Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
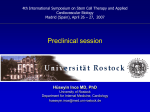
[CANCER RESEARCH 58. 794-800. February 15. I998| Expression of Granulocyte Colony-stimulating Factor Receptor Correlates with Prognosis in Oral and Mesopharyngeal Carcinoma1 Hideaki Tsuzuki, Shigeharu Fujieda,2 Hiroshi Sunaga, Ichiro Noda, and Hitoshi Saito Department of Otarhinoluryngolagy. Fukui Medical University, Matsuoka-cho, Yashida-gun, Fukui 910-11. Japan ABSTRACT Granulocyte colony-stimulating factor receptors (G-CSFRs) have been observed on the surface of not only hematopoietic cells but also several cancer cells. The stimulation of G-CSF has been demonstrated to induce proliferation and activation of G-CSFR-positive cells. In this study, we investigated the expression of G-CSFR on the surface of tumor cells and G-CSF production in oral and mesopharyngeal squamous cell carcinoma (SCO by an immunohistochemical approach. Of 58 oral and mesopharyngeal SCCs, 31 cases (53.4%) and 36 cases (62.1%) were positive for G-CSFR and G-CSF, respectively. There was no association between G-CSFR expression and G-CSF staining. In the group positive for G-CSFR expression, relapse was significantly more likely after primary treatment (/' = 0.0069), whereas there was no association between G-CSFR expression and age, sex, tumor size, lymph node metastasis, and clinical stage. Also, the G-CSFR-positive groups had a significantly lower disease-free and overall survival rate than the G-CSFR-negative groups i/' = 0.0172 and 0.0188, respec tively). However, none of the clinical markers correlated significantly with G-CSF staining, nor did the status of G-CSF production influence the overall survival. The results imply that assessment of G-CSFR may prove valuable in selecting patients with oral and mesopharyngeal SCC for aggressive therapy. INTRODUCTION G-CSF,1 a glycoprotein growth factor, regulates the proliferation and differentiation of granulocytic progenitor cells and functionally activated mature neutrophils (1-3). Cells stimulated by G-CSF (espe cially neutrophils) play an important role in the local host defense response to infection or inflammatory disorders through their phago cytosis, chemotaxis. and microbicidal activities (4, 5). However, a recent study showed that the effect of G-CSF was not limited to bone marrow cells or to hematopoietic deviation. Several malignant tumors, including hepatocarcinoma (6), bladder carcinoma (7), SCC of the oral cavity (8, 9), and malignant mesothelioma (10), have been dem onstrated to secrete large amounts of G-CSF. Various effects of G-CSF are triggered by the binding of G-CSF to its receptor on the surface of the cells (11-17). Not only hematopoietic cells but also several cancer cells, including colon adenocarcinoma (18), small cell lung carcinoma (19), and bladder carcinoma (20, 21), have functional receptors for G-CSF and stimulation via G-CSFRinduced proliferation of tumor cells. Autocrine growth of transitional cell carcinoma of the bladder by G-CSF has been demonstrated, suggesting that G-CSF-producing cancers with G-CSFR would have a poor prognosis (21). In this study, we investigated the expression of G-CSFR on the surface of tumor cells and G-CSF production in oral and mesopha ryngeal SCC by using an immunohistochemical approach. Also, we analyzed the correlation between clinicopathological factors of the patient and expression of G-CSFR or G-CSF production. MATERIALS AND METHODS Patients and Sample Collection. We studied 58 patients with oral and mesopharyngeal SCC who had undergone tumor-curative resections in the Department of Otorhinolaryngology, Fukui Medical University from 1984 to 1996. The mean age of the patients was 63.5 years (median age, 65.0 years). According to the general rules for head and neck cancer (tumor-node-metas tasis classification), they were classified as 7 stage I cases (12%), 11 stage II cases (19%), 13 stage III cases (22%), and 27 stage IV cases (47%). Seventy percent of the patients (41 cases) were followed-up for 5 years, and the rest were followed-up for at least I year. Ten patients died from other diseases. None of the patients had been treated with either chemotherapy or irradiation therapy before the surgery. Patients with oral and mesopharyngeal SCC had been treated with standard therapy based on the disease stage. Briefly, patients at stages I and II