Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
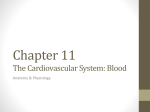
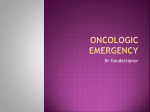
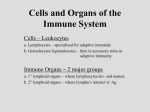
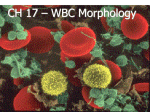
Vol. 3, 705-711, May Clinical 1997 Clinical Pharmacology of Filgrastim following Chemotherapy and Autologous Bone Marrow Transplantation’ William and P. Petros,2 William Bone Rabinowitz, Ann ited Stuart, Transplant Medical Department Program, Center, Durham, North of Medicine, Carolina Duke 27710 tial ABSTRACT namics following evaluated the of filgrastim high-dose marrow pharmacokinetics transplantation. and were developed Serum 10 patients of (tm) volume of distribution counts fusion, the 4-h receiving study periods Clearance 4-32 4-h systemic infusion group was volume. by in all during WBC 14 of severe patients recovery. The by a differential a static component WBC concentration. and one component These data suggest dosing strategies transplantation may effect equation following that marrow the of in of doses of WBCs included autologous bone Clinical the therapeutic following multiple remain therapeutic these (5625 -3), proteins and regarding their the pharmacological optimal characteristics. myeloaquestions use of A lim- characteristics of these to pharmacody- variables All as part in Review regimen bone previously marrow II-IV approved and was breast G-CSF that derived following and outlined the extinction from coefficient should product. continuous starting Escherichia 3 h after bone immediately receiving lected daily 5, 10, 1 (6). the Autolend of Amgen, Inc.). Amgen revised the doses reported to the currently was administered by either or daily 4-h infusions for 21 marrow Sampling. Single daily during the continuous infusion to day of 4, 8, 16, 32, recombinant, trial, thus, in (165 -6 after by 1.2 to be equivalent The cytokine iv. infusion or Duke cisplatin coli; of this for filgrastim; be multiplied the (day in Fig. 4 days the completion cancer by of 4 days reinfused trial bone for Clinical Trials of cyclophosphamide mg/m2), the course clinical autologous was (600 over and Board consisted filgrastim I/il of stage study carmustine as described received of a Phase chemotherapy This administered patients chemotherapy (day + I). Patients received doses or 64 pUg/kg/day of filgrastim (nonglycosylated, here to cell and ABMT, consent for the treatment mg/m2), mg/m2) mar- of link seems granulocytic METHODS Institutional The ablative Note benefits which blood or substan- chemotherapy Therapy. to high-dose marketed 14-day administering hematopoietic growth factors blative chemotherapy and ABMT;3 however, unanswered AND and University Humans. days trials have demonstrated that support human INTRODUCTION disposition, or ABMT data suggest the pharmacokinetic to evaluations melanoma. with used be suboptimal. in for volunteers following These in peripheral high-dose metastatic ogous of (1-5). describes is available to healthy the cytokine following informed and that varied that currently report following subsequent neutropenia. receiving patterns PATIENTS plasma WBC received variability to Patients immediately postinin the disappearance of on Cls was described row 197 mm, plasma then rebounded with a delay (CIs) 705 effects. Models Mean theory. on the presence increased fflgrastim infusions. clearance approximated based sag/kg/day namic colony-stimu- had interpatient related addition information its administration chemotherapy filgrastim cytokine bone colony-stimulating factor. The effect on filgrastim Cls was determined continuous infusions by segregation granulocyte concentrations patients daily filgrastim transiently fell, which correlated serum WBC granulocyte receptor-binding half-life in I study of this and autologous pharmacokinetic who recovery. This pharmacody- were