Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
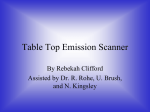
J Neurosurg 111:1201–1206, 2009 Surface-based facial scan registration in neuronavigation procedures: a clinical study Clinical article Reuben R. Shamir, M.Sc.,1 Moti Freiman, M.Sc.,1 Leo Joskowicz, Ph.D.,1 Sergey Spektor, M.D., Ph.D., 2 and Yigal Shoshan, M.D. 2 School of Engineering and Computer Science; and 2Department of Neurosurgery, Hadassah Medical Center, Hebrew University, Jerusalem, Israel 1 Object. Surface-based registration (SBR) with facial surface scans has been proposed as an alternative for the commonly used fiducial-based registration in image-guided neurosurgery. Recent studies comparing the accuracy of SBR and fiducial-based registration have been based on a few targets located on the head surface rather than inside the brain and have yielded contradictory conclusions. Moreover, no visual feedback is provided with either method to inform the surgeon about the estimated target registration error (TRE) at various target locations. The goals in the present study were: 1) to quantify the SBR error in a clinical setup, 2) to estimate the targeting error for many target locations inside the brain, and 3) to create a map of the estimated TRE values superimposed on a patient’s head image. Methods. The authors randomly selected 12 patients (8 supine and 4 in a lateral position) who underwent neurosurgery with a commercial navigation system. Intraoperatively, scans of the patients’ faces were acquired using a fast 3D surface scanner and aligned with their preoperative MR or CT head image. In the laboratory, the SBR accuracy was measured on the facial zone and estimated at various intracranial target locations. Contours related to different TREs were superimposed on the patient’s head image and informed the surgeon about the expected anisotropic error distribution. Results. The mean surface registration error in the face zone was 0.9 ± 0.35 mm. The mean estimated TREs for targets located 60, 105, and 150 mm from the facial surface were 2.0, 3.2, and 4.5 mm, respectively. There was no difference in the estimated TRE between the lateral and supine positions. The entire registration procedure, including positioning of the scanner, surface data acquisition, and the registration computation usually required < 5 minutes. Conclusions. Surface-based registration accuracy is better in the face and frontal zones, and error increases as the target location lies further from the face. Visualization of the anisotropic TRE distribution may help the surgeon to make clinical decisions. The observed and estimated accuracies and the intraoperative registration time show that SBR using the fast surface scanner is practical and feasible in a clinical setup. (DOI: 10.3171/2009.3.JNS081457) Key Words • image-guided therapy • surface-based registration • registration error I mage-guided surgery based on preoperative images and intraoperative navigation has become the standard of care for many neurosurgical procedures. A key step in image-guided surgery is the accurate intraoperative alignment, commonly called “registration,” between preoperative MR images or CT scans and the intraoperative patient situation. Three registration approaches are currently available to achieve proper alignment: 1) FBR, 2) IBR, and 3) SBR. Fiducial-based registration relies on anatomical landmarks Abbreviations used in this paper: FBR = fiducial-based registration; IBR = image-based registration; SBR = surface-based registration; SRE = surface registration error; TRE = target registration error. J Neurosurg / Volume 111 / December 2009 and/or fiducial markers affixed to the patient’s skin or skull prior to scanning. Intraoperatively, the surgeon touches the fiducial markers and/or anatomical landmarks with a tracked probe and pairs these points with their counterparts in the preoperative image.3,12,18,21 Image-based registration uses intraoperatively acquired images, such as ultrasonographic or MR images, instead of landmarks to establish image-to-patient alignment.1,20 Surface-based registration uses intraoperative 3D surface points from the patient’s anatomy, such as the face and forehead, to compute the image-to-patient transformation.4,6,8 This article contains some figures that are displayed in color online but in black and white in the print edition. 