Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
1 .GENERAL APPEARANCE
• Patient is 30yrs old female
• look anxious
• conscious and oriented with following vital signs
•
•
•
•
B.P
PULSE
RESPIRATION
TEMPREATURE
• SpO2
: 110/70mmHg
: 88b/m
: 20b/m
: 36.6 c
: 99%
2. SKIN
• Fair complexion.
• Skin is warm.
3. HEAD
• Hair is equally distributed.
• Absence of dandruff & alopecia.
4. EYES
• Both eyes are normal , able to move both eyes.
• No discharges .
5. EARS
• Patient pinna is same colour as fascial.
• Able to hear sounds clearly.
• No discharges.
6. NOSE
• Pink nasal mucosa.
No nasal discharge
7. MOUTH
Pink and dry oral mucosa.
• Tongue and uvula in midline position.
•
Teeth is properly aligned with no dentures.
•
8. NECK AND THROAT
• No tenderness nodes.
• No palpable mass and lesions
9. CHEST & LUNGS
• Thorax is symmetric on inspection.
• Dry cough present.
• Clear breath sounds.
10. CARDIO VASCULAR SYSTEM
• ECG is normal.
• No cardiomegaly.
• Apical pulse is 88 bpm
11. UPPER &LOWER EXTREMITIES
•Normal range of motions.
12. ABDOMEN
•Bowel sounds are normal.
•On palpation Abdomen is slightly enlarged .
13 . GENITO URINARY SYSTEM
• no discharges
14.
GASTRO INTESTINAL
• No bowel obstruction present.
• Abdominal pain present.
15. NEUROLOGIC
Patient is mentally alert and oriented with
circumstances.
• Able to follow commands.
• No neurovascular deficit
•
PATIENT HISTORY
PAST MEDICAL HISTORY
No past medical history .
PRESENT MEDICAL HISTORY
Patient came to OPD on 17.5.2013 with complaints of abdominal
pain and vomiting . On examination they suspected cholelithiasis
and send her for usg abdomen . After Usg abdomen she was
diagnosed as having cholelithiasis .
PAST SURGICAL HISTORY
• Patient has
no past surgical history.
PRESENT SURGICAL HISTORY
•Patient had under gone Laproscopic choleycystectomy on
20.5.2013.
INVESTIGATIONS DONE FOR THE PATIENT
• USG Abdomen
• X-ray chest
• Blood investigations
o CBC
o ABORH
o PT/INR
o APTT
o ELECTROLYTES
ITEMS
PATIENT VALUE
NORMAL VALUE
CBC
HEMOGLOBIN(hb)
HCT
RBC
PLT
12.6 gm/dl
35.9 g/dl
3.85
2 10
13.7 - 16 .5 gm/dl
40.1 – 51.g/dl
4.63 – 6.08*10^6/ul
163-337/ul
SODIUM
143
135 - 150
POTTASSIUM
3.7
3.5-5.0mmol/l
PT
13.1
10.0-17 sec
I NR
0.85
2.4 therapeautic unit
APTT
29.2
26.1-36.3
ABRH
AB +VE
Drug
Route
Dose/frequency
Action
Inj.
Perfelgan
iv
1000mg /bd
Analgesis
Inj.Flagyl
iv
500mg /bd
antibiotics
Inj.Augmenti
n
Inj.Premos
an
iv
1.2gm/tid
Antibiotics
iv
10mg/bd
Antiemetic
iv
40mg/od
Inj.Risek
H2
receptor
antagonist
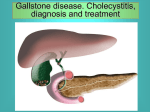
Presence of stone in the gall bladder is known as
cholelithiasis.It is a crystalline concretion formed with the gall
bladder by accretion of bile components.These gall stones are
formed in the gall bladder but may distally pass in to other parts of
biliary tract such as cystic duct,common bile duct, pancreatic duct
or thae ampulla of vater.
Choledocholithiasis
It refers to the presence of one or more Gallstones in the
common bile duct. Usually, this occurs when a gallstone
passes from the gallbladder into the common bile duct .
A gallstone in the common bile duct may impact distally in the
ampulla of Vater, the point where the common bile duct and
pancreatic duct join before opening into the duodenum
TYPES OF GALLSTONES
Types of gallstones that can form in the gallbladder
include:
Cholesterol gall stones
Pigment gall stones
Mixed gall stones
Gallbladder is a pear-shaped sac that lies between the right
medial and quadrate lobes of the liver. It is partly attachedand
partly free.
It is covered anteriorly and posteriorly by peritioneum.
It sits in a shallow depression called the
gallbladder fossa.
The gallbladder is about 7.5–10 cm (3–4 inches) long and
about a 2.5 cm (1 inch) wide.