determined by ELISA in continuous i.v. filgrastim infu- receiving for incorporation and during a Phase chemotherapy lating factor concentrations 21 patients receiving 14-day sions of standard-dose Research High-Dose following to patients be We amount filgrastim P. Peters Marrow University Josh Cancer administration (day +1). serum samples were obtained regimen. Samples before and after infusion were collected 4-h infusions. In addition, 15, 20, 30, 45, 60, 120, 240, from the patients samples were coland 360 mm after the completion of the 4-h infusions on day + 15. Urine was collected for 24 h after drug administration in a subset of patients receiving Received 7/8/96; revised 2/7/97; accepted 2/10/97. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. This work was supported by NIH Grant 1PO1CA47741-01A3. 2 To whom requests for reprints should be addressed, at Duke University Medical Center, Box 3961 (DUMC), Durham, NC 27710. Phone: (919) 684-6707; Fax: (919) 684-5177; E-mail: [email protected]. 3 The abbreviations used are: ABMT, autologous bone marrow transplantation; CSF, colony-stimulating factor; G-CSF, granulocyte CSF; sCr, serum creatinine. I the 4-h infusion regimen on day + 1 and day + 15. Analytic Procedure. Immunoreactive G-CSF was measured in our laboratory using a double-antibody sandwich technique (Amgen Diagnostics, Thousand Oaks, CA). Microtiter plates for were precoated G-CSF. incubated One with hundred polyclonal for 4 h at 37#{176}C. Serum anti-G-CSF jugate was rabbit p.1 of test was samples 2-h incubation tetramethylbenzidine at 37#{176}C. After was further added and were removed monoclonal antibody-horseradish added and bound to the G-CSF antibody and specific added and 100 pA of peroxidase conon the well during a washing, oxidized 100 p.1 of dilute by enzyme to 706 Filgrastim Clinical Pharmacology Day -6 -8 Cyclophosphamide (1875 mg/rn ‘/day) Cisplatin (55/mg/rn -4 Marrow 2 6 4 Infusion 8 10 12 14 16 18 20 ‘U. #{176}/day) U Fig. 1 Marrow Infusion Filgrastim 14-day Treatment administration scheme. * Infusions continuous - 64 (4 0 -2 Carrnustine (600 mg/rn) Bone from IV pg/kg/day) or 21-day four hour (4 - 64 pg/kg/day) yield a blue QD complex IV during a 30-mn room temperature incu- years, and 89% of the females bation. Addition of 100 p.1 of 0.5 N sulfuric acid stopped the reaction and yielded a yellow color. Absorbance was determined by an ELISA plate reader with a 450-nm interface filter, using eration of WBC related, with 650 con- of con- Patients nm as the centrations taming trations >25 were calculated. range G-CSF sample to minimize coefficients wavelength. in the ng/ml using the standards were reference were were diluent. always patient receiving ping a 4-h (RSTRIP sequent V.4.03; evaluations nonlinear tical model determined i.v. infusion the following using unknown conducted with values standards infusion was performed MicroMath, Salt data regression Systemic receiving City, clearance = UT). Sub- conducted using V.3.0.; Statis- drug clearance filgrastim noncompartmental equation: Lake sets were as described infusion rate/serum by con- centration. Statistical Analysis. paired analyses, nonpaired group during ory. Wilcoxon and the Mann-Whitney comparisons. Modeling continuous infusion A differential equation concentration-time approximated The data by a linear was based relating was was used U test was of clearance on pharmacokinetic This to expedite for used for changes pharmacokinetic developed. equation test thetheory relationship ported to was analysis. able for pharmacokinetic Twenty-eight purposes. The patients mean patient were WBC evalu- age was 40 those clearly found dose at doses previously (7, discernably of 64 throughout infusions less pjg/kg/day therapy. climbed steadily concentrations also Three To investigate (Fig. the acute counts effects