1201 R. R. Shamir et al. Surface-based registration has the following advantages over FBR and IBR: 1) it is marker free; 2) it is fast, intuitive, and easy to use; 3) it is not subject to manual pairing and localization errors; and 4) its accuracy is surgeon independent given that the surface is automatically generated by the scanner. Authors of recent studies have compared the accuracy of FBR and landmark-based registration in a clinical environment.4,7,9–11,13–16,21,22 Their conclusions are inconsistent: some authors reported that SBR is significantly less accurate than FBR,7,15,16,21,22 whereas others showed that SBR’s accuracy is similar to that of FBR.4,9–11,13,14 A possible explanation for the different results is the variation in the selected registration fiducial and target locations. As shown in clinical studies, the fiducial setup and target location do influence targeting accuracy.17–19 Therefore, any direct comparison of the FBR and SBR methods may be biased to the specific fiducial and target locations selected in the study. Furthermore, researchers in all of these studies have measured the targeting error for only a few targets located on the head surface, and thus they have made incomplete error assessments, especially for targets inside the brain. Since the actual target locations inside the brain are unknown, an error estimation method must be used to evaluate the localization error. In the study on FBR by West et al.,19 patient head images were augmented by overlaid contours that showed the estimated TREs. This visualization provided additional clinically relevant information that could help a neurosurgeon in the decision-making process. The goals in the present study on SBR were: 1) to quantify the SBR error in a clinical setup, 2) to estimate the targeting error for various locations inside the brain, and 3) to help neurosurgeons better assess the TRE by visualizing it on a patient’s head image. Methods We randomly selected 12 patients who were scheduled to undergo image-guided neurosurgeries for various clinical indications. Patient consent was obtained in all cases. Data Acquisition Protocol All patients underwent imaging the day before surgery. Contrast-enhanced T1-weighted MR images with a 1-mm slice width (Signa, GE Medical Systems) were obtained in 11 patients (93%). Contrast CT head scans (helical Twin Flash scanner, Philips Medical Systems) with a 1.3-mm slice width were obtained in 1 patient (7%). Magnetic resonance images showed 256 × 256 × 200 voxels, with a voxel size of 0.93 × 0.93 × 1 mm; CT scans showed 512 × 512 × 100 voxels, with a voxel size similar to that used in the MR imaging. The imaging volume included areas of interest inside the brain and on the facial surface. Before surgery, the head surface was automatically segmented and reconstructed, as reported in our previous study.8 Seventy-three thousand to 115,000 facial surface points were extracted from the MR imaging data sets, and 64,000 from the CT data set. After imaging and preoperative planning, the patients were taken to the operating 1202 Fig. 1. Photograph of the operating room setup showing the patient and surface scanner positions. room. After general anesthesia had been induced, 8 patients were placed supine and 4 in a lateral position. Because nasogastric tube fixation to the nose and eye draping can significantly alter facial surface geometry around the eyes and nose, we performed surface scanning prior to this time. One to 5 scans of each of the 12 patients’ faces were acquired with a root mean square point location accuracy of 0.3 ± 0.2 mm by using a commercial 3D optical surface scanner (faceSCAN II, Breuckmann) in the setup shown in Fig. 1. We acquired 34 different intraoperative scans in the 12 patients. For each patient, several scans were obtained using different scanner positions and environmental setups. We recorded all the data and brought it to our laboratory for further study. Experimental Protocol We selected the anterior facial region from the preoperative surface scan and semiautomatically extracted points on the patient’s upper facial surface, including the forehead, eyes, and nose, by using custom software. The preoperative MR image or CT scan was then aligned to an intraoperative surface scan using a robust 2-step registration algorithm (Fig. 2). The first step established a coarse correspondence based on 4 eye and nose bridge