Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Epidemiology wikipedia , lookup
Genetic engineering wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
Fetal origins hypothesis wikipedia , lookup
Race and health wikipedia , lookup
Gene therapy wikipedia , lookup
Prenatal testing wikipedia , lookup
Public health genomics wikipedia , lookup
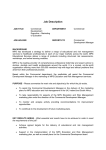
E M O RY G E N E T I C S N E W S L E T T E R FA X • J A N . 2 0 0 7 DEPARTMENT OF HUMAN GENETICS • DIVISION OF MEDICAL GENETICS • EMORY UNIVERSITY SCHOOL OF MEDICINE • ATLANTA, GEORGIA GENETIC take the ©2007 CHALLENGE test your knowledge of clinical genetics What is your diagnosis? What is Your Diagnosis? Caucasian CHIEF COMPLAINT A 12 month old Caucasian male presents with the following history: 31 y.o. 29 y.o. 12 months • • • • Developmental delay Unusual facial features Gibbus deformity Skeletal changes prompting concern of a skeletal dysplasia • Failure to thrive Te s t y o u r s e l f : answer these questions before reading the answers on page 2. 1. Which of the following tests are likely to lead to a clear diagnosis? A. Enzyme assay for alpha-L-iduronidase B . Urinary glycosaminoglycans (GAGs) analysis C. Gene sequence analysis for the IDUA gene D. All of the above PA S T M E D I C A L H I S T O RY The patient is the product of an uneventful f i r s t p r e g n a n c y. H e h a d a n i n g u i n a l h e r n i a repaired at 5 months of age. His diet consists of soy formula due to lactose intolerance. He has had no major illnesses and does not take any medications. He was able to support himself on his forearms in prone position at 3 months of age, and was rolling over at 4 months, but was not able to sit unsupported until 10 months. He is not yet crawling, cruising, or walking. 2. What is the most likely diagnosis for your patient? A. A c h o n d r o p l a s i a B. Gaucher disease type I C . Mucopolysaccharidosis type I (Hurler) D. Glycogen storage disease (Pompe) E. I-cell disease PHYSICAL EXAM 3 . What is the recurrence risk for this disorder? A. 1 % o r l e s s B. 25% C. 50% D. 100% Yo u n o t e t h a t t h e p a t i e n t h a s c o a r s e f a c i a l features, corneal clouding, and mild macroglossia. The patient has hepatosplenomegaly and a thoracolumbar gibbus. His fingers are short with unilateral c l a w i n g o f t h e 3 rd d i g i t . 4 . Is prenatal testing an option for the family’s future pregnancies? A. No, prenatal diagnosis is not available for this disorder B . Ye s , t h r o u g h b i o c h e m i c a l s t u d i e s by CVS or amniocentesis C . Ye s , t h r o u g h m o l e c u l a r s t u d i e s b y CVS or amniocentesis D . Yes, but only if the familial mutations have previously been identified in the affected child ADDITIONAL ASSESSMENTS Based on the history and physical exam, you suspect that the patient has a l y s o s o m a l s t o r a g e d i s o r d e r. T h e r e f o r e , y o u order a skeletal radiologic survey that identifies features consistent with dysostosis multiplex. FA M I LY H I S T O RY See pedigree. Patient’s parents do not have any known relatives in common. The family shares with you that they are planning to conceive a second pregnancy within the n e x t y e a r. continued next page 1 sulfate. GAGs are complex polysaccharides that are an important component of the extracellular matrix and connective tissues throughout the b o d y. D e f i c i e n c y o f t h i s e n z y m e l e a d s t o accumulation of GAGs in the lysosome, ultimately resulting in cell, tissue and organ dysfunction. If you answered 1) D, 2) C, 3) B, and 4) C&D for each question, congratulations! Yo u h a v e m a s t e r e d t h i s m o n t h ' s Genetic Challenge! FINAL DIAGNOSIS Mucopolysaccharidosis type I (MPS I) [question 2]. The urine MPS screen revealed abnormal glycosaminoglycans (GAGs) of 196.4 mg GAG/gm creatinine (normal is 2.9 - 80.5). Qualitative GAGs identified included dermatan sulfate, chondroitin 4-sulfate, and chondroitin-6 sulfate. The enzyme assay for alpha-Liduronidase revealed an enzyme level in leukocytes of 0 pmol/hr/mg protein (control range of 100-350 pmol/min/mg protein). MPS I occurs in severe, intermediate, and milder forms that cover a broad spectrum of symptoms and disease progression. MPS I is now considered a spectrum of disease, though in the past, it was divided into three subtypes based on disease severity: “Hurler” for severe MPS I, “Hurler-Scheie” for intermediate MPS I, and “Scheie” for mild MPS I. The heterogeneity of MPS I disease demonstrates a wide range of clinical involvement marked by umbilical and inguinal hernias, skeletal abnormalities, recurrent and persistent upper respiratory tract infections, coarse f a c i a l f e a t u r e s , a r t h r o p a t h y, hydrocephalus, spinal root and peripheral nerve entrapment, obstructive airway disease, sleep apnea, hearing l o s s , m a s s i v e h e p a t o s p l e n o m e g a l y, corneal clouding, glaucoma, retinal d e g e n e r a t i o n , o p t i c a t r o p h y, c a r d i a c valvular and ischemic myocardial damage. As MPS I progresses, complications become debilitating and often life threatening. FOLLOW UP After a quick search on the internet, you find that there is a lysosomal storage disease center in your area that can assist you with coordination of patient care, genetic counseling, discussion of treatment options, and participation in r e s e a r c h t r i a l s . Yo u p r o v i d e t h e f a m i l y with information