fell 4-5 precipi- infusion the 4-h filgrastim the next of G-CSF WBC 2). following over following who had day h. Interestingly, did not decay significantly during ing 0.001 between G-CSF and WBC concentra- inverse and relation- G-CSF con- collected included due and WBC parameters for 10 individuals i.v. infusion are shown in Table at 0, to high counts 1, 2, 4, variability elimination approximating and n = following model process with best plasma volume. G-CSF Mean were concentration infusion, zero-order described parameters included volume of distribution receiv1. Only 6 h postinfusion in serum immediately A one-compartment cases. Calculated of 198 mm and 0.84, for each). The pharmacokinetic filgrastim by 4-h samples the (Fig. 2). We selected the three + 15 WBC counts of >4 X 106 cells/mi to centration postinfusion was noted in each patient (r = 0.92, and 0.93 for patients 231, 233, and 234, respectively; < and serum infusion the relationship P pa- (patients of 64 pUg/kg/day tions with linear regression analysis. A linear ship between WBC concentration postinfusion 8 and 8). hema- taken off the study drug prematurely Other clinical results have been re- Infusions. samples evaluate had at a dose counts not up accel- administration on the WBC count, seven patients counted at the same time points as the postinfusion hour hour reported made (i.e., (7, 8). in the first first as continuous tously above. RESULTS Population and lower pharmacokinetic then was response 4 pjg/kg/day response, cancer response to filgrastim pig/kg/day, only previously of breast therapeutic hematopoietic 231, 233, and 234) were due to suspected toxicity. first-order Patient 32 receiving patients was by continuous methods recovery) and of filgrastim had WBCs strip- The maximum receiving manifested the diagnosis group. Intermittent for each by curve (PCNONLIN KY). patients estimation 16, tients of the appropriate parameter 8, topoietic to the inter- and intraday for both high and low Selection and initial Lexington, in those concen- corresponding All samples obtained during continuous in the same run for individual patients of individual least-squares Consultants, appropriate and however, < 10% to eliminate any potential bias. Pharmacokinetic Analysis. pharmacokinetic to curve Unknowns densities regression, were samples. analyzed standard ng/ml. diluted intemin variation; of variation were quality control infusions were 1-25 Optical fit by linear Assays The of with study these as described input data and a in all an average half-life (t1,) (Vd) of 0.06 liter/kg, systemic exposure, as Clinical Cancer Research 707 300 -J w E C) -I C C) ID Fig. 2 Mean serum G-CSF (-) and WBC (- - - -) concentrations from seven patients following the 4-h fligrastim infusions. Concentrations were normalized to a dose of 16 pg/kg for comparison. U. (I) ID 0 0 5 4 30 100 0 200 Time Table Patient no. Dose Pharmacokinetic 1 AUC (.Lg/kg/day) param eters (p.g/mL mm) - for patients C,,. post receiving 4 hour infusion filgr astim Vd (liter/kg) (ng/mI) 300 by 4-h (minutes) v infusion (mm) t1, 400 Cls (mi/h/kg) WBCs#{176} (X l0/ml) 311 4 30.3 81.3 0.061 160.3 15.8 1.0 287 247 8 16 37.7 285.0 1 16.0 0.038 123.4 12.7 4.3 499.7 255 256 261 268 269 16 16 16 32 32 119.0 25.8 121.5 343.2 413.3 273.4 84.9 330.4 734.2 469.1 0.025 0.040 0.095 0.030 0.031 0.058 3.4 8.1 37.2 7.9 5.6 4.6 3.0 6.3 3.4 1.3 1.2 1.5 281 280 32 64 18.0 487.6 68.6 1635.1 303.3 206.6 105.9 156.7 229.8 521.1 66.4 101.4 197.5 106.9 7.9 21.0 15.3 0.5 133.5 31.7 0.171 0.019 0.057 Mean SD 0.046 a Measured on the day of pharm acokinetic measured dose; by area under however, interpatient (coefficient sidered of variation, apparent tinguish the between evaluation. curve (AUC) or C,,,, variability in clearance 151%). because These current endogenously values Continuous infusions also ance. continuous