landmarks that are automatically extracted from both the MR image/CT scan and the facial surface scan data. The second step derived the registration transformation by aligning the point clouds from the MR image/CT scan and the facial surface with the robust iterative closest point registration method.2 J Neurosurg / Volume 111 / December 2009 Surface-based registration in neurosurgery procedures operating room illumination, distance and orientation of the surface scanner with respect to the patient, and the tools, tubes, and other equipment around the patient’s head. Results Fig. 2. Image demonstrating the face surface points from an intraoperative surface scan (gray points) registered to forefront surface points extracted from a preoperative MR image (red/dark points). To quantify the clinical accuracy of the SBR, we computed 2 error measurements: 1) the actual SRE, and 2) the estimated TRE. The actual SRE is the root-mean-square distance between facial surface points on the intraoperative facial surface scan and their closest corresponding points on the MR image/CT head surface after registration. Note that when the registration is based on fiducials, a compatible error is known as the fiducial registration error. The actual TRE is the distance between the true location of a predefined target and its predicted location as computed with SBR. Since targets are located inside the brain, their true location and actual TRE cannot be measured. Instead, we used the analytical formula described by Fitzpatrick et al.5 to estimate the TRE of various target locations inside the brain. This method was originally designed for FBR under the assumption of independent, identically and normally distributed landmark localization errors. From a careful examination of this method we concluded that it could be used for SBR under similar assumptions. Ten targets were selected on each patient image at increasing distances from the facial surface, and the corresponding TRE estimations were computed. Based on these estimations, isoerror value contours were superimposed on a representative MR image, providing an estimated TRE map of the brain. The results were tabulated separately for the supine and lateral positions. We also investigated registration sensitivity to scanning conditions, including internal surface scanner parameters, patient anatomical properties, and environmental parameters. Scanner parameters included the intensity of projected structured light and expected object brightness. Patient parameters included skin color and the presence/ absence of facial hair. Environmental parameters included J Neurosurg / Volume 111 / December 2009 The intraoperative surface scans were registered to the MR imaging/CT data sets in < 1 minute on a standard personal computer (2.4-GHz processor, Pentium 4, Intel). Results, which were tabulated separately for the supine or lateral positions, are summarized in Table 1. There was no difference in the measured SREs and TREs in the 2 groups. The mean SRE over all 12 patients was 0.91 ± 0.35 mm, with a range of 0.69–1.31 mm. The mean estimated TRE increased as the target location lay further from the face surface scan (Fig. 3). For example, targets located at 60, 105, and 150 mm from the patient’s face had estimated TRE ranges of 1.53–2.84, 2.26–4.53, and 2.99–6.40 mm, respectively. To better understand and visualize the clinical relevance of our results, we created estimated TRE maps by selecting a representative MR imaging slice and drawing on it the estimated TREs as isoerror value lines superimposed on the image (Fig. 4). An important finding in our study is the poor correlation between the SRE and the estimated TRE. In particular, we observed that close SRE values do not necessarily predict close TRE values: Data Sets 9 and 11 have nearly identical SRE values (0.98 ± 0.38 mm and 0.99 ± 0.42 mm, respectively) but increasingly different TRE values (2.69 and 2.17 mm at 60 mm, 4.52 and 3.49 mm at 105 mm, and 6.40 and 4.88 mm at 150 mm, respectively). Our recent research corroborates these findings.17,18 We also noted that to obtain the best results from the surface scan data, the surface scanner should be placed at a distance of 0.9–1.2 m above the patient’s head, with the internal scanner parameters for light intensity set to the 75–100 U range and the expected scanned object parameter set to “dark.” Factors such