LAYERS OF GALL BLADDER
Muscular layer ( A layer of smooth
muscle)
Perimuscular layer (connective tissue
that covers the muscular layer.
Mucosa (inner layer of epithelium and
connective tissue)
Serosa (outer covering of the
gallbladder
For the purpose of description gallbladder is divided in to
three;
Fundus of the gallbladder
Body of the gallbladder
Neck of gallbladder
BILE DUCT,HEPATIC DUCT,
CYSTIC DUCT ,BILE
It is a yellowish green fluid made by the liver. The gall bladder stores
bile produced in the liver.The gall bladder can stores about 40 ml-70
ml of bile. Bile is important in the digestion of lipids.
Bile is mainly made up of:
•
•
•
•
bile salts
bile pigments (such as bilirubin)
cholesterol
water
Bile duct formed by the union
of hepatic duct &cystic duct
that carries bile from liver
&gallbladder to the
duodenum.
Main excretory duct of liver which joins the cystic duct to form the
common bile duct.
It drains bile from the liver through the left and right hepatic duct.
The cystic duct joins the
gallbladder to the common
bile duct. It usually lies next
to cystic artery.The Cystic
duct of the gallbladder is 24 cm long
ARTERIAL SUPPLY,
VENOUS DRAINAGE &LYMPHATIC DRAINAGE
:
FUNCTIONS OF GALL BLADDER
•
•
•
•
•
Stores and mobilizes bile.
for digestion.
Promote physical coordination.
Maintain health of connective tissues.
Closed linked with the liver.
Defensive energy against catching infections.
Etiology Of Cholelithiasis
•
•
•
•
•
•
•
•
Female sex.
European or native american ancestry
Increasing age above 40 yrs
Obesity.
Pregnancy.
Gallbladder stasis.
Drugs.
Heredity.
Factors that may increase risk of gallstones include:
•
•
•
•
•
•
•
•
•
•
•
•
•
Being female
Being age 60 or older
Being an American Indian
Being a Mexican-American
Being overweight or obese
Being pregnant
Eating a high-fat diet
Eating a high-cholesterol diet
Eating a low-fiber diet
Having a family history of gallstones
Having diabetes
Losing weight very quickly
Taking some cholesterol-lowering medications
•
•
•
•
•
•
pain in the upper right portion of abdomen.
Back pain between shoulder blades
Pain in right shoulder.
Nausea and vomiting.
Jaundice.
Clay coloured stool .
DIAGNOSTIC STUDIES
HIDA SCAN
CT SCAN
ERCP
ABDOMINAL
ULTRA SOUND
BLOOD TESTS
CHOLESTEROL AND CALCIUM BILIRUBINATE IN
BILE ARE PRESENT IN CONCENTRATIONS THAT
APPROACH THE LIMITS OF THEIR SOLUBILITY
BILE IS CONCENTRATED IN THE GALLBLADDER,
IT CAN BECOME SUPERSATURATED WITH THESE.
SUBSTANCES
PRECIPITATE FROM SOLUTION AS
MICROSCOPIC CRYSTALS
CRYSTALS ARE TRAPPED IN GALLBLADDER
MUCUS, PRODUCING GALLBLADDER SLUDGE
CRYSTALS GROW, AGGREGATE, AND FUSE TO
FORM MACROSCOPIC STONES.
OCCLUSION OF THE DUCTS BY SLUDGE
AND/OR STONES
GALLSTONE DISEASE
I.
MEDICAL MANAGEMENT
ORAL BILE SALT THERAPY(URSODEOXYCHOLIC+URSODIOL
CONTACT DISSOLUTION
EXTRA CORPOREAL SHOCK WAVE LITHOTRIPSY
LAPROSCOPIC
CHOLECYSTECTOMY
ENDOSCOPIC
SPHINCTEROTOMY
SURGICAL
OPEN
CHOLECYSTECTOMY
CHOLECYSTOSTOM
Y
GALL
BLADDER
EMPYEMA
GALL
BLADDER
ADENO
CARCINOMA
ACUTE
CHOLECYSTITIS
PERFORATION
AND PERI
CHOLECYSTIC
CHOLEY
CYSTOENTRIC
FISTULAS
ABSCESS
GALL STONE
ILEUS
COMPLICATIONS OF SURGERY
• Infection of an incision.
• Internal bleeding.
• Injury to the common bile duct .
• Injury to the small intestine by one of the instruments used
during surgery.
• Risk of general anaesthesia .
UNCOMMON COMPLICATIONS
• Injury to the cystic duct,.
• Gallstones that remain in the abdominal cavity.
• Bile that leaks into the abdominal cavity.