estimates infusion should be con- methods cannot produced G-CSF and concentrations with large disexog- + 1 and day G-CSF was added to urine Patients receiving continuous i.v. large interpatient variability in clear- and laboratory i.v. infusion data are shown for individuals in Table re- 2. Clearance are divided into values obtained at an early point in the regimen (day +4 to day +8) when the WBC count was cells/mm3 few days recovery in all patients of infusion (day was in progress. an equilibration patients G-CSF Infusions. manifested Pharmacokinetic ceiving <250 Known rose was analytical enously administered drug. Twenty-four-h urine samples collected on day + 15 from five patients showed that no detectable present in urine. were detectable. receiving point <64 and those + 13 to day Serum ((20% daily p.g/kg/day. G-CSF F- obtained on the final when hematopoietic concentrations reached + 15) fluctuation) However, by day patients 64 p.g/kg/day continued recovery. hematopoietic tion from ng/ml day +4 in these increased to day patients. slightly +3 The was over +8 Conversely, over tients who had therapy ifested rapidly increasing of infusion. to accumulate Median increase third this p.gfkg/day crease 20% to early by 106 cells/mI. dysfunction time period. 2). ducted Two discontinued early due G-CSF concentrations patient had her continuous 700 and three Only infusion for all patients infusion of seven one patient (total bilirubin, Three (Table of these with 2). had WBC 272) mg/dl) developed baseline patients final (patient >5.0 and did not demonstrate to 1500 of the patients three stopped on day recov- receiving The <64 median counts in- increased of > 1 X of < 1 X experienced during pa- to toxicity manbefore the end was drawn. during hematopoietic in therapy sion, whereas six patients creatinine, more than twice +4 in all from in clearance was 27% (P = 0.001). Clearance for six of seven patients with final WBC counts 106 cells/nil receiving 100%, the Cls for the other before a G-CSF serum sample Systemic clearance increased ery compared serum G-CSF before in G-CSF concentra- hepatic filgrastim infu- renal dysfunction (serum value during therapy; Table pharmacokinetic altered disposition studies compared conto 708 Filgrastim Clinical Pharmacology Table 2 Pharmacoki netic and clinical laboratory d ata for patients receivi ng filgrastim by con tinuous iv. infusion Cls (mi/h/kg) Patient Dose (p.g/kg/day) no. Change Late’ Early’ 5.95 in Cisc (%) WBC (X count” l06/ml) sCr, day 6 (mg/dl) sCr, maxe (mg/dl) 267 285 283 4 4 8 4.07 7.58 7.72 32.05 8.07 30 688 7 0.6 2.1 0.8 0.6 0.7 0.7 0.6 1.3 0.9 272 314 8 8 5.13 4.50 5.67 6.51 11 45 2.7 0.5 0.6 0.8 2.3 0.6 218 224 207 215 238 16 16 16 16 16 4.87 4.87 3.32 3.16 6.17 4.98 5.38 214 32 3.65 4.99 21 1 213 4.54 2.18 1.58 3.92 4.70 0.9 0.7 1.6 2.4 0.6 3.1 0.8 0.6 0.7 0.8 0.7 0.5 0.7 0.7 0.7 1.8 1.0 1.2 0.7 0.9 0.7 1.1 0.8 0.7 254 32 32 32 64 2 10 20 40 23 37 4 1.0 0.8 1.2 0.7 265 64 3.81 0.8 0.9 234 233 232 23 1 229 64 64 64 64 64 N/A1 3.37 4.54 3.81 1.02 0.7 0.7 1.4 1.6 246 a b C d e 3.99 4.42 7.58 56 3.40 156.86 2.56 9841 -35 9.26 70.4 0.8 143 1.4 N/A N/A N/A N/A 4.32 N/A 1.14 N/A N/A -5 N/A 12 0.7 0.8 1.4 N/A 0.8 0.9 0.6 2.4 1.7 Average values for days 4-8 of continuous infusion. Average values for days I 3-15 of continuous infusion. [Cls Late - Cls Early]/Cls Early. Final day of continuous infusion. During infusion. 1N/A, not available. 