as patient skin color, facial hair, and adjacent surgical instruments did not affect registration accuracy. Discussion Our results indicated that SBR has a low average SRE of 0.91 mm in the facial zone. These results are excellent considering the intrinsic image resolution error and are comparable to those obtained using FBR based on comparable MR imaging/CT data sets.3,12,18,19 The average estimated TRE increases as the target location lies further away from the face, with errors of 4 mm in deep targets located 105 mm from the face. Observed differences between the SRE and estimated TRE in SBR were also noteworthy. The SRE, which is the only accuracy measure provided by commercial neuronavigation software for both registration methods (SBR and FBR), underestimates the TRE for structures inside the brain and thus can be misleading. As our data show, the TRE of SBR for targets at a distance of > 60 mm can be relatively high and sometimes unacceptable, even in cases in which the SRE is low. The discrepancy may be crucial for small deep targets in, for example, the basal ganglia, 1203 R. R. Shamir et al. TABLE 1: Summary of SBR accuracy results in 12 patients* Case No.† 1 2 3 4 5 6 7§ 8 average for supine position 9 10 11 12 average for lat position overall average Average No. of Face Surface No. of Points (in thousands) Intraop Surface Extracted Scan From Surface Extracted FRE Data Sets Scans From MRI/CT Measured (mm) 5 4 5 2 3 3 3 2 — 2 2 2 1 — — 1.7 2.8 1.8 2.1 2.0 1.5 2.4 2.1 2.1 1.7 2.1 2.2 2.9 2.1 2.1 81 90 110 100 90 94 64 115 93 73 96 100 104 92 93 0.69 ± 0.23 1.08 ± 0.42 0.87 ± 0.33 0.76 ± 0.30 0.81 ± 0.30 0.83 ± 0.28 1.31 ± 0.55 0.85 ± 0.31 0.91 ± 0.25 0.98 ± 0.38 0.90 ± 0.34 0.99 ± 0.42 1.09 ± 0.44 0.95 ± 0.15 0.91 ± 0.35 TRE Estimated (mm) 60 mm‡ 105 mm‡ 150 mm‡ 1.58 2.59 3.63 2.18 3.49 4.86 1.85 3.10 4.39 1.53 2.40 3.32 1.88 3.04 4.25 2.10 3.46 4.85 2.84 4.53 6.29 1.80 2.85 3.95 1.99 3.23 4.52 2.69 4.52 6.40 1.87 2.99 4.16 2.17 3.49 4.88 1.60 2.26 2.99 2.05 3.30 4.60 2.00 ± 0.55 3.24 ± 0.95 4.53 ± 1.41 * Values represent the means ± SDs, unless indicated otherwise. Patients in the first 8 cases were supine, whereas those in the last 4 cases were placed in the lateral position. — = not applicable. † Also referred to as data set number. ‡ Distance between the target and the patient’s face. § Patient underwent preoperative CT scanning; all other patients underwent preoperative MR imaging. pineal region, and cerebral peduncle as well as the upper brainstem when it is approached from anterior to the coronal suture. Therefore, a surgeon using SBR should consider the SRE as an incomplete error assessment. Our estimated TRE map (Fig. 4) shows the expected TRE at various zones of the brain image. This type of input can help the neurosurgeon select his or her approach (entry point and trajectory) using neuronavigation to a specific target while estimating the success rate (for example, correct diagnosis on stereotactic biopsy) and complication probability. Our data also suggested that SBR is feasible in a busy operating room routine. The surface scanner is used before the skin incision, does not require direct contact or sterilization, and can be moved out of the operating field for the rest of the surgery. It requires < 5 minutes to set up, with the actual scanning taking only a few seconds. The surface scan-to-image data set registration process is fully automatic and relatively short, requiring < 2 minutes’ computation time. In comparison, standard neuronavigation systems with FBR require the surgeon to manually locate and touch the anatomical landmarks, which can be an inaccurate and time-consuming process, especially when performed by an inexperienced surgeon or when the patient is placed in the lateral position. Another commercially available alternative is a tracked laser-beam line scanner (Z-touch, BrainLab). To acquire surface points, the surgeon points the laser beam to the patient’s face and moves the beam in a predefined pattern to 1204 record several hundred face surface points. This process is time consuming, user dependent, and error prone. In contrast, the fast 3D surface scanner automatically acquires tens of thousands of points, which can increase registration Fig. 3. Graph revealing the mean (center line) and SD (interval) of the estimated TRE with respect to the location of the target. It is shows that as the