underwent only tumor resection, whereas those at stages III and IV underwent tumor resection, standard neck dissection, and irradiation (60 Gy) after surgery. One doctor (H. Sa.) conducted all of the surgeries. Surgically resected SCC tissues were quickly fixed in 10% buffered formal dehyde for 24 h and embedded in paraffin. Immunohistochemical Staining. Immunohistochemical staining was performed to detect G-CSFR and G-CSF in SCC tissues using the tradi tional avidin-biotin-peroxidase complex technique. Paraffin-embedded blocks were cut to 5-/¿m-thickspecimens and deparaffinized by ethanol. After washing in distilled water and rinsing with PBS (pH 7.4), inhibition of endogenous peroxidase activity was accomplished by incubation in 0.3% H,O; solution dissolved in absolute methanol at room temperature for 15 min. All specimens were washed in distilled water, rinsed with PBS, and incubated with normal sheep serum (DAKO LSAB kit; DAKO, CarpinterÃ-a, CA) for 5 min at room temperature to block the background absorption of antiserum; then they were incubated with mouse antihuman G-CSFR mAb (LMM741 clone; PharMingen, San Diego, CA; diluted 1:50: G-CSFR mAb. Ref. 16) or rabbit anti-rG-CSF polyclonal Ab (Chugai Pharmaceu tical Co., Tokyo, Japan; diluted 1:200; aG-CSF Ab) at 4°Covernight. All specimens were treated with goat antimouse biotinylated IgG (DAKO) or goat antirabbit biotinylated IgG. Specimens were then rinsed with PBS and allowed to react with the avidin-biotin-peroxidase complex for 40 min at room temperature. After rinsing with PBS, peroxidase color visualization was carried out with 3,3'-diaminobenzidine tetrahydrochloride solution (DAB; Dojin, Kumamoto, Japan; 30 mg dissolved in 150 ml of PBS and added to 10 fil of 30% HjO, solution). Before staining with aG-CSF Ab, specimens were subjected to microwave irradiation for 10 min in distilled water to enhance immunohistochemical staining (22). Nuclear counterstaining was carried out with Harris hematoxylin for 30 s before mounting. Evaluation of Specimens. Formicroscopeanalysisof G-CSFRandG-CSF staining, we selected 5 high-powered fields, with each field containing more than 200 tumor cells, and counted both the number of positive and the total number of cancer cells. In total, at least 1000 tumor cells were counted. We calculated the average of 10 readings showing the percentage of G-CSFR- or G-CSF-positive cells and expressed them as the G-CSFR score or the G-CSF score, respectively. Both G-CSFR and G-CSF stainings were scored independ ently by two doctors (H. T. and H. Su.) in a coded manner (without knowledge of the clinical parameters and outcomes). The plus (+ ) shows that over 20% of the tumor cells were positive. Infiltrating neutrophils in the section were used as a positive control of the stain for the G-CSFR mAb, and mouse IgG or Received 8/25/97; accepted 12/19/97. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1 Supported in part by Grant-in-Aid 07457397 (to H. Sa.) from the Ministry of Education, Science, Sports and Culture, Japan. : To whom requests for reprints should be addressed. Phone: 81-776-61-3111, exten sion 2398; Fax: 81-776-61-8118; E-mail: [email protected]. 1 The abbreviations used are: G-CSF, granulocyte colony-stimulating factor; G-CSFR, G-CSF receptor; ru-CSF, recombinant G-CSF; SCC. squamous cell carcinoma; mAb, monoclonal antibody: Ab. antibody; HGF. hepatocyle growth factor; CSF-1, macrophage colony-stimulating factor. 794 Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1998 American Association for Cancer Research. G-CSFR AND PROGNOSIS *£ B Fig. 1. H&E staining (A) and immunohistochemical staining of G-CSFR (ß)in a G-CSFRpositive oral SCC. Cytoplasmic and plasma mem branes of the tumor cells were positively stained (G-CSFR score, 95%; X200). H&E staining (O and lack of G-CSFR staining (D; G-CSFR score, 5%| in a different oral SCC than that shown in A. Infiltrating neutrophils (E) served as a positive con trol for G-CSFR staining (X2000). • c rabbit serum was used as a negative control instead of primary Ab for G-CSFR or G-CSF, respectively. survival rate of the patients was determined and plotted according to the Kaplan-Meier test. The Macintosh personal computer system (Stat View Statistical Analyses. The clinical characteristics of the patients in relation to G-CSFR and G-CSF were analyzed by log-rank (Mantel-Cox) tests. The software; Abacus Concepts, Inc., Berkeley, CA) was used for all statistical analyses. 