• Injury to abdominal blood vessels, such as the major blood
vessel carrying blood from the heart to the liver (hepatic
artery)..
• A gallstone being pushed into the common bile duct.
• The liver being cut.
PRE-OPERATIVE INTERVENTION
• The provision of psycho-educational care.
• Provision of adequate and appropriate informastion thruogh out the day care
experience .
• Enhancement of patient self-efficacy via positive encouragement and
information provision.
• Reduction of the negative impact of the clinical environment and encouraging
implicit and explicit messages of safety such as
the hospital performs many operations .
• helps to create a warm, friendly and comfortable environment.
POST OP INTERVENTION
• Management of pain and post-operative nausea and vomiting.
• Initial assistance with mobilization.
• Pain management should commence with an assessment of the patient’s
pain at regular intervals.
• Measures to manage patients’ anxiety should be implemented preoperatively and continued throughout the post-operative recovery period
until discharge
Care of Patient with Cholecystectomy
Preventing respiratory complications
Encouraging activity.
Promoting wound healing.
Maintaining normal body temperature.
Promoting bowel function ..
maintaining gastro intestinal function and
resuming nutrition .
ACUTE PAIN RELATED TO GALL BLADDER REMOVEL
NAUSEA AND VOMITING RELATED TO SURGERY
RISK FOR INFECTION RELATED TO SURGICAL INCISION
KNOWLEDGE DEFICIT RELATED TO TREATMENT
REGIMEN AND POST OP CARE
ASSESSMEN NSG
T
DIAGNOSIS
Subjective
I have severe
pain as
verbalized by
the patient.
Painscale -5/10
As 0/10 is the
lowest and 10/10 is
the highest
{WONG –BAKER}
Objective
data:
Fascial
grimace
Reports
pain on
movement
Guarding
behavior
Altered
comfort,pai
n, related to
tissue
trauma
secondary
to surgical
operation.
PLANNING
INTERVENTION
RATIONAL
EVALUATON
After series of
nursing
intervention
patient will
manifest a
decrease in pain
Scale from 5/10
to 0/10
1.Assess patients pain
scale and perception
1.To identify the
onset ,intensity and
duration of pain
2.to reduce the pain
and to provide
relaxation
After 12 hrs of
nursing
interventions
the goals were
fully met as
evidenced by
2. provid comfort
measures (backrub,
position change,
environmental control)
3. Encourage deep
3.To assist muscle
breathing exercises
and genarelised
relaxation
4.Teach divertional
4.To destract clients
activities(listening to
attention from pain
music)
5. Monitor vital signs
5.To identify the
intensity of pain
6.Administer pain
medication per doctor’s
order prior to exercise
or activities of daily
living{INJ.PERFELGAN
1GM IV BD}
.
6. To relieve the pain
verbalize
relief of pain
as evidenced
by a pain scale
of 0 out of 10
positive
response
during
evaluation
verbalize &
demon-strate
willingness to
partici-pate in
activities
HEALTH EDUCATION
• Health education given on wound care and dressing .
• Instructed her the signs of infection and asked him to notify if
any signs occurs .
• Instructed her to follow the physians order regarding diet
and medication.
• Educated her the the importance of follow up .
• Instructed her she will have no restrictions to physical
activities, however the patient should listen to their body in
response to certain activities. Gradually increase activities at
a comfortable and individual pace.
• Advised her to contact if he develops any problems such as
prolonged nausea/vomiting, temperature elevations above
101.5 or other difficulties.
• Advised her to take the medications accordingly.
CONCLUSION
•
•
•
•
Presented a case of patient with cholelithiasis.
Patient underwent laproscopic cholecystectomy on 20/05/13.
Presence of stone in the gall bladder is known as cholelithiasis
It is a crystalline concretion formed with the gall bladder by
accretion of bile components.
•Gallstones may cause no signs or symptoms.Gall stones may be
asymptomatic even for years .these stones are called silent
stones . If a gallstone lodges in a duct and causes a blockage,
signs and symptoms may result.
•Laproscopic cholecystectomy has now replaced open
cholecystectomy as the first-choice of treatment for gall stones
and inflammation of the gallbladder unless there are
contraindications to the laparoscopic approach. This is because
open surgery leaves the patient more prone to infection.
BIBLIOGRAPHY
•
BRUNNER AND SUDDARTH TEXT BOOK OF
MEDICAL –SURGICAL NURSING 9 TH
EDITION .
•
LIPPIN COTT WILLIAMS AND WILKINS.
•
POTTER AND PERRY FUNDAMENTALS OF
NURSING 5 TH EDITION
•
WWW.WIKIPEDIA.ORG.