Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
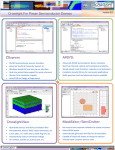
Interventional endovascular procedures simulation with patient-specific carotid arteries models generated from CTA scans Moti Freiman1, Einav Nammer2, Ofek Shilon2, Leo Joskowicz1, Jacob Sosna3 1. School of Eng. and Computer Science, The Hebrew Univ. of Jerusalem, Israel. 2. Simbionix LTD, Israel. 3. Dept of Radiology, School of Medicine, Hadassah Hebrew U, Medical Center, Israel. Purpose Minimally invasive endovascular surgeries such as carotid, coronary, and cardiac angiographic procedures are frequent in interventional radiology. They require experienced physicians and involve time-consuming trial and error with repeated contrast agent injection and X-ray imaging. This leads to outcome variability and non-negligible complication rates. Training simulators such the ANGIO MentorTM (Simbionix LTD. Israel, 2008) have the potential to significantly reduce the physicians’ learning curve, improve their performance, and reduce the outcome variability [1]. A key limitation is the simulators’ reliance on hand-tailored anatomical models generated by a technician from CTA scans, which are impractical to produce for each patient in a clinical environment. Patient specific simulation requires the segmentation of the entire vascular anatomy, including the Common Carotid Artery (CCA), the extracranial Internal Carotid Artery (ICA) and External Carotid Artery (ECA), the ECA branches, the Carotid Bifurcation (CB), the Subclavian Arteries (SA), and the Aortic Arch (AA). The vertebral arteries are desired but not required for the simulation. These vessel structures usually have a very large intra and inter-patient intensity and geometrical shape variability, are near bone structures with similar intensity values, and suffer from imaging artifacts caused by metallic objects such as dental implants. In addition, in many pathological cases, severe stenosis around the carotid bifurcation frequently causes segmentation failure [2]. Therefore the generation of patient specific models for simulation is a challenging task. Materials and Method In this study, we conducted a preliminary evaluation of the resulting segmentation models using our new method for patient-specific carotid interventional radiology simulations [3]. The method starts with the morphological-based segmentation of the aorta and the construction of a prior intensity probability distribution function for arteries. The carotid arteries are then segmented with a graph min-cut method based on a new edge weights function that adaptively couples voxel intensity, intensity prior, and geometric vesselness shape prior. Finally, the same graph-cut optimization framework is used to interactively remove a few vessel segments and to fill minor vessel discontinuities caused by intensity variations. In the study, we used a Simbionix ANGIO MentorTM (Simbionix LTD. Israel, 2008) station. The ANGIO MentorTM is an integrated software and hardware endovascular simulation platform (Fig. 1a). It simulates interventional vascular procedures based on a diagnostic CTA and a vasculature simulation model. It supports realistic haptic catheter insertion and manipulation feedback (Fig. 1b) and creates continuous fluoroscopic X-ray imaging, fluoroscopic C-arm positioning, and simulated contrast agent injection (Fig. 2a-c). For more details, see http://www.simbionix.com Four CTA datasets acquired with administrated 100cc of non-iodinated of contrast agent with a rapid injection aid at 3-4cc per sec. The CTA scans, acquired on a Sensation 16 Siemens Medical Solutions scanner (Forchheim, Germany) have in-plane pixel size 0.5x0.5mm2, matrix size 512x512, 0.55mm slice spacing, and 750 slices. The patient specific models were generated from the CTA images as follows. First, the carotid arteries systems were segmented using the nearlyautomatic method described in [3]. Next, 3D mesh with centerlines, bifurcation points, and vascular radiuses were computed with the VMTK software library automatic meshing and centerline generation modules [4]. The entire simulation model generation required less than 10 minutes for each on a standard PC, most of it computation time without interaction. Results The simulation models were then directly transferred to the Simbionix ANGIO MentorTM simulator platform. We then performed common interventional radiology procedures, such as catheter insertion and manipulation, balloon positioning and dilation, and stent placement on the patient-specific models. Fig. 2a-c shows sample snapshots of the simulation with the patientspecific models. A movie showing the simulation with http://www.cs.huji.ac.il/~freiman/vessels-cut. our 3D models is available in The simulations ran flawlessly and successfully in real time for over an hour. The users reported great realism and an excellent overall experience, which was significantly better than similar experiences with the previous manually generated models. While this simulation experiment is qualitative and preliminary, it constitutes a proof-of-concept of practical patient specific carotid interventional radiology simulations from clinical CTA scans. Conclusion We have presented a proof-of-concept of practical patient specific carotid interventional radiology simulations from clinical CTA scans. Patient specific models were generated using previously presented techniques, and used for clinical simulation successfully. Our results indicate that the generated models are accurate, robust, and provide useful information for patient specific simulation. We are currently expanding the using of patient specific models for intra-operative mode guided interventional radiology procedures. References [1] Stern, J., Zeltser, I., Pearle, M., 2007. Percutaneous renal access simulators. J. of Endourology 21 (3), 270–273. [2] Manniesing, R., Viergever, M., Niessen, W., 2007. Vessel axis tracking using topology constrained surface evolution. IEEE Trans. Med. Imaging 26 (3), 309–316. [3] Freiman, M., Broide, N., Natanzon, M., Weizman, L., Nammer, E., Shilon, O., Frank, J., Joskowicz, L., Sosna, J., 2009. Vessels-Cut: A Graph Based Approach to Patient-Specific Carotid Arteries Modeling. In: Proc. of the 2nd 3D Physiological Human workshop, 3DPH’09. Vol. 5903 of LNCS. pp. 1–12. [4] Antiga, L., Steinman, D., 2004. Robust and objective decomposition and mapping of bifurcating vessels. IEEE Trans. Med. Imaging 23 (6), 704–713, http://www.vmtk.org. (a) Simbionix ANGIO MentorTM station (b) Haptic catheter manipulation Fig. 1: (a) Simbionix ANGIO MentorTM, (b) Haptic catheter manipulation. (a) lateral view (b) AP view (c) Bifurcation with stent Fig. 2: Patient-specific simulation experiment: (a) Lateral simulated angiogram, (b) AP simulated angiogram, (c) bifurcation with stent – detail.