Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Presented at SPIE Medim 2007, San Diego, CA, Feb 2007
1
Clinical Determination of Target Registration Error of an ImageGuided Otologic Surgical System using Patients with Bone-Anchored
Hearing Aids
Ramya Balachandrana, Robert F. Labadieb, J. Michael Fitzpatricka
a
Dept. of Electrical Engineering and Computer Science
Vanderbilt University, Nashville, TN 37212, USA
{ramya.balachandran, j.michael.fitzpatrick}@vanderbilt.edu}
b
Dept. of Otolaryngology-Head and Neck Surgery
Vanderbilt University Medical Center, Nashville TN 37232
[email protected]
ABSTRACT
Image guidance in otologic surgery has been thwarted by the need for a non-invasive fiducial system with target
registration error (TRE) at the inner ear below 1.5mm. We previously presented a fiducial frame for this purpose that
attaches to the upper dentition via patient-specific bite blocks and demonstrated a TRE of 0.73mm (±0.23mm) on
cadaveric skulls. In that study, TRE measurement depended upon placement of bone-implanted, intracranial target
fiducials—clearly impossible to repeat clinically. Using cadaveric specimens, we recently presented a validation method
based on an auditory implant system (BAHA System®; Cochlear Corp., Denver, CO). That system requires a skullimplanted titanium screw behind the ear upon which a bone-anchored hearing aid (BAHA) is mounted. In our validation,
we replace the BAHA with a fiducial marker to permit measurement of TRE. That TRE is then used to estimate TRE at
an internal point. While the method can be used to determine accuracy at any point within the head, we focus in this
study on the inner ear, in particular the cochlea, and we apply the method to patients (N=5). Physical localizations were
performed after varying elapsed times since bite-block fabrication, and TRE at the cochlea was estimated. We found
TRE to be 0.97mm at the cochlea within one month and 2.5mm after seven months. Thus, while accuracy deteriorates
considerably with delays of seven months or more, if this frame is used within one month of the fabrication of the biteblock, it achieves the goal and in fact exhibits submillimetric accuracy.
Keywords: Image-guided therapy, localization, registration, validation
1. INTRODUCTION
Fiducial systems are common in image-guided neurosurgical procedures. They usually employ bone-implanted markers
and provide submillimetric accuracy. For non-malignant cases, like otologic surgery, these invasive methods are not
acceptable. A non-invasive but still accurate fiducial system is preferred for image-guided otologic surgery. Such a noninvasive system was developed here at Vanderbilt University. This system consists of a fiducial frame that can be
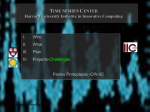
attached to a subject repeatedly via a custom-made dental bite block [1, 2, 3, 4]. Figure 1 shows the fiducial frame
attached to a patient. This fiducial frame is similar to the frame developed by Edwards et al. [5]. The frame supports 12
fiducial markers that surround the surgical field of interest, the ears. The fiducial markers can be localized in the physical
and image space, and they provide the transformation between the physical and image space. Clinically, it is important to
document the target registration error (TRE) of this system at the surgical target. Skull-based studies conducted
previously showed that this system has submillimetric accuracy [3, 4, 6, 7]. The mean TRE in the surgical field was
found to be 0.73mm±0.23mm with a root-mean-square value of 0.77mm by implanting markers in cadaveric skulls [3, 4,
6].
2
Presented at SPIE Medim 2007, San Diego, CA, Feb 2007
(b)
(a)
Figure 1. Fiducial frame system. (a) Imaging markers attached to the frame on the fiducial posts, (b) dental
bite block.
A unique method was described to perform clinical validation of the system without the need for intra-operative data
collection, and proof of concept was demonstrated on cadaveric specimens for determining targeting accuracy at the
cochlea [7]. This method requires participation of patients with bone-anchored hearing aid (BAHA®). These patients
have a titanium screw implanted behind the ear. A fiducial marker was attached to the screw, and TRE was measured at
that position. From that measurement, TRE can be estimated at other positions. This validation method does not require
any operating procedure time. All the measurements can be done in a laboratory. IRB approval was obtained to conduct
this clinical validation with patients. In this paper we report the results of a clinical validation study of the same system
using five BAHA patients. We also show the time-dependence of the fiducial marker system regarding accuracy (TRE).