795 Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1998 American Association for Cancer Research. G-CSFR AND PROGNOSIS Fig. 2. A, H&E staining of cancerous and noncancerous areas in oral SCC. B and D, noncancerous areas; C and £,cancerous areas. Noncancerous area B was negative for G-CSFR. Cancerous area C was positively stained for G-CSFR (G-CSFR score, 53%; X200). Noncancerous area D was positive for G-CSF. Cancerous area £was also positively stained for G-CSF (G-CSF score, 78%; X200). RESULTS 1.0 Expression of G-CSFR Correlated Significantly with the Prog nosis. Using G-CSFR mAb, 58 formalin-fixed paraffin-embedded oral and mesopharyngeal > SCC specimens were stained with standard h-- - - G-CSFR (-) (+) 0.8 3 l £ 0.6 Table 1 Association betH-een clinicopathological factors and expression of G-CSFR 0.4 0.2 (nNo.61.8 31)%506050486057555257553859574373387841groupingNegative 27)%504050524043454843456241435727622159P0.38490.46800.88240.79240.663 (nNo.64.8 0 • 0 SD)GenderMaleFemaleTumor Age (mean ± 12.81912411)98161546516(primary)25619121516G-CSFR= ± 13.11984M66131435811198720423= ± 10 20 30 40 50 60 Months B sizeTlT2T3T4Lymph LO w 0.8metastasisPositiveNegativeClinical node I - - G-CSFR (-) (+) 0.6- U) stageI11111IVPostoperative I 0.4 10.36170.00690.0066 O 0.2 treatmentIrradiationNoneRecurrenceYesNoDeath 0 10 20 30 40 50 60 Months diseaseYesNoPositive from Fig. 3. Disease-free survival curves (A) and overall survival curves (B) for patients with oral and mesopharyngeal SCC. The disease-free survival and overall survival of 31 patients with G-CSFR-positive cancer cells were significantly shorter than those of 27 patients with G-CSFR-negative tumors (/> = 0.0172 and 0.0188, respectively). 796 Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1998 American Association for Cancer Research. O-CSFR AND PROGNOSIS Fig. 4. H&E staining (.Aland immunnhistochemical staining of G-CSF (B) in a G-CSF-positive oral SC'C. In the cytoplasm and plasma membrane »Ithe iunior trii, immunoreaclivity for G-CSF was observed (G-CSF score, 90%; X200). H&E staining (O and lack of G-CSF staining (O) (G-CSF score, 7%; X200) in a different oral SCC than that shown in A. and noncancerous areas. Cancer cells were positive for G-CSFR staining (G-CSFR score, 53%; Fig. 1C). However, noncancerous areas were negative (Fig. IB}. Nine percent of these samples (3 of 33) showed positive staining for G-CSFR in the normal adjacent area. Both normal squamous epithelium and fibroblast were positively stained. The association between clinical factors and expression of G-CSFR is shown in Table 1. There was no association between G-CSFR expression and age, sex, tumor size, lymph node metastasis, or clinical stage. The G-CSFR score did not correlate with these five clinical factors (data not shown). ABC methods. Cytoplasm and plasma membrane of tumor cells were positively stained (Fig. 1, A and B), but partial heterogeneity of staining was observed in each of these cases. The mean G-CSFR score in this study was 41.9 ± 37.5% (mean ± SD; median, 27.9%). Positive expression of G-CSFR, ranging from 25.1-100% with a mean ±SD of 72.8 ±22.6%, was found in 31 of 58 cases (53.4%). A specimen of oral SCC demonstrated to be negative for G-CSFR staining is shown in Fig. 1, C and D. Neutrophils that had infiltrated the section stained positive for G-CSFR in all specimens (Fig. IE). Thirty-three of 58 samples had histologically normal adjacent tissue. The specimen of oral SCC shown in Fig. 2A included both cancerous 797 Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1998 American Association for Cancer Research. G-CSFR AND PROGNOSIS G-CSFR expression was significantly associated with recurrence of the disease (P = 0.0069). In 26 of 58 patients, primary cancer treatment failed. Nineteen of these 26 patients with recurrence (73%) had G-CSFR-positive tumors, whereas the remaining 7 (27%) had G-CSFR-negative tumors. In the patients with recurrent disease, the average G-CSFR score was 55.2 ±35.3%, whereas in patients with out recurrence, it was 31.0 ±36.2% (P = 0.0134). Seventeen of 26 patients with recurrence were examined again for G-CSFR expression at the time of recurrence. Eleven of 17 cases (64%) stained positively both times (initial and recurrent). Ten of these patients died of the disease. Three