4 mcg/kg/day -1- 8 mcglkglday -*- 16 mcg/kg/day -9-- 32 mcg/kg/day -*-- 64 mcg/kg/day .0 -J Fig. 3 Median clearance of filgrastim during continuous infusion grouped by dose level. Studies were conducted before (Day 4-8) and during (Day 13-15) hematopoietic recovery (n 18). E 0 C to to 04 0 3 2 others Day4-8 with to be related cry, scribe similar WBC to dose both as shown in Fig. 3. Two pharmacodynamic the relationship (model 0) assumes Systemic and after models between during continuous infusion. eliminated by a first-order first counts. before Dayl3-15 Both process WBC were and clearance hematopoietic considered G-CSF models assume in the absence that WBC-mediated appeared recov- order. Applying the steady-state assumption in this case yields the equation: to de- C1s1*[GJ, = Dose = C1s1*[G]1 (A) + K0*WBCf, elimination that G-CSF is of WBCs. The elimination is zero- where [G] represents sents the time when refers to the clearance the concentration WBC counts of filgrastim of G-CSF were <250 in the absence and cells/mm3. i repreCls1 of significant Clinical Model Cancer Research 709 0 -J E C CD CD Fig. 4 Comparison oftwo proposed models of disposition. Model 0, plot of the change in G-CSF concentrations from beginsting to the end of infusion versus the final WBC count divided by the initial Cls as described by Eqs. A and B (r = 0.63; P < 0.001). Model 1, plot of the change in filgrastim CIs from end to beginning infusion versus the end of infusion WBC count as described in Eqs. C and D (r = 0.51; P = 0.004). -, regressions of all data, , regressions cxcluding the patient with a WBC count of 70 X 106 cells/mi (patient 246). filgrastim 0.05 Model 0.5 WBC1/C11 50 5 (ceIIs105/hr/kg) 1 2 .0 -J E 0) 0 ID 0 100 WBC1 WBC counts and is assumed to be constant. the absolute amount of G-CSF eliminated time (zero-order) in units of ng/kg/h (cells’lO#{176}/mL) The term K0 reflects by each WBC per unit per (cells X 106/ml). Parameters followed by f are those observed etic recovery. Rearranging terms yields: [G]1 The ination tion alternative of G-CSF in this case [G]f model by WBC. yields = during Applying 1) assumes WBC (B) first-order the steady-state dimassump- of G-CSF X 106/ml). (Cls1 + K1*WBCf)*[G]f, WBC by each The clearance (first-order) in the presence of is: Comparison (C) K*WBC1. = Cls1 + of the two models 4. Regression excluding patient infusion analysis 246 (highest was patient performed final (D) was determined log(Clsf Cls1) versus log(WBCf), i.e., and log([G]1 - [G]) versus log(WBC/Cls1), Eq. B) for all continuous the equation: = Dose per (cells (Cls) Fig. C1s1*[G]1 K1 is the clearance in mi/h/kg hematopoi- K0*WBCCls1. (model where WBC model by plotting 1 (from i.e., model data sets, both count Eq. D); 0 (from as shown including and clearance) in and 710 Filgrastim due Clinical Pharmacology to the large model influence of this 1 did not accurately describe 0.4); in contrast, 0.41, P model 0.02). < however, model 0 was 0.001 versus WBC elimination yielded a value if WBC r = still 0.51, In the latter set (r a significant 246 superior P 0.004). These (r both = 1 (r = 0.63, data suggest P < X l06/ml). Data from lack 0 or 1 .3 pg/kg/day. Infusion of filgrastim ABMT can toxicities and is widely used been following reduce in such recovery, settings. differences transplant patient, to the most marrow due and peripheral of this study demonstrated yond 16 pjg/kg/day did efficacy of therapy, actually slow of this ablation. data dosage cytokine higher of 64 pg/kg/day cases in the of portion based on both in vitro of an endogenous bethe seemed (7, 8). One to possible and the receptor of only a small to be internalized (1 1). Occupancy receptors on a particular biological response to provide activity, rethe a clearance to be sufficient receptor mechanism, to the cell of available beyond binding suspected immediate as was is thought noted to margmnation be (15). coincided with persisted in this have a transient for approximately time 1-h time yielded point trial accounted We concentration, in WBC reduction data (13, for by alterations that this delay in drug a re- Use at the end of infusion clearances this neutrophil in WBC elimination, 1 h postinfusion. apparent in which of multiple- and following that were