2. METHODS
The validation study requires participation of patients who have undergone BAHA® implantation for hearing
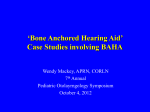
restoration. The BAHA® system (www.entific.com) consists of three parts: a titanium screw implant, an external
abutment and a sound processor (Figure 2). The titanium screw is surgically implanted into the skull behind the ear, and
an external abutment affixes to the screw. The sound processor is detachably installed on the external abutment. For our
validation study, we detach the sound processor and attach a fiducial post designed such that one end of it snaps onto the
external abutment and the other end receives a target marker (Figure 2).
3
Presented at SPIE Medim 2007, San Diego, CA, Feb 2007
(b)
(c)
(d)
(a)
Figure 2. BAHA® Target System. (a) Sound processor, (b) the abutment attached to the implant, (c) new fiducial post,
and (d) target physical marker (divot cap).
Informed consent is obtained from each patient participating in the validation study. Dental impressions are obtained for
each patient, and a bite block is made customized to that patient. The fiducial frame is attached to the bite block and the
bite block is attached to the patient’s dentition. Imaging markers are attached to the fiducial posts on the frame. Acustar-I
markers (z-kat, Inc, Hollywood, FL) , both imaging markers and physical markers, which are known as “divot caps” (see
below), were used in this work, both on the frame and as targets. (We use the term “physical” to apply to markers that
are used outside the scanner and measurements that are made outside the scanner.) The BAHA sound processor is
removed, and the new fiducial post along with the target marker is snapped on to the external abutment. CT scans are
obtained using a protocol clinically applicable for the temporal bone. Figure 1 shows the set up for the CT scan for a
patient. After scanning, the fiducial frame and the bite block are removed from the patient. All the markers are localized
in the CT image space using an algorithm described in [8]. The patient then returns to our laboratory for physical
measurements. For those physical measurements, positions of all the markers are obtained using a hybrid Polaris infrared
tracking system (Northern Digital Inc; Waterloo, Ontario, Canada) in its passive mode (i.e., infrared radiation generated
by the system is reflected by reflective balls and then detected by the system).
Figure 3 shows the physical acquisition of the markers using a coordinate reference frame (CRF)1. The CRF is rigidly
attached to the patient or to the fiducial frame during the physical localizations. The physical positions of all the markers
are obtained relative to the CRF. This allows movement of the object attached to the CRF relative to the tracking system
during the physical localizations. The fiducial frame is first attached to the CRF, and the positions of the twelve fiducial
markers are obtained relative to the CRF (Figure 3a). The imaging markers are replaced with divot caps for physical
measurements. The divot cap is such that when the probe tip is placed on the divot, the center of the probe tip represents
the center of the imaging marker. After obtaining the physical position of all the 12 markers, the CRF is removed and
attached to the bite block of the patient. The bite block is reattached to the patient (Figure 3b). A divot cap replaces the
BAHA target marker, and the physical location of the target marker is obtained relative to the CRF.
The 12 fiducial marker positions are used to find the rigid registration between image space and physical space. The
registration minimizes fiducial registration error (FRE) using the singular value decomposition of the cross covariance
matrix [9]. FRE is defined as the root-mean-square (RMS) distance between the corresponding fiducials after
registration. If { xi } and { yi } , i = 1…N are the two sets of three dimensional vectors representing the positions of N
fiducial marker, then the registration minimizes
FRE 2 =
1
1
N
N
∑ Rx + t − y
i =1
i
i
2
(1)
The CRF shown in Figure 3 supports markers for two different tracking systems. The arrangement of reflective balls on the CRF
corresponds to the reference system that we used for the hybrid Polaris system operating in its passive mode. The checkerboard
pattern markers correspond to a different tracking system that was being tested but not reported on here.
