS 3 2.3% 1 0.8% GASTRITIS 2 1.5% 1 0.8% COLITIS 0 0.0% 1 0.8% CONSTIPATION 0 0.0% 1 0.8% CHOLECYSTITIS 0 0.0% 1 0.8% FLATULENCE 0 0.0% 1 0.8% GASTROINTESTINAL PAIN 0 0.0% 1 0.8% HEMORRHOIDS 0 0.0% 1 0.8% INTESTINAL OBSTRUCTION 0 0.0% 1 0.8% APHTHOUS STOMATITIS 0 0.0% 1 0.8% ANOREXIA 0 0.0% 1 0.8% TENESMUS 0 0.0% 1 0.8% TONGUE DISORDER 0 0.0% 1 0.8% ANOREXIA 2 1.5% 0 0.0% LIVER DAMAGE 1 0.8% 0 0.0% HALITOSIS 1 0.8% 0 0.0% RESPIRATORY SYSTEM 44 33.1% 41 31.5% UPPER RESPIRATORY INFECTION 35 26.3% 29 22.3% COUGH INCREASED 7 5.3% 11 8.5% APENA 5 3.8% 4 3.1% ___________________________________________________________________________ PATIENTS WITH ONE OR MORE ADVERSE EVENTS 119 89.5% 117 90.0% ADVERSE EVENTS FOR THIS TABLE ARE CODED USING THE HARTS DICTIONARY. IND ANNUAL REPORT Table 2.3 death02t.lst 20DEC01 ADVERSE EVENT SUMMARY CUMULATIVE LIST OF SUBJECTS/PATIENTS WHO DIED ____________________________________________________________________________________________________ PROTOCOL DRUG RELATED NUMBER PATIENT TREATMENT PERIOD CAUSE OF DEATH ASSESSMENT ____________________________________________________________________________________________________ XXXXXXXXX 002007 PLACEBO POST-TRT CONGESTIVE HEART FAILURE NOT RELATED 004010 ACTIVE DRUG ON-TRT PNEUMONIA NOT RELATED ____________________________________________________________________________________________________ IND ANNUAL REPORT Table 2.4 discn02t.lst 20DEC01 ADVERSE EVENT SUMMARY CUMULATIVE LIST OF SUBJECTS/PATIENTS WHO DROPPED OUT DUE TO ADVERSE EVENT (RELATED & NON-RELATED) BASED ON ADVERSE EVENT FORM ___________________________________________________________________________________________________ PROTOCOL TREATMENT DRUG RELATED NUMBER PATIENT CODED TERM GROUP ASSESSMENT ___________________________________________________________________________________________________ XXXXXXXXX 001016 002003 002004 002006 003006 003007 003011 003012 003016 003017 004008 004014 004024 005002 00500L DIARRHEA ACTIVE DRUG RELATED LIVER FUNCTION TEST ABNORMAL ACTIVE DRUG RELATED PYOGENIC ARTHRITIS PLACEBO RELATED INFECTION PLACEBO RELATED HEADACHE ACTIVE DRUG RELATED DIARRHEA ACTIVE DRUG RELATED BONE DISORDER PLACEBO NOT RELATED BACK PAIN ACTIVE DRUG RELATED MACULOPAPULAR RASH PLACEBO RELATED ASTHENIA ACTIVE DRUG RELATED INTESTINAL OBSTRUCTION ACTIVE DRUG NOT RELATED MACULOPAPULAR RASH ACTIVE DRUG RELATED GASTROINTESTINAL HEMORRHAGE ACTIVE DRUG NOT RELATED DIZZINESS ACTIVE DRUG RELATED LYMPHOMA LIKE REACTION PLACEBO NOT RELATED MULTI ORGAN FAILURE PLACEBO NOT RELATED 005012 LIVER FUNCTION TEST ABNORMAL PLACEBO RELATED 005013 RASH ACTIVE DRUG RELATED 005018 JOINT DISORDER PLACEBO NOT RELATED 006003 ASH ACTIVE DRUG RELATED 006007 BONE FRACTURE (NOT SPONTANEOUS) ACTIVE DRUG NOT RELATED 006009 HYPERTENSION PLACEBO RELATED AUSEA PLACEBO RELATED ___________________________________________________________________________________________________ CONCLUSION Producing an IND annual report does not have to be a dreaded annual task if you are organized and have a process in place. It is also important for the departments involved to work together as a team. REFERENCES “Introduction to U.S. Drug Development”, Bill Wollberg, Quintiles internal course, March 2000 “Investigational New Drug (IND) Application Process”, http://www.fda.gov/cder/regulatory/applications/ind_pag_l. htm “Food and Drug Administration, HHS – Part 312.33 Annual Reports”, Code of Federal Regulations CONTACT INFORMATION Kristi Wiser Quintiles Inc. P. O. Box 9708 Kansas City, MO 64134-0708 Email: [email protected]