Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
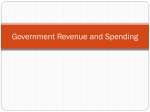
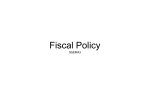
How Drug Benefits Affect Pharmaceutical and Medical Use Geoffrey Joyce Rising Expenditures on Prescription Drugs • Drug spending increasing rapidly – New drugs and higher prices – Increased insurance coverage – Aging population – Earlier diagnosis – Increased marketing and advertising • Drug spending about 10% of total expenditures – Higher percentage for non-elderly A5094-2 01/04 Health Plans Face Largest Increases in Pharmaceutical Spending % Annual Increase 1990–98 Private health plans 18% Patients 4% Source: C. Copeland, EBRI Notes (September, 2000) A5094-3 01/04 Study Questions • How does benefit design affect Rx use and costs? • Do the effects of higher cost-sharing vary by drug class and patient group? • Do pharmacy benefits affect use of medical services? • What will pharmacy benefits look like over the next 3-5 years? A5094-4 01/04 Study Sample • Linked health care claims to health plan benefits of 30 large employers (1997-2000) – 52 health plans – 529,000 primary beneficiaries age 18-64 (960,000 person-years) – Adding data for 2001-2003 A5094-5 01/04 Analytic Approach Outcomes • Pharmacy spending and use (days supplied) • Inpatient and ER use Other factors controlled for • • • • • Rx drug benefits Medical benefits; plan type Patient demographics Health status (26 chronic conditions) Area characteristics and year A5094-6 01/04 Doubling Co-payments Reduces Rx Spending Type of plan Co-payment % Reduction in total Rx spending $ Savings to plan 1-tier $5 for all drugs $10 22% 2-tier $5 generic, $10 brand $10/20 33% $220 3-tier $5 generic, $10 preferred, $15 non-preferred brand $10/20/30 35% $237 $165 A5094-7 01/04 Adding Tiers Reduces Rx Spending Rx benefit Benefit change % Reduction in total Rx spending 1-tier plan: $10 co-payment for all drugs Add 2nd tier ($20 for brand drugs) 19% 2-tier plan: $10 generic $20 brand drugs Add 3rd tier ($30 for non-preferred brand drugs) 4% 2-tier plan: $10 generic $20 brand drugs Require generics 8% A5094-8 01/04 Drugs for Treating Chronic Conditions Drug class Top drugs in 2000 Antihistamines Claritin, Allegra, Zyrtec Antiinflammatories Celebrex, Relafen, Vioxx Antidiabetics Glucophage, Rezulin, Avandia Antiasthmatics Singulair, Flovent Antiulcerants Prilosec, Prevacid, Propulsid Antihyperlipidemics Zocor, Lipitor, Pravachol Antihypertensives Norvasc, Vasotec, Cardizem CD Antidepressants Zoloft, Paxil, Prozac A5094-9 01/04 Higher Co-Pays Reduce Use; Effects Differ Across Drug Classes Antihistamines Antiinflammatories Antidiabetics Antiasthmatics Antiulcerants Chronicallyill only All members Antihyperlipidemics Antihypertensives Antidepressants 0 10 20 30 40 50 Reduction in days supplied from doubling copays (%) A5094-10 01/04 Disease-Specific Medications Decline Less Therapeutic class Antihistamines NSAIDs Antidiabetics Antiasthmatics Antiulcerants Antihyperlipidemics Within Class Other Classes Antihypertensives Antidepressants 0 5 10 15 20 25 30 35 Reduction in days supplied when co-payments double (%) A5094-11 01/04 Impact on Medical Use For diabetes, asthma and gastric acid disorder… • Doubling co-payments led to a : • 10% increase in hospital days • 17% increase in ER visits • No significant effects for other 5 conditions Preliminary evidence • Limited information on full extent of medical plan choice A5094-12 01/04 Effect of Moving Prilosec (omeprazole) to 3rd Tier 1 0.9 Plan A 0.8 0.7 Proportion of GI prescriptions 0.6 0.5 0.4 Plan B 0.3 0.2 Plan C 0.1 0 1 3 5 7 9 11 13 15 17 19 21 23 Month A5094-13 01/04 Assessing the Effects of Spending Caps The tradeoff: • Lower caps decrease cost of Rx benefit, making drug coverage available to more patients • Exceeding the cap increases risk that patients will reduce medication use Study sample: • About 1300 Medicare+Choice enrollees in one state • Exceeded annual Rx benefit cap of $750 or $1,200 in 2001 • Had resulting coverage gaps of 75-180 days A5094-14 01/04 Exceeding Caps Significantly Affected Medication Use Switched Used less often Used free samples 0 10 20 30 40 50 % of beneficiaries using strategy A5094-15 01/04 Shifting More Costs to Patients Will Continue… Survey of health plans and insurers indicate: • Continued growth in 3-tier and 4-tier benefits • Promote generics and generic-only plans • Larger co-pay differences between 1st & 3rd tiers • Tiered coinsurance • Concern over injectibles and biotech agents A5094-16 01/04 Summary of Findings • Cost-sharing matters (across plans, patient groups) – Doubling co-payments reduced use by 1/3rd – Largest reductions for drugs that treat symptoms – Smaller reductions in use by chronically ill • But price sensitivity raises health concerns • Spending caps affect adherence and use – 18% exceeding cap took less medication – 15% switched medications A5094-17 01/04 A5094-18 01/04