4
Presented at SPIE Medim 2007, San Diego, CA, Feb 2007
Probe
Probe used
used for
for
localization
localization
Probe used for
localization
CRF
CRF
(a)
(b)
Figure 3. Physical data acquisition. (a) Acquisition of the fiducial markers positions with CRF attached to the frame. (b) Acquisition
of the BAHA® target marker position with the CRF attached to the patient using the bite block.
where R is the three-dimensional rotation matrix and t is the three-dimensional translation vector. N is 12 in our case.
The FRE is due to the error in localizing the fiducials, called fiducial localization error (FLE), in the image and physical
space. FLE can be estimated from FRE as follows [9, 10]:
FLE 2 = N FRE 2
( N − 2) ,
(2)
where . represents the expected value.
The effect of FLE also introduces error at target point. The target point is any point other than the fiducials used for the
registration and intuitively refers to points in the surgical area. The error due to FLE is a component of the total TRE that
a surgeon can expect during the surgery at that target point. The TRE introduced at a target point r due to the FLE can be
estimated as follows [9, 10]:
TRE 2FLE ( r ) =
FLE 2 1 3 d k2
1 + ∑
N 3 k =1 f k2
(3)
where dk is the distance of r from the kth principal axis of the fiducial set, and fk is the root-mean square distance of the
fiducials themselves from the kth principal axis.
The bite block is removed from the patient after the imaging is done and reattached during the physical data acquisition
of the BAHA target marker. The error in reattaching the bite block at the same position relative to the teeth results in
error in placing the fiducial frame (virtually) at the same pose (position and orientation) relative to the patient. This biteblock relocation error is a major component of the total TRE measured at any target point [6, 7]. This error component
will be referred as TREframe, and can be assumed to be uncorrelated to TREFLE. Thus, in terms of expected values these
two error components add in quadrature as follows:
2
TRE 2 ( r ) = TRE 2FLE ( r ) + TRE frame
(r ) ,
(4)
where TRE(r ) is the total expected TRE at the target point r. Thus, at the BAHA target
2
TRE 2 ( BAHA ) = TRE 2FLE ( BAHA ) + TRE frame
( BAHA ) .
(5)
We can measure the error at the BAHA target marker using the localized positions of the marker in the image and
physical space. This measured TRE at the BAHA includes an additional error which we call “target localization error”
(TLE). It is the error in localizing the BAHA target marker. It can be assumed to be uncorrelated to the other TRE
components. Thus,
5
Presented at SPIE Medim 2007, San Diego, CA, Feb 2007
TRE 2measured ( BAHA ) = TRE 2 ( BAHA ) + TLE 2BAHA .
(6)
The BAHA target marker is of the same type as the fiducial markers, and therefore TLE 2BAHA = FLE 2 . Furthermore,
FLE 2 can be estimated using Eq. (2).
For our study we focus on finding the TRE at the cochlea of the inner ear, a statistic that has impact on image-guided
surgery in this anatomical area. We do this by estimating the value of TRE at the cochlea from the TRE measured at the
BAHA [7]. TRE at the cochlea, like TRE at the BAHA, is due to FLE and bite-block relocation error, and hence has an
expression similar to Eq. (4):
2
TRE 2 ( cochlea ) = TRE 2FLE ( cochlea ) + TRE frame
( cochlea )
(7)
2
TRE 2FLE ( cochlea ) can be computed using Eq. (3). TRE frame
( cochlea ) can be estimated from the value of
2
TRE frame ( BAHA ) as follows: The distances of the cochlea and the BAHA marker from the teeth are large compared
to the distance across the teeth themselves. So we can assume that the error due to repositioning of the frame is
dominated by the rotational errors in the reattachment of the bite block to the teeth. Due to this dominance, we can
expect the error due to repositioning of the frame at a point r to be approximately proportional to the distance of r from
the teeth. Assuming exact proportionality, we can expect the following relationship to be true:
d ( cochlea )
2
2
TRE frame
( choclea ) ≈
TRE frame ( BAHA ) ,
d
BAHA
(
)
2
(8)
where d(cochlea) and d(BAHA) are the distances of the cochlea and the BAHA, respectively, from the center of the
2
teeth. From Eqs. (5) and (6), we can get an expression to compute TRE frame
( BAHA ) as
2
TRE frame
( BAHA ) = TRE 2measured ( BAHA ) − TRE 2FLE ( BAHA ) − TLE 2BAHA .