target lies closer to the face, the SBR is more accurate and the TRE is decreasing. J Neurosurg / Volume 111 / December 2009 Surface-based registration in neurosurgery procedures a miniature robot for keyhole neurosurgery.8 We envisage using this method for other image-guided surgery applications for which real-time tracking is not available. Conclusions Fig. 4. Expected TRE map showing the mean estimated TRE as isovalue lines superimposed on a representative MR imaging slice. accuracy, and the surface is acquired in a few seconds. The registration result is surgeon independent as he or she has no effect on the generated surface. The main drawback of our proposed method is the actual cost of a 3D surface scanner (~ €20,000, although the prices are dropping) with an accuracy of ± 0.3 mm or better. In addition, a custom stand to hold the scanner may be required in the operating room. Another limitation of our method is that none of the existing TRE estimation methods are clinically validated for image-to-patient SBR. Current TRE estimations and appropriate visualization methods need further investigation and development. A key limitation of SBR is that it does not include location information from other parts of the head and thus can be of limited use for targets in the deep temporal, parietal, and occipital lobes, basal ganglia, pineal region, and upper brainstem. We envisage 2 possible solutions. The first is the addition of 1 or 2 skin fiducial markers in strategic head locations. Although the surgeon will need to touch these fiducials with a tracked probe intraoperatively, the localization uncertainty will be much smaller than with anatomical landmarks.18 Furthermore, our and other studies indicated that adding a single fiducial marker in an optimal location can reduce the TRE by one-half.17,19 A second possible solution is to use additional uni- or bilateral ear scans. The outer ear surface provides lateral localization information that can be added to the frontal surface scan. Although the ear is flexible and deformable, we have observed that its outer surface and location with respect to the head is relatively stable. Thus, the outer ear surface can be extracted from the preoperative CT/MR image and matched with an intraoperative side surface scan. The conjunction of both data sets may provide a better distribution of registration points and allow us to obtain a smaller TRE. For the supine position, bilateral external ear scanning may provide a combination of 2 opposite surface registration data sets that may enhance TREs. Further studies will be required to explore this idea. We have integrated SBR into a system consisting of J Neurosurg / Volume 111 / December 2009 A surface-based facial scanning–to–preoperative MR imaging/CT data registration process is automatic, short, and feasible with good operating room integration. Our results on 12 patients showed that the surface registration error is ~ 1 mm in the facial zone for both supine and lateral patient positions. This level of accuracy is comparable to that obtained using FBR with skin fiducial markers in commercially available optical-based neuronavigation systems. The SBR accuracy was better in the face and frontal zones, and the estimated registration error increased as the target location lay further away from the upper facial surface and deeper inside the brain. Visualization of the mean estimated TRE as isovalue lines superimposed on a patient’s MR image can assist the surgeon in decision making while planning and executing his neuronavigation procedures. Disclosure This research was supported in part by Magneton Grant No. 34377 from the Israeli Ministry of Industry and Trade. Acknowledgment The authors thank Mrs. Shifra Fraifeld at Hadassah-Hebrew University Medical Center for her editorial assistance in the preparation of this manuscript. References 1. Amstutz C, Caversaccio M, Kowal J, Bachler R, Nolte LP, Hausler R, et al: A-mode ultrasound-based registration in computer-aided surgery of the skull. Arch Otolaryngol Head Neck Surg 129:1310–1316, 2003 2. Besl PJ, McKay ND: A method for registration of 3D shapes. IEEE Trans Pattern Anal Mach Intell 14:239–256, 1992 3. Bjartmarz H, Rehncrona S: Comparison of accuracy and precision between frame-based and frameless stereotactic navigation for deep brain stimulation electrode implantation. Stereotact Funct Neurosurg 