cases (18%) that did not stain for G-CSFR initially were found to have become positive for G-CSFR expression at the time of recurrence. All three patients died of the disease. Two cases (12%) that initially stained positive for G-CSFR were later negative for G-CSFR staining; one of these patients is alive. Only one patient (6%) showed no expression of G-CSFR at the initial and recurrent times, and this patient is still alive. Also, a significant association was found between G-CSFR expres sion and the number of deaths from the disease. Nineteen patients died of the disease in this series of patients, and 15 of these 19 patients (78%) had G-CSFR-positive cancer cells (P = 0.0066). The average G-CSFR score of patients who died of the disease was significantly higher than that of well-controlled patients (56.2 ± 35.5 versus 34.9 ±36.8%, mean ±SD; P = 0.0412). Fig. 3 shows disease-free and overall survival curves stratified by G-CSFR status. The disease-free and overall survival rates of both G-CSFR-positive and -negative groups were calculated using the Kaplan-Meier method. There was a significant difference in the dis ease-free survival rate in favor of the G-CSFR-negative groups (P = 0.0172; Fig. 3A). There was also a significant difference in the overall survival rate between G-CSFR-positive and -negative groups (P = 0.0188; Fig. 3ß). Although 72.8% of the G-CSFR-negative group survived 5 years, only 44.0% of G-CSFR-positive patients survived for that period. The administration of rG-CSF to patients seems to be an important factor in the contribution of G-CSFR to survival. A total of two Table 2 Clinicopathological features of the study population in relation to C-CSF staining =No.63.6 (n =No.62.5 (n Table 3 Muli/variate factorsGender Prognostic Cox proportional hazard analysis CI"0.43-2.890.72-5.740.96-7.731.04-10.180.54-4 ratio1.1122.0292.7193.2581.54195% male)Tumor (female or T^/T4)Lymph size (T!/T2 or +)G-CSFR node metastasis (—or +)G-CSF (- or (- or +)Hazards 1 CI, confidence interval. patients were treated with rG-CSF for the leukocytopenia induced by chemotherapy. In one of these patients, the recurrent tumor positively expressed G-CSFR, whereas in the other, there was no expression of G-CSFR. No Correlation of G-CSF Staining with the Prognosis. The same 58 oral and mesopharyngeal SCC specimens that were examined for G-CSFR expression were also stained with aG-CSF Ab (Fig. 4). The mean G-CSF score was 53.5 ±35.6% (mean ±SD; median, 62.9%). Thirty-six cases (62%) were found to have a G-CSF score of more than 20% (from 23.0-100%) and determined to stain positively for G-CSF. The clinicopathological features of the study population in relation to G-CSF staining of cancer cells are shown in Table 2. None of the clinical markers correlated significantly with G-CSF staining or G-CSF score (data not shown). The Kaplan-Meier analysis showed that there was no difference in the status of G-CSF staining (P = 0.7735). The survival rate for 5 years was 54.9 and 60.8% in the positive and negative group for G-CSF staining, respectively. Association of G-CSFR Expression and G-CSF Staining. The association of G-CSFR expression and G-CSF staining in the tumor area was examined. Twenty-one specimens (36%) stained positively for both G-CSFR and G-CSF, 10 cases (17%) were G-CSFR positive and G-CSF negative, 15 cases (26%) were G-CSFR negative and G-CSF positive, and 12 cases (21%) were both G-CSFR and G-CSF negative. No significant association between G-CSFR expression and G-CSF staining was found by the x2 test (P = 0.3400). In addition, no correlation was found between the G-CSFR and the G-CSF score using the Spearman rank correlation coefficient test (r = 0.245; P = 0.067). We also evaluated G-CSF staining in the tissue surround ing the cancer cells. The areas shown in Fig. 2, D and E, are the same as those in Fig. 2, B and C, respectively. Because both cancerous and noncancerous areas stained positively for G-CSF (Fig. 2, D and E), 49 of 58 samples (84%) showed some positive G-CSF staining of normal No signif icant relationship was found between G-CSFR expression in cancer cells and the G-CSF status of the whole section, including adjacent 9.31573676148324131931012715= ± SD)GenderMaleFemaleTumor Age (mean ± 14.8231351588152149914(primary)251116201224G-CSF36)%61656371535752725782M52577862636362stainingNegative ± tissue, using the x2 test (P = 0.8503). si/eTlT2T3T4Lymph metastasisPositiveNegativeClinical node stageIIIIIIIVPostoperative treatmentIrradiationNoneRecurrenceYesNoDeath 22)%393537294743482843183148432138373738P0.75690.73860.70260.10440.33740.14400.94020.9050 squamous epithelium and fibroblast in the adjacent tissue. Next, we focused on the 19 patients who died from disease and the association between G-CSFR and total G-CSF staining. Six of 15 G-CSFR-positive patients (40%) were negative for G-CSF, whereas 3 of 4 G-CSFR-negative patients (75%) were G-CSF positive. These results indicate that G-CSFR expression on the tumor cells is com pletely independent of G-CSF status in cancer tissue. Relative Risks Contributing to Survival Time. The prognostic value of G-CSFR expression was examined by multivariate analysis using the Cox proportional hazard model. G-CSFR expression was significant as an independent prognostic indicator for overall survival, followed by lymph node metastasis (Table 3). The risk ratio of death was 3.258 among patients who were G-CSFR positive versus those who were G-CSFR negative (P = 0.0422). DISCUSSION diseaseYesNoPositive from In this study, we demonstrated that there was a significant associ ation between G-CSFR expression in cancer cells and a poor prog- 798 Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1998 American Association for Cancer Research. G-CSFR AND PROGNOSIS nosis in patients with oral and mesopharyngeal SCC. Expression of G-CSFR is also associated with a possibility for relapse of the disease, although the physiological functions of G-CSFR on the surface of patients with carcinoma expressing G-CSFR, we feel that care should be taken in the clinical use of rG-CSF in patients with G-CSFRpositive cancer. The expression of G-CSFR in oral and mesopharyn cancer cells remains unclear. G-CSFR expression has been frequently observed not only in cancer cell lines (18-20) but also on human transitional carcinoma cells of the bladder (21, 23). G-CSFR-positive cancer cells derived from a clinical specimen have been shown to proliferate in vitro by spontaneous G-CSF production by cancer cells or by the addition of exogenous G-CSF. This proliferation was blocked by anti-G-CSF Ab (21, 23). These results suggest that G-CSF and its receptor act as a paracrine and/or autocrine loop mechanism for the proliferation of tumor cells. This concept was demonstrated by a gene transfection model in which a human osteosarcoma cell line transfected by retroviral infection to produce human G-CSF became autostimulatory in vitro and grew easily in vivo (24). However, we showed that there was no association between G-CSFR expression and G-CSF production in geal SCC may be a prognostic factor, and effective measures includ ing aggressive therapy against the disease after primary surgery should be considered. ACKNOWLEDGMENTS We thank Drs. T. Saito, G. Tsuda, N. Tanaka, C. Sugimoto, M. Seki, T. Ito, and S. Noriki for their critical review of this work. We also thank Kyowa Hakko Kogyo Co. Ltd. and Chugai Pharmaceutical Co. Ltd. for supplying the Abs. REFERENCES 1. Nicola, N. A., and Metcalf, D. Binding of the differentiation inducer, granulocytecolony-stimulating factor, to responsive but noi unresponsive leukemic cell lines. Proc. Nati. Acad. Sci. USA, 81: 3765-3769, 1984. 2. Nicola, N. A.. Begley, C. G., and Metcalf, D. Identification of the human analogue of a regulator that induces differentiation in murine leukaemic cells. Nature (Lond.), 314: 625-628. 1985. 3. Weite. K., Platzer. E., Lu, L., Gabrilove, J. L„Levi, E., Mertelsmann, R., and Moore, M. A. S. Purification and biochemical characterization of human pluripotent hematopoietic colony-stimulating factor. Proc. Nati. Acad. Sci. USA, 82: 1526-1530. 1985. 4. Asano. S. Human granulocyte colony-stimulating factor: its basic aspects and clinical applications. Am. J. Pediatr. Hematol. Oncol.. 13: 400-413, 1991. 5. Demetri, G. D., and Griffin. J. D. Granulocyte colony-stimulating factor and its receptor. Blood, 78: 2791-2808, 1991. 6. Gabrilove, J. L.. Weite, K., Lu, L., Castro-Malaspina, H., and Moore. M. A. S. Constitutive production of leukemia differentiation, colony-stimulating, erythroid burst-promoting, and pluripoietic factors by a human hepatoma cell line: character ization of the leukemia differentiation factor. Blood, 66: 407-415. 1985. 