(9)
TRE 2FLE ( BAHA ) and TLE 2BAHA can be computed using Eqs. (3) and (2) respectively. TRE 2measured ( BAHA ) can be
2
calculated using the BAHA target marker positions in the image and physical space. Thus, TRE frame
( BAHA ) can be
2
computed using Eq. (9). TRE frame ( cochlea ) is then obtained using Eq. (8), which is then applied to Eq. (7) to compute
the total TRE squared value expected at the cochlea and1hence
the expected TRE value at the cochlea. Finally, we report
2
root-mean-square (RMS) values, where RMS ( x ) ≡ x 2 .
3. RESULTS AND DISCUSSION
The IRB-approved validation study was conducted using five patients (1 male, 4 female, 23 to 64 years old) who have
undergone BAHA® implantation for hearing restoration. Informed consent was obtained following which dental
impressions were made and a customized bite block was prepared. Once the bite block was made, the patient came to
obtain the CT scan. The fiducial frame with 12 markers was attached to the patient cantilevered from the bite block to
surround the external ears. The BAHA sound processor was replaced with the specially-designed fiducial post and a
target marker. Clinically-applicable, temporal-bone CT imaging was performed. The fiducial frame and the bite block
were removed from the patient. The patient then returned to our laboratory for physical data measurements. The CRF
was attached to the fiducial frame. The imaging markers were replaced with divot caps for the physical localization. The
physical positions of the fiducial markers were obtained using the Polaris tracking system. The CRF system was then
removed from the frame and attached to the patient using the bite block. The BAHA target marker was replaced with a
divot cap. Three physical acquisitions were obtained for the BAHA marker, and the bite block along with the CRF was
removed from the patient. The fiducial and target markers were localized in the CT image space using the algorithm
described in [8]. Rigid body point-based registration was performed using the fiducials markers to provide the mapping
between the image and physical space [9]. RMS TRE was then calculated at the BAHA target using the position of the
BAHA marker in both the image and physical spaces. The error components of TRE at the BAHA due to localization
error of the fiducials and the target marker were computed, and the bite block relocation error component was computed
using Eq. (9). The position of the cochlea was obtained in the CT image space manually. The approximate frame
Presented at SPIE Medim 2007, San Diego, CA, Feb 2007
6
component of the TRE at the cochlea was computed using Eq. (8), and the error component at cochlea due to FLE was
computed using Eq. (3). Then the total expected TRE at the cochlea was computed using Eq. (7).
Due to constraints of patients’ schedules, some patients returned for the CT scan and physical data acquisitions
immediately after the bite block was made, while others were delayed by weeks to months. We discovered that the TRE
depended on the time from obtaining the dental impressions to physical space data acquisition. Once this trend was
recognized, we collected additional data from patients who had experimentation performed at an early time point. There
were totally nine physical data acquisitions obtained amongst which 5 were taken within 40 days of obtaining the dental
impressions and the other 4 were taken after almost 7 months2. Table 1 reports the RMS error values observed over all
the trials.