85:235–242, 2007 4. Cao A, Thompson RC, Dumpuri P, Dawant BM, Galloway RL, Ding S, et al: Laser range scanning for image-guided neurosurgery: investigation of image-to-physical space registrations. Med Phys 35:1593–1605, 2008 5. Fitzpatrick JM, West JB, Maurer CR Jr: Predicting error in rigid-body point-based registration. IEEE Trans Med Imaging 17:694–702, 1998 6. Grimson WL, Ettinger GJ, White SJ, Lozano-Perez T, Wells WM, Kikinis R: An automatic registration method for frameless stereotaxy, image guided surgery, and enhanced reality visualization. IEEE Trans Med Imaging 15:129–140, 1996 7. Hoffmann J, Westendorff C, Leitner C, Bartz D, Reinert S: Validation of 3D-laser surface registration for image-guided cranio-maxillofacial surgery. J Craniomaxillofac Surg 33: 13–18, 2005 8. Joskowicz L, Shamir R, Freiman M, Shoham M, Zehavi E, Umansky F, et al: Image-guided system with miniature robot for precise positioning and targeting in keyhole neurosurgery. Comput Aided Surg 11:181–193, 2006 9. Marmulla R, Hassfeld S, Luth T, Mende U, Muhling J: Soft tis- 1205 R. R. Shamir et al. sue scanning for patient registration in image-guided surgery. Comput Aided Surg 8:70–81, 2003 10. Marmulla R, Muhling J, Wirtz CR, Hassfeld S: High-resolution laser surface scanning for patient registration in cranial computer-assisted surgery. Minim Invasive Neurosurg 47:72–78, 2004 11. Mascott CR, Sol JC, Bousquet P, Lagarrigue J, Lazorthes Y, Lauwers-Cances V: Quantification of true in vivo (application) accuracy in cranial image-guided surgery: influence of mode of patient registration. Neurosurgery 59 (1 Suppl 1): ONS146–ONS156, 2006 12. Maurer CR Jr, Fitzpatrick JM, Wang MY, Galloway RL Jr, Maciunas RJ, Allen GS: Registration of head volume images using implantable fiducial markers. IEEE Trans Med Imaging 16:447–462, 1997 13. Miga MI, Sinha TK, Cash DM, Galloway RL, Weil RJ: Cortical surface registration for image-guided neurosurgery using laser-range scanning. IEEE Trans Med Imaging 22:973– 985, 2003 14. Raabe A, Krishnan R, Wolff R, Hermann E, Zimmermann M, Seifert V: Laser surface scanning for patient registration in intracranial image-guided surgery. Neurosurgery 50:797–803, 2002 15. Schicho K, Figl M, Seemann R, Donat M, Pretterklieber ML, Birkfellner W, et al: Comparison of laser surface scanning and fiducial marker-based registration in frameless stereotaxy. Technical note. J Neurosurg 106:704–709, 2007 16. Schlaier J, Warnat J, Brawanski A: Registration accuracy and practicability of laser-directed surface matching. Comput Aided Surg 7:284–290, 2002 17. Shamir RR, Joskowicz L, Spektor S, Shoshan Y: Localization and registration accuracy in image guided neurosurgery: a clinical study. Int J CARS 4:45–52, 2009 1206 18. Shamir RR, Joskowicz L, Shoshan Y: Optimal landmarks selection and fiducial marker placement for minimal target registration error in image-guided neurosurgery. Proc SPIE 7261:[epub ahead of print], 2009 19. West JB, Fitzpatrick JM, Toms SA, Maurer CR Jr, Maciunas RJ: Fiducial point placement and the accuracy of point-based, rigid body registration. Neurosurgery 48:810–817, 2001 20. Wirtz CR, Tronnier VM, Bonsanto MM, Knauth M, Staubert A, Albert FK, et al: Image-guided neurosurgery with intraoperative MRI: update of frameless stereotaxy and radicality control. Stereotact Funct Neurosurg 68:39–43, 1997 21. Woerdeman PA, Willems PWA, Noordmans HJ, Berkelbach van der Sprenkel JW: Clinical accuracy of neuronavigation using registration methods based on point-pairs or surface matching. Int J CARS 1:297–299, 2006 (Abstract) 22. Woerdeman PA, Willems PW, Noordmans HJ, Tulleken CA, Berkelbach van der Sprenkel JW: Application accuracy in frameless image-guided neurosurgery: a comparison study of three patient-to-image registration methods. J Neurosurg 106:1012–1016, 2007 Manuscript submitted November 9, 2008. Accepted March 19, 2009. Please include this information when citing this paper: published online April 24, 2009; DOI: 10.3171/2009.3.JNS081457. Portions of this work have been presented as an extended abstract at the CARS 2007, Computer-Assisted Radiology and Surgery 21st International Congress in Berlin, Germany. Address correspondence to: Reuben R. Shamir, M.Sc., School of Engineering and Computer Science, Hebrew University, Givat Ram Campus, Jerusalem, Israel 91904. email: [email protected]. J Neurosurg / Volume 111 / December 2009