7. Souza. L. M., Boone, T. C., Gabrilove, J., Lai. P. H., Zsebo, K. M.. Murdock, D. C., Chazin, V. R., Bruszewski, J., Lu. H., Chen. K. K.. Barendt. J., Platzer. E., Moore, M. A. S., Mertelsmann, R., and Weite, K. Recombinant human granulocyte colonystimulating factor: effects on normal and leukemic myeloid cells. Science (Washing ton DC), 232: 61-65, 1986. 8. Nagata, S., Tsuchiya, M., Asano, S.. Kaziro. Y.. Yamazaki. T., Yamamoto, O., Mirata, Y., Kubota, N.. Oheda, M.. Nomura, H., and Ono, M. Molecular cloning and expression of cDNA for human granulocyte colony-stimulating factor. Nature (Lond.), 319: 415-418, 1986. 9. Tsukuda. M., Nagahara, T., Yago. T., Matsuda. H., and Yanoma, S. Production of granulocyte colony-stimulating factor by head and neck carcinomas. Biotherapy (Tokyo). 6: 183-187. 1993. 10. Demetri. G. D.. Zenzie, B. W.. Rheinwald. J. G., and Griffin J. D. Expression of colony-stimulating factor genes by normal human mesothelial cells and human malignant mesothelioma cells lines in viiro. Blood, 74: 940-946, 1989. 11. Fukunaga, R.. Seto, Y., Mizushima, S., and Nagata. S. Three different mRNAs encoding human granulocyte colony-stimulating factor receptor. Proc. Nail. Acad. Sci. USA, 87: 8702-8706. 1990. 12. Fukunaga. R.. Ishizaka-Ikeda, E., Pan, C-X., Seto, Y., and Nagata. S. Functional domains of the granulocyte colony-stimulating factor receptor. EMBO J., 10: 28552865, 1991. 13. Fukunaga, R.. Ishizaka-Ikeda. I . and Nagata. S. Growth and differentiation signals mediated by different regions in the cytoplasmic domain of granulocyte colonystimulating factor receptor. Cell. 74: 1079-1087. 1993. 14. Ziegler, S. F., Bird, T. A., Morella, K. K.. Mosley, B., Gearing, D. P., and Baumann, H. Distinct regions of the human granulocyte-colony-stimulating factor receptor cytoplasmic domain are required for proliferation and gene induction. Mol. Cell. Biol., 13: 2384-2390, 1993. 15. Dong, F., Buitenen. C. V., Pouwels, K., Hoefsloot, L. H.. Löwenberg, B., and Touw, I. P. Distinct cytoplasmic regions of the human granulocyte colony-stimulating factor receptor involved in induction of proliferation and maturation. Mol. Cell. Biol., 13: 7774-7781. 1993. 16. Nicholson, S. E., Dates, A. C., Harpur, A. G.. Ziemiecki, A.. Wilks, A. F.. and Layton, J. E. Tyrosine kinase JAM is associated with the granulocyte-colony-stimulating factor receptor and both become tyrosine-phosphorylated after receptor activation. Proc. Nati. Acad. Sci. USA, 91: 2985-2988. 1994. 17. El-Sonbaty, S. S., Watanabe. M., Hochito. K., Yamaguchi. K.. Matsuda, I., and Tsuchiya, H. Exogenously expressed granulocyte colony-stimulating factor (G-CSF) receptor on K562 cells can transduce G-CSF-triggered growth and differentiation signals. Int. J. Hematol., 61: 61-68, 1995. 18. Berdel, W. E., Denhauser-Riedl. S., Steinhauser, G., and Winton, E. F. Various human hematopoietic growth factors (interleukin-3, GM-CSF, G-CSF) stimulate clonal growth of nonhematopoietic tumor cells. Blood, 73: 80-83. 1989. 19. Avalos, B. R., Gasson, J. C., Hedvat, C., Quan. S. G.. Baldwin, G. C.. Weisbart. R. H.. Williams. R. E.. Golde, D. W., and DiPersio, J. F. Human granulocyte colonystimulating factor: biological activities and receptor characterization on hematopoietic cells and small cell lung cancer cell lines. Blood, 75: 851-857, 1990. oral mesopharyngeal SCC, suggesting that cancer cells do not neces sarily produce G-CSF by themselves. G-CSF is usually produced by normal fibroblasts and tissue adjacent to the cancer (25, 26). Actually, the serum levels of endogenous G-CSF were significantly elevated in patients with lung cancer compared with healthy people (27). Exog enous G-CSF immediately up-regulated G-CSFR expression in leu kemia cells (28). Studies of whether G-CSF stimulates proliferation and enhances the expression of G-CSFR in oral and mesopharyngeal carcinoma cells are under way. Human G-CSFR has five isoforms differing in the cytoplasmic domain, arising from alternative RNA splicing (11, 29, 30). The membrane-bound receptor isoforms are speculated to differentially regulate proliferative and other signals (i.e., mature signals; Ref. 30). A portion of the cytoplasmic domain of G-CSFR has been demon strated to be indispensable to the transduction of the G-CSF signal (12). A point mutation in the region coding for the cytoplasmic domain of the G-CSFR gene was shown to be involved in a reduced or abnormal response to G-CSF (31). Thus, we speculate that the signal via G-CSFR has functions other than proliferation in oral and mesopharyngeal SCC. The most likely function of the G-CSFR signal is enhancement of cancer cell invasiveness. Several growth factors, CSF-1, transforming growth factor ß,epidermal growth factor, HGF, and basic fibroblast growth factor, enhanced the invasiveness and metastatic activity of cancer cells (32-43). In the invasive model, CSF-1 and HGF require CSF-1 receptor and HGF receptor to function on the surface of cancer cells, respectively (32, 35, 40). The expres sion of CSF-1 receptor has been associated with adverse clinicopathological prognostic variables in ovarian carcinoma (32). We have evidence that exogenous G-CSF enhanced the invasive potential of head and neck SCC cell lines through the elevation of metalloproteinase produced by cancer cells (44).4 Also, G-CSF promoted inva sion by lung cancer cell lines (45). Thus, we hypothesize that the poor prognosis of G-CSFR-positive cancer patients results mainly from enhanced invasiveness triggered via the G-CSFR signal. rG-CSF is being used more and more frequently to treat patients with head and neck cancer after chemotherapy in an attempt to reduce bacterial/fungal infections during neutropenia and/or to administer high-dose chemotherapy (4, 5). The present study provides evidence that the poor prognosis of patients with oral and mesopharyngeal carcinoma is related to the expression of G-CSFR on the surface of cancer cells. Although we have no data as of yet to determine whether exogenous G-CSF induces tumor cell proliferation in vivo in the 4 I. Noda. S. Fujieda, H. Tsuzuki. H. Sunaga. N. Tanaka. T. Otsubo, and H. Saito. G-CSF enhances the invasive potential of human head and neck carcinoma cell lines, submitted for publication. 799 Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1998 American Association for Cancer Research. O-CSFR AND PROGNOSIS 20. Ohigashi, T.. Tachihana. M., Tazaki. H., and Nakamura. K. Bladder cancer cells express functional receptors for granulocyte-colony stimulating factor. J. Urol.. 147: 283-286. 1992. 21. Tachibana. M.. Miyakawa. A., Tazaki. H., Nakamura. K.. Kubo, A., Hata, J-l., Nishi, T., and Amano. Y. Autocrine growth of transitional cell carcinoma of the bladder induced by granulocyte-colony stimulating factor. Cancer Res., 55: 3438-3443, 1995. 22. Shi. S-R., Key, M. E., and Kalra, K. L. Antigen retrieval in formalin-fixed, paraffinembedded tissues: an enhancement method for immunohistochemical staining based on microwave oven heating of tissue sections. J. Histochem. Cytochem., 39: 741-748, 1991. 23. Tachibana. M., Miyakawa. A.. Uchida, A., Murai, M., Eguchi. K., Nakamura. K.. Rubo. A., and Hata, J-I. Granulocyte colony-stimulating factor receptor expression on human transitional cell carcinoma of the bladder. Br. J. Cancer. 75. 1489-1496. 1997. 24. Thacker. J. D.. Dedhar, S., and Hogge. D. E. The effect of GM-CSF and G-CSF on the growth of human osteosarcoma cells in vitro and in vivo. Int. J. Cancer. 56: 236-243. 1994. 25. Kaushansky. K., Lin, N.. and Adamson, J. W. Interleukin 1 stimulates fibroblasts to synthesize granulocyte-macrophage and granulocyte colony-stimulating factors. J. Clin. Invest., 81: 92-97, 1988. 26. Vancheri, C, Ohtoshi. T., Cox, G., Xaubet, A., Abrams, J. S., Gauldie, J.. Dolovich. J., Denburg, J.. and Jordana. M. Neutrophilic differentiation induced by human upper airway fibroblast-derived granulocyte/macrophage colony-stimulating factor (GMCSF). Am. J. Respir. Cell Mol. Biol.. 4: 11-17. 1991. 27. Kat.sumata. N.. Eguchi, K., Fukuda, M., Vaniamolo, N.. Ohe, Y.. Oshita. F., Tamura, T.. Shinkai. T.. and Saijo, N. Serum levels of cytokines in patients with untreated primary lung cancer. Clin. Cancer Res., 2: 553-559, 1996. 28. Steinman, R. A., and Tweardy. D. J. Granulocyte colony-stimulating factor receptor mRNA up-regulation is an immediate early marker of myeloid differentiation and exhibits dysfunctional regulation on leukemic cells. Blood. 83: 119-127, 1994. 29. Larsen, A., Davis, T.. Curtis. B. M.. Gimpel. S.. Sims. J. E.. Cosman. D., Park. L., Sorensen. E.. March. C. J.. and Smith. C. A. Expression cloning of a human granulocyte colony-stimulating factor receptor: a structural mosaic of hematopoietin receptor, immunoglobulin, and fibronectin domains. J. Exp. Med.. 772: 1559-1570, 1990. 