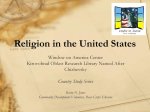
Figure 4 shows a plot of TRE at the cochlea versus the number of days elapsed between obtaining the dental impression
and the physical data acquisition. A clear distinction can be seen in the TRE values over time. TRE values obtained
during different data acquisitions for the same patient are connected using straight lines to highlight the intra-patient
increase of TRE with respect to time. We noticed two clusters in the plot. One of the clusters corresponds to the
collection of TRE values obtained when the system was used immediately after receipt of the dental impression
(typically 1-2 weeks). All the TRE values in this cluster were less than 1.5mm and the RMS TRE value at the cochlea
was found to be 0.97 mm (standard deviation 0.35mm). The other cluster in the plot corresponds to the TRE values
obtained when the system was used after few months of obtaining the dental impression. The RMS TRE value at the
cochlea was found to be 2.5 mm (standard deviation 0.91mm) for this cluster.
The bite block is designed to exactly match the dental impression obtained for the patient to make sure that the bite block
fits the teeth in the same way repeatedly. The teeth arrangement may change slightly over a few months. If such a
change takes place, the bite block will not fit exactly to the teeth and will be more likely to vary every time we remove
and attach the bite block to the patient. This variation will cause an increase in the bite block relocation error and is a
likely cause of the increase in the TRE frame ( BAHA ) and TRE frame ( cochlea ) with time. Thus the overall accuracy of
the system deteriorates over time. The error component due to FLE does not change much though because there are no
changes expected in the anatomy of the inner ear, and the localization accuracy of the markers remains approximately
the same throughout. We also note that the main component of the total error is the bite-block relocation error, as noted
for skulls in [6, 7].
4. CONCLUSIONS
In this paper we described a validation study for a fiducial system designed for image-guided otologic surgery using
patients who are BAHA® recipients. This is, to our knowledge, the first presentation of clinical use of the BAHA system
to validate an image-guided surgical system. BAHA patients constitute a unique patient population upon which
validation studies of image-guided surgical systems can be performed. The validation method involves obtaining a CT
scan wearing a fiducial frame and some measurements in the laboratory. TRE is measured at a remote location using the
measurements, and the TRE at the desired location is estimated from that measurement. Thus, the whole study is done
outside the operating room saving operating room time and providing flexibility to conduct the study. While this method
can be employed to estimate accuracy at any point within the head, we have chosen to focus for this study on the cochlea
in the context of image-guided surgery in the inner ear.
Furthermore, this is the first work that shows the dependence of the accuracy of a bite-block registration system upon the
time elapsed after fabrication of the bite block. Clinically, our dental affixed fiducial system is shown to achieve a TRE
of less than 1.5mm at the inner ear with an RMS value of 0.97mm±0.35mm when used within one month from the time
of bite block fabrication. If the system is used seven months or more after the time of fabrication, the accuracy
deteriorates. In the usual circumstances, the surgery will be conducted within 1-2 weeks of the bite block fabrication, and
our system is shown to be accurate for those circumstances.
2
One of the fiducial posts in the fiducial frame was damaged and modified between the time the CT scan of some patients was
obtained and the physical data was acquired. For three patients, we were able to use only 11 out of 12 fiducial markers for registration
for one of the physical data acquisition.
7
Presented at SPIE Medim 2007, San Diego, CA, Feb 2007
Patient1
Days between
dental impression &
physical data
Patient2
Patient3
Patient4
Patient5
15
280
10
13
251
212
9
296
37
FRE measured
0.65
0.52
0.54
0.71
0.65
0.41
0.41
0.49
0.51
FLE
0.71
0.58
0.59
0.78
0.72
0.45
0.45
0.55
0.56
TRE measured ( BAHA )
1.91
2.56
0.89
2.67
3.77
6.26
1.78
5.34
1.77
TRE ( BAHA )
1.77
2.49
0.66
2.55
3.70
6.24
1.72
5.31
1.68
TRE FLE ( BAHA )
0.31
0.26
0.28
0.37
0.37
0.22
0.26
0.31
0.23
TRE frame ( BAHA )
1.74
2.48
0.60
2.52
3.68
6.24
1.70
5.30
1.67
TRE FLE ( cochlea )
0.24
0.20
0.18
0.24
0.24
0.14
0.16
0.20
0.18
TRE frame ( cochlea )
0.94
1.34
0.31
1.30
1.89
3.31
0.94
2.92
0.96
TRE ( cochlea )
0.97
1.35
0.36
1.32
1.90
3.31
0.95
2.93
0.98
Table 1. Root-Mean-Square Error Values. All error values are in millimeter units.