on linear WBC counts reach sets. regression below be exceed the in the same WBCs have the In particular, cytokine to than saturate all per (cells X 106/ml; that in patients with hematopoietic elimination pig/kg/day, regardless of dose. is presumably first-order; there- 1.3 of G-CSF this theoretical optimum the G-CSF-receptor of to be a zero- of the sufficient 1 X 106 cells/mI, not and cells appears doses K = 54 ng/kg/h of Eq. B) implies Using (e.g., interaction 13 igfkg/day and a filgrastim pg/kg/day would be reasonable. of the clearance relationships when One filgrastim would was 2 gig/kg/day) can minimizing the while dose in the range It is important described above administered anticipate by s.c. injection; doses than those similar by continuous effects i.v. is given however, these effects found here because the may occur bioavailability at higher of the These of therapy The data chemotherapy data imply that an optimal following ilar to that investigational (regramostim) of patients by others, (1, 3, 4). Our of filgrastim to increase of the (2). We have Alternatively, an earlier dis- following which have high-dose identified between the apparent clearance of filgrastim in patients with chronic neutropenia (2) or chemotherapy the disposition would continue schedule of therapy at low occurs, quite the altogether. from this study confirm reports a direct correlation and WBC counts infusion. the cytokine of what is typically practiced today. more consideration could be made for continuation of 15-20 to realize that all were determined when is incomplete. opposite perhaps uct data would periods amount of drug eliminated by alternate mechanisms. Higher doses may be of use when the desired WBC count is >1 X 106 cells/mI. For example, if a WBC count of 1 X i0 cells/ml is desired, then hematopoietic elimination could be expected to as described infusion doses maximize others the continuous receptors. based range of values noted in both adult (5) and pediatric (3) patients following nonablative chemotherapy; however, this methodology will not allow for detailed investigation of nonlinear effects, with report lower latter by reduction available in this during of G-CSF. of G-CSF that (7, 8). igIkg/day) clearance quantities clearance suggests patients hematopoietic of G-CSF administration may entail initiation doses and titration upward as reconstitution 14). Mechanistically, noted used G-CSF to the course (>20 for patients set. lead 64 p.g/kg/day. to be detri- in three of fligrastim developing is likely patient may receiving appeared that dependent during toxicities doses limited in this maximum for full protease followed those severe suspect dose clearance appears acute effects following a filgrastim infusion on the WBC concentration have been described previously include bound, In addition, types of complex for filgrastim. The peripheral and cell is thought (12). returned fraction WBC that process near G-CSF. appears surface fact order clearance setting is not of available receptors on several the G-CSF-receptor the fore, receptors and/or responsive hematopoietic cells. The question in dose selection appears to be the number of and their precursors present, as well as the capacity of surface binding, to use only Metabolic as G-CSF critical WBCs to use potential be by on systemic would not concentrations between that of dose however, prescribed relationship evidence in vivo of filgrastim therapy in the posttransplant by the dose infused but rather by the number cells The provides such a, which may down-regulate G-CSF 10). Overall, these results suggest that G-CSF binds to cell WBCs in vitro. Following neutropema. will efficacy limited these not be routinely absolute a similar shown are complicated One in patients concentrations high have as seen drug with that of G-CSF and cytokine coinciding