30. Avalos. B. R. Molecular analysis of the granulocyte colony-stimulating factor recep tor. Blood, 88: 761-777, 1996. 31. Dong. F.. Brynes, R. K.. Tidow. N.. Welle, K., Löwenberg. B., and Touw, I. P. Mutations in the gene for the granulocyte colony-stimulating-factor receptor in patients with acute myeloid leukemia preceded by severe congenital neutropenia. N. Engl. J. Med.. 333: 487-493, 1995. 32. Kacinski, B. M., Carter. D.. Mittal, K., Yee, L. D., Scala, K. A.. Donofrio, L., Chambers, S. K., Wang. K-I., Yang-Feng, T., Rohrschneider. L. R., and Rothwell. V. M. Ovarian adenocarcinomas express fms-complementary transcripts and fms antigen, often with coexpression of CSF-1. Am. J. Pathol.. 137: 135-147. 1990. 33. Filderman. A. E., Bruckner, A.. Kacinski. B. M.. Deng, N., and Remold. H. G. Macrophage colony-stimulating factor (CSF-1) enhances invasiveness in CSF-1 receptor-positive carcinoma cell lines. Cancer Res., 52: 3661-3666, 1992. 34. Chambers, S. K., Wang. Y.. Gertz, R. E., and Kacinski, B. M. Macrophage colonystimulating factor mediates invasion of ovarian cancer cells through urokinase. Cancer Res., 55: 1578-1585, 1995. 35. Sapi, E.. Flick, M. B., Rodov, S., Gilmore-Hebert, M., Kelley, M.. Rockwell, S.. and Kacinski. B. M. Independent regulation of invasion and anchorage-independent growth by different autophosphorylation sites of the macrophage the colony-stimu lating factor 1 receptor. Cancer Res., 56: 5704-5712, 1996. 36. Yano, S.. Nishioka. Y.. Nokihara. H.. and Soné.S. Macrophage colony-stimulating factor gene transduction into human lung cancer cells differentially regulates metas tasis formations in various organ microenvironments of natural killer cell-depleted SCID mice. Cancer Res.. 57: 784-790, 1997. 37. Welch, D. R., Fabra, A., and Nakajima. M. Transforming growth factor ßstimulates mammary adenocarcinoma cell invasion and metastatic potential. Proc. Nati. Acad. Sci. USA, 87: 7678-7682. 1990. 38. Agarwal, C., Hembree. J. R.. Rorke, E. A., and Eckert, R. L. Transforming growth factor 01 regulation of metalloproteinase production in cultured human cervical epithelial cells. Cancer Res., 54: 943-949, 1994. 39. Mizoguchi, H.. Komiyama. S.. Matsui, K., Hamanaka. R.. Ono. M.. Kiue, A.. Kobayashi. M.. Shimizu. N.. Welgus. H. G.. and Kuwano. M. The response to epidermal growth factor of human maxillary tumor cells in terms of tumor growth, invasion and expression of proteinase inhibitors. Int. J. Cancer, 49: 738-743, 1991. 40. Singh-Kaw, P., Zarnegar, R., and Siegfried, J. M. Stimulatory effects of hepatocyte growth factor on normal and neoplastic human bronchial epithelial cells. Am. J. Physiol., 26«:L1012-L1020, 1995. 41. Yamashita. J-L. Ogawa, M., Yamashita. S-I., Nomura. K.. Kuramolo. M.. Saishoji, T., and Shin, S. Immunoreactive hepatocyte growth factor is a strong and independent predictor of recurrence and survival in human breast cancer. Cancer Res., 54: 1630-1633, 1994. 42. Siegfried, J. M., Weissfeld, L. A., Singh-Kaw. P., Weyanl, R. J., Testa. J. R.. and Landreneau. R. J. Association of immunoreactive hepatocyte growth factor with poor survival in resectable non-small cell lung cancer. Cancer Res., 57: 433-439, 1997. 43. Galzie, Z., Femig, D. G.. Smith, J. A., Poston, G. J., and Kinsella. A. R. Invasion of human colorectal carcinoma cells is promoted by endogenous basic fibroblast growth factor. Int. J. Cancer, 71: 390-395, 1997. 44. Noda. L, Saito, H., Ohtsubo, T., Fujieda, S., Tsuda. G.. Tsuzuki, H., Tanaka. N., Sugimoto, C.. and Saito, T. Effect of G-CSF on tumor invasion of maxillary cancer cell lines. Head and Neck Cancer, 22: 24-28. 1996. 45. Pei. X-H., Nakanishi, Y., Takayama, K., Yatsunami, J., Bai, F., Kawasaki, M.. Wakamatsu. K., Tsuruta. N., Mizuno, K., and Hará,N. Granulocyte-colony stimu lating factor promotes invasion by human lung cancer cell lines in vitro. Clin. Exp. Metastasis. 14: 351-357, 1996. Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1998 American Association for Cancer Research. Expression of Granulocyte Colony-stimulating Factor Receptor Correlates with Prognosis in Oral and Mesopharyngeal Carcinoma Hideaki Tsuzuki, Shigeharu Fujieda, Hiroshi Sunaga, et al. Cancer Res 1998;58:794-800. Updated version E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://cancerres.aacrjournals.org/content/58/4/794 Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1998 American Association for Cancer Research.