Figure 4. Plot of TRE at the cochlea versus time between the dental impression fabrication and obtaining the
physical data.
Presented at SPIE Medim 2007, San Diego, CA, Feb 2007
8
ACKNOWLEDGEMENTS
The research reported in this paper was supported by a grant from the National Institute of Biomedical Imaging and
Bioengineering, 5R21 EB002886-01. We would like to thank all the patients who participated in this validation study.
We would also like to thank Jason Mitchell for his help with the design of the fiducial frame system, Gene Edwards for
her help in scheduling the studies, and Dahl Irvin for her help with the CT scans.
REFERENCES
1. Labadie RF, Fenlon M, Devikalp H, Harris S, Galloway RL, and Fitzpatrick JM. Image-guided otologic surgery.
Computer Assisted Radiology and Congress and Exhibition (eds: Lemke HU, Vannier MW, Inamura K, Farman AG,
Doi K, Reiber JHC), Elsevier Science, 627-32, 2003.
2. Fenlon MR, Jusczyzck AS, Edwards PJ, and King AP. Locking acrylic resin dental stent for image guided surgery.
The Journal of Prosthetic Dentistry, 83(4):482-5, 2000.
3. Labadie RF, Shah RJ, Harris SS, Cetinkaya E, Haynes DS, Fenlon MR, Juszczyk AS, Galloway RL, and Fitzpatrick
JM. In vitro assessment of image-guided otologic surgery: Submillimeter accuracy within the region of the temporal
bone, Otolaryngology-Head and Neck Surgery, 132, 435-442, 2005.
4. Labadie RF, Shah RJ, Harris SS, Cetinkaya E, Haynes DS, Fenlon MR, Juscyzk AS, Galloway RL, and Fitzpatrick
JM, Submillimetric Target-Registration Error using a Novel, Non-Invasive Fiducial System for Image-Guided Otologic
Surgery, Computer Aided Surgery, 9(4), 145-153, 2004.
5. Edwards PJ, King AP, Maurer Jr. CR, De Cunha DA, Hawkes DJ, Hill DLG, Gaston RP, Fenlon MR, Jusczyzck A,
Strong AJ, Chandler CL, and Gleeson MJ. Design and Evaluation of a System for Microscope-Assisted Guided
Interventions (MAGI). IEEE Transactions on Medical Imaging 19(11): 1082-1093, 2000.
6. Fitzpatrick JM, Balachandran R, and Labadie RF, Bite-Block Relocation Error in Image-Guided Otologic Surgery,
Medical Image Computing and Computer-Assisted Intervention, 3217, 518-525, 2004.
7. Balachandran R, Labadie RF, and Fitzpatrick JM, Validation of a fiducial frame system for image-guided otologic
surgery utilizing BAHA bone screws, IEEE International Symposium on Biomedical Imaging: Macro to Nano, 2006,
518-521, 2006.
8. Wang MY, Maurer Jr. CR, Fitzpatrick JM, and Maciunas RJ. An automatic technique for finding and localizing
externally attached markers in CT and MR volume images of the head. IEEE Transactions on Biomedical Engineering,
43, 627-37, 1996.
9. Fitzpatrick JM, Hill DLG, and Maurer CR. Registration. Medical Image Processing, Volume II of the Handbook of
Medical Imaging, M. Sonka and J. M. Fitzpatrick, ed., SPIE Press. 447-513, 2000.
10. Fitzpatrick JM, West JM, and Maurer Jr. CR. Predicting error in rigid-body, point based registration. IEEE
Transactions on Medical Imaging, 17, 694-702, 1998.