suggests (3). elimination serum should of degree The clinical in some effects, factor (9, cytokine sparse appropriate to the typically a dose is the stimulation necrosis expression mental, that increasing filgrastim dose not seem to significantly improve whereas for these evidence, the increasing This ABMT. Pharmacokinetic in the present study, alludes blood hematopoiesis explanation this relatively in disposition perhaps thus However, in regard chemotherapy of chemotherapy-induced or other CSFs following such as that provided to potential tumor ceptor high-dose the severity hematopoietic speed published filgrastim information, bone than both bein Fig. 3. data should concentrations, of therapy, as demonstrated These escalating G-CSF DISCUSSION have delivery of the ligand; at high greater (1) was evident as shown influence of fllgrastim concentrations to decrease humans of the latter of the potential clearance Doses and some due to s.c. drug metabolic at low Thus, of G-CSF of filgrastim reconstitution, (16) however, of knowledge steadily with animals absorption that Model elimination Dose-related clearance and after hematopoietic fore relationship; models; process. per (cells WBC then P = relationship is a zero-order cells/mI, case, = 0.05, improved to model of K0 = 54 ng/h/kg 106 point. the data patient of G-CSF 1 X ng/kg/h is 54 0 yielded Including data sigmoidal evaluated approach (Eq. C) proposes with WBC count relationship previously recombinant in patients that to describing that the clearance and thus is dissimwas postulated the pharmacokinetics granulocyte treated macrophage with exactly by of an CSF prod- the same Clinical high-dose namic noted chemotherapy regimen effect between on that trial; WBCs however, (17). A similar dysfunction during cytokine administration fusion displayed reduced drug clearance. We apparent treated study lack with of such receptor or concentrations patients who Further of studies secondary cytokine should renal of higher regramostim. of the cytokines In to detect contrast, relationship between to optimize and toxicity dosage while Sensitive results release also dysfunction is possignificant granulocyte between and specific obtained by filgrastim regimens maximizing and toxic Clinical clearance of fllgrastim therapeutic con- WBCs, and bioassays should ELISA. The role in the therapeutic be considered. should clearance, effects utilization and WBCs be of of of the may by minimizing response. help cost 1. Layton, J. E., Hockman, H., Sheridan, W. P., and Morstyn, G. Evidence for a novel in vivo control mechanism of granulopoiesis: mature cell-related control of a regulatory growth factor. Blood, 74: 1303-1307, 1989. 2. Kearns, C. M., Wang, W. C., Stute, N., lhle, J. N., and Evans, W. E. Disposition of recombinant human granulocyte-colony stimulating factor in children with severe chronic neutropenia. J. Pediatr., 123: 471479, 1993. 3. Stute, N., Santana, M., Rodman, J. H., Schell, M. J., Bile, J. N., and Evans, W. E. Pharmacokinetics of subcutaneous recombinant human granulocyte colony-stimulating factor in children. Blood, 79: 28492854, 1992. 4. Eguchi, K., Shinkai, T., Sasaki, Y., lamura, I., Ohe, Y., Nakagawa, K., Fukuda, M., Yamada, K., Kojima, A., Oshita, F., Monte, M., Suemasu, K., and Saijo, N. Subcutaneous administration of recombinant human granulocyte colony-stimulating factor (KRN86O1) in intensive chemotherapy for patients with advanced lung cancer. Jpn. J. Cancer Res., 81: 1168-1174, 1990. 