about treatment options for their son, including enzyme replacement therapy and hematopoietic s t e m c e l l t r a n s p l a n t a t i o n . Yo u a l s o m a k e referrals to obtain baseline studies including echocardiogram, PT assessment to assess range of motion, developmental assessment, pulmonary function tests, MRI/CT for liver and spleen volumes, hearing exam, and brain/spine MRI. DIAGNOSIS The diagnosis of MPS I is demonstrated by deficient activity of the lysosomal enzyme alpha-L-iduronidase in peripheral blood leukocytes, cultured f i b r o b l a s t s , o r p l a s m a . H o w e v e r, t h e amount of residual enzyme does not p r e d i c t d i s e a s e s e v e r i t y. Te s t i n g f o r urinary GAGs (qualitatively or quantitatively) is a useful preliminary test; if abnormal, a MPS disorder is likely [question 1]. ABOUT MUCOPOLYSACCHARIDOSIS TYPE I MPS I is a progressive, autosomal recessive genetic disorder resulting from a defect in the gene for the lysosomal enzyme α-L-iduronidase. The genetic defect leads to a partial or complete deficiency of α-L-iduronidase a n d , s u b s e q u e n t l y, p r o g r e s s i v e accumulation of the glycosaminoglycans (GAGs), dermatan sulfate and heparan MOLECULAR TESTING MPS I is caused by mutations in the iduronidase-A (IDUA) gene on chromosome 4. For some mutations, genotype-phenotype correlations do 2 nervous system manifestations of this disease. Aldurazyme® is administered intravenously at a dose of 0.58 mg/kg, typically on an outpatient basis once per week. exist. Gene sequencing for MPS I is clinically available through Emory Genetics Laboratory and both mutations are detected in >95% of patients. Once the underlying gene mutation(s) has been identified by sequencing, family members can have carrier testing and couples can have prenatal testing, targeted for the specific gene mutation(s) [question 4]. For couples with a family history of MPS I but no living affected relatives available for testing, sequencing is available for the couple to clarify genetic counseling concerning their carrier risk. Couples who have had an affeced child with MPS I are obligate carriers and have a 1 in 4 or 25% risk for recurrence in future pregnancies [question 3]. REFERENCES & ADDITIONAL I N F O R M AT I O N : Emory Genetics Laboratory h t t p : / / w w w. g e n e t i c s . e m o r y. e d u / t e s t i n g / test.php?test_id=138 Gene Reviews h t t p : / / w w w. g e n e t e s t s . o r g / q u e r y ? d z = m p s 1 Aldurazyme Information h t t p : / / w w w. a l d u r a z y m e . c o m / National MPS Society - w w w. m p s s o c i e t y. o r g T R E AT M E N T O P T I O N S T h e r e i s n o c u r e f o r M P S I . C u r r e n t l y, a hematopoietic stem cell transplant (HSCT) from bone marrow or umbilical cord blood is the only proven therapy that can stabilize neurocognitive development and improve survival in patients with MPS I. Bone marrow transplant is most advantageous when performed on a patient with minimal symptoms of MPS I (typically before 2 years of age). HSCT has its own associated risks for complications, including developing graft versus host disease. The risk of severe complications and death varies depending upon several factors, including pulmonary function and whether there is a related versus u n r e l a t e d d o n o r. Another available treatment option for MPS I is enzyme replacement therapy with Aldurazyme®. This drug is the only enzyme replacement therapy available that treats the underlying cause of MPS I. Aldurazyme has been shown to improve pulmonary function, endurance and functional capacity as well as decrease g l y c o s a m i n o g l y c a n s ( G A G, t h e accumulated substrate), and reduce hepatomegaly in patients with this d i s o r d e r. T h e t h e r a p y h a s n o t b e e n evaluated for effects on the central 3 Ta k e t h e G e n e t i c C h a l l e n g e ! f e a t u r e s o n e o r m o r e g e n e t i c c a s e s p e r m o n t h t o t e s t y o u r k n o w l e d g e o f clinical genetics. We hope you find these cases interesting and educational. Questions or comments, p l e a s e c a l l : 1 - 8 0 0 - 3 6 6 - 1 5 0 2 o r v i s i t u s o n t h e w e b a t : w w w. g e n e t i c s . e m o r y. e d u . T h i s i s s u e o f “ Ta k e t h e Genetic Challenge!” was written by Heather Clark, MS, CGC, with edits by Daniel Gruskin, MD. Emory Department of Human Genetics revolutionizing patient care through human genetics research If you have additional questions regarding MPS I or other lysosomal storage disorders, call the Emory Lysosomal Storage Disease Center at (404)778-8565 or 1-800-200-1524, or fill out the information below, and fax this page to: FAX (404) 778-8562. Thank you. Name_______________________________________________________________________ Address_____________________________________________________________________ Phone_________________________________FAX__________________________________ I am interested in: _____Receiving this newsletter fax. Please add me beginning next month. (Name, address, phone, and fax# above must be completely filled out.) _____Please remove my fax number from the newsletter fax. _____Other:________________________________________________________________ PLEASE NOTE: In accordance with the Federal Communications Commission, this newsletter fax is for educational purposes only. Recipients may request removal by filling out the above information and faxing this page to: (404) 778-8559.