5. Eguchi, K., Sasaki, S., Tamura, I., Sasaki, Y., Shinkai, T., Yamada, K., Soejima, Y., FukUda, M., Fujihara, Y., Kunitou, H., Tobinai, K., Ohtsu, I., Suemasu, K., Takaku, F., and Saijo, N. Dose escalation study of recombinant human granulocyte-colony-stimulating factor (KRN86O1) in patients with advanced malignancy. Cancer Res., 49: 5221-5224, 7. Laughlin, M. J., Kirkpatrick, 0., Sabiston, N., Peters, W., and Kurtzberg, J. Hematopoietic recovery following high-dose combined alkylating-agent chemotherapy and autologous bone marrow support in patients in phase-I clinical trials of colony-stimulating factors: G-CSF, GM-CSF, IL-l, IL-2, M-CSF. Ann. Hematol., 67: 267-276, 1993. factors and W. P., and Peters, dose intensity. W. P. Hematopoietic colony-stimulating Oncol., 20: 94-99, 1993. Semin. 9. Rabinowitz, J., Petros, W. P., Stuart, A., Rosner, G. L., Simms, I., and Peters, W. P. Effect of endogenous serum tumor necrosis factoralpha on myelopoiesis induced by recombinant, human G-CSF. Blood, 78 (Suppl. 1): 259, 1991. 10. Piacibello, W., Sanavio, F., Severino, A., Morelli, S., Vaira, A. M., Stacchini, A., and Aglietta, M. Opposite effect of tumor necrosis factor a on granulocyte colony-stimulating factor and granulocyte-macrophage colony-stimulating factor-dependent growth of normal and leukemic hemopoietic progenitors. Cancer Res., 50: 5065-5071, 1990. 11. Nicola, N. A., and Metcalf, D. Binding of differentiation-inducer, granulocyte-colony-stimulating factor, to responsive but not unresponsive leukemic cell lines. Proc. Nail. Acad. Sci. USA, 81: 3765-3769, 1984. 12. Nicola, N. A., and Metcalf, D. Binding colony-stimulating factor to normal murine REFERENCES 1989. Research 6. Peters, W. P., Ross, M., Vredenburgh, J. J., Meisenberg, B., Marks, L. B., Winer, E., Kurtzberg, J., Bast, R. C., Jones R., Shpall, E., Wu, K., Rosner, G., Gilbert, C., Mathias, B., Coniglio, D., Petros, W., Henderson, C., Norton, L., Weiss, R., and Hurd, D. High-dose chemotherapy and autologous bone marrow support as consolidation after standard-dose adjuvant therapy for high-risk primary breast cancer. J. Clin. Oncol., 11: 1132-1143, 1993. 8. Petros, (17). pharmacokinetics filgrastim the relationship appropriate dosing. used to substantiate filgrastim G-CSF. on the current a relatively with not able inthe was excreted in the urine of patients following and the extent of such excretion was less in experienced to monitor of either handling we were was renal via continuous postulate that compared renal because macrophage CSF its administration, in patients be a result availability dissimilar especially urinary tinue may affinity Alternatively, sible, effects filgrastim pharmacody- and apparent drug clearance patients who experienced Cancer Physiol., 124: 313-321, 13. Morstyn, of ‘I-labeled hemopoietic granulocyte cells. J. Cell. 1985. G., Campbell, L., Lieschke, G., Layton, J. E., Maher, D., O’Connor, M., Green, M., Sheridan, W., Vincent, M., Alton, K., Souza, L., McGrath, K., and Fox, R. M. Treatment of chemotherapy-induced neutropenia by subcutaneously administered granulocyte colony-stimulating factor with optimization of dose and duration of therapy. J. Clin. Oncol., 7: 1554-1562, 1989. 14. Bronchud, M. H., Potter, M. R., Morgenstern, G., Blasco, M. J., Scarffe, J. H., Thatcher, N., Crowther, D., Souza, L. M., Alton, N. K., and lesta, N. G. In vitro and in vivo analysis of the effects of recombinant human granulocyte colony-stimulating factor in patients. Br. J. Cancer, 58: 64-69, 1988. 15. Okada, Y., Kawagishi, M., and Kusaka, M. Neutrophil kinetics of recombinant human granulocyte colony-stimulating factor-induced neutropenia in rats. Life Sci., 47: 65-70, 1990. 16. Tanaka, H., and Kaneko, T. Pharmacokinetics of recombinant human granulocyte colony-stimulating factor in the rat: single and multiple dosing studies. Drug Metab. Dispos., 19: 200-204, 1991. 17. Petros, W. P., Rabinowitz, J., Stuart, A. R., Gilbert, C. J., Kanakura, Y., Griffin, J. D., and Peters, W. P. Disposition of recombinant human granulocyte-macrophage colony-stimulating factor in patients receiving high-dose chemotherapy and autologous bone marrow support. Blood, 80: 1135-1140, 1992. 711