Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
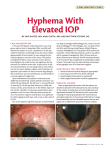
PHARMACOLOGY OF GLAUCOMA TARIQ ALASBALI Glaucoma: Treatment Goal “The goal of glaucoma treatment is to preserve the visual field of patients and prevent the loss of visual function associated with the disease.” Ref: Survey of Ophthalmology; 2003 Vol. 48(1): S1-S3 What is a target IOP? “The IOP at which the rate of retinal ganglion cell loss is no greater than the age related loss.”Brubaker AAO Guidelines: Target IOP % reduction from baseline 40 40 35 30 25 20 15 10 5 0 30 30 20 Mild Damage Advance Damage NTG OHT Ref: Survey of Ophthalmology 2003; 48 (suppl 1); 53-57 Target IOP is based on over-all glaucomatous damage Optic Nerve Damage IOP Target IOP VF Risk Factors FLUCTUATIONS IN IOP REQUIREMENT OF AN AGENT FOR PROVEN 24-HOUR CONTROL Not only controlling peak IOP is important but the drug should also control fluctuations in IOP In POAG what is your first line drug and why? What are your next choices? PG/PA Target Achieved: Continue to Follow Target Not Achieved Ineffective Or Side effect Effective Not at Target Continue & Return to Top with Additional Drug Discontinue & Return to Top with Different Drug Beta-Blockera Brimonidinea Topical CAIa Cholinergicb Oral CAIb a: Order depends on side effects & contraindications b: Secondary Drugs Consider other therapies also Primary Drug Classes Prostaglandin Analogues / Prostamides Beta Adrenergic Antagonists ‘Beta blockers’ Alpha 2 Adrenergic Agonists Carbonic Anhydrase Inhibitors Primary Drug Classes A meta-analysis of 27 articles suggests that bimatoprost, travoprost, latanoprost, and timolol are the most effective intraocular pressure-reducing agents in POAG and OH patients. Ophthalmology. 2005 Jul;112(7):1177-85 . Prostaglandin Analogues is approved by (FDA), as a first line treatment for elevated (IOP) associated with open angle glaucoma or ocular hypertension http://www. medscape.com assessed on 18/11/03 Secondary Drug Classes Parasympathomimetics Cholinergic (Muscarinic) Agonists Acetylcholinesterase inhibitors Non-selective Adrenergic Agonists Rarely used Drug class Medication Mean ↓IOP % ↓IOP PGA Latanoprost Bimatoprost Travoprost 6-8 mm Hg 7-8 mm Hg 7-8 mm Hg ~ 30% B-blocker, non selective Timolol ~6mm Hg ~25% A-2 adrenergic Brimonidine 2-6 mm Hg 20-25% B-blocker, selective Betaxolol 4-5 mm Hg ~20% CAI Dorzolamide 3-5 mm Hg 15-20% Prostaglandin Analogues & Prostamides: Dosing & Preparations Latanoprost Travoprost Bimatoprost All QHS Latanoprost: Instillation at 9 pm 27 25 IOP (mmHg) 23 Latanoprost when instilled at 9 pm effective controlled IOP at 9 am Peak IOP 21 Baseline 19 Latanoprost 17 15 0 15 18 21 24 03 Time (hours) 06 09 12 Prostaglandin Analogues & Prostamides: Mechanism of Action Increase uveoscleral outflow At least 8 PG receptor subtypes Latanoprost and Travoprost analogues of PGF2α bind known PG receptors Whether Bimatoprost works in the same way seems to depend on whether you work for Allergan or Pfizer Prostaglandin Analogues & Prostamides: Mechanism of Action Free acid is active component at PG receptors Requires enzymatic cleavage Latanoprost and Travoprost are esters Esterases present in cornea and a.c. Bimatoprost is an amide. Prostaglandin Analogues & Prostamides: IOP Response Expected IOP lowering: ~30% Latan = Trav=Bim (1) Another finding difference, generally < 1mmHg (2) Recent Meta-Analysis (3) Latan: 31% peak, 28% trough Trav: 31 % peak, 29% trough Bim: 33 % peak, 28% trough Onset of IOP lowering 2-4 hours Peak Effect 8-12 hours Wash Out 4-6 weeks 1-Clin Experiment Ophthalmol. 2006:34(8):755-64. 2-Adv Ther. 2004 Jul-Aug;21(4):247-62. 3-Ophthalmology.2005:112(7):1177-1185 PROSTAGLANDIN: Proven for 24 hour IOP Control Baseline Dorzolomide three times daily 27 Timolol twice daily Latanoprost, travoprost, and bimatoprost were effective in reducing the 24-h IOP in patients with XFS and OH Latanoprost 25 IOP (mmHg) 23 21 19 17 15 Eye (2007) 21, 453–458 0 15 18 21 24 03 Time (hours) Ref: Invest Ophthalmol Vis Sci 2000; 41: 2566-2573 06 09 12 Prostaglandin Analogues & Prostamides: Interactions with Other IOP drugs Theoretically expected to have poor additivity with parasympathomimetics Clinically, this has not been proven Good additivity to others Prostaglandin Analogues & Prostamides: Side Effects Lash Changes Pigmentation Iris Periocular skin Pro-Inflammatory Hyperemia of Conjunctiva Uveitis CME Reactiviation of HSV keratitis Beta-Blocker Preparations Non-selective Timolol 0.25%, 0.5% Gel-vehicle (Timoptic XE 0.25%, 0.5%) Levobunolol 0.25%, 0.5% Befunolol Metipranolol Beta 1 Selective Betaxolol 0.25%, 0.5% Beta-Blocker Preparations With ISA Cartelol 0.5% - 2% Pindolol 2% Beta Blockers: Mechanism of Action Mediated through beta 2 adrenergic receptors Decreases aqueous production Beta Blockers: Dosing BID dosing except gel-vehicle Increasing beyond BID of no help Timoptic XE once daily in a.m. Beta Blockers: IOP Response Expected IOP lowering: ~25% Peak effect Two hours Wash out 2-5 weeks Beta Blockers Use w/ systemic β-blocker: • No additional effect on pulse or BP • ↓ IOP lowering with ↑ oral dose • Use of systemic β-blocker can mask prior IOP elevation and cause pseudo-NTG picture Beta-Blockers Carteolol 1% Intrinsic sympathomimetic activity • Theoretically causes less bronchoconstriction, bradycardia, vasoconstriction • Less ocular irritation • Better tolerated in dry eye patients Beta-Blockers Betagan ® Levobunolol 0.25%, 0.5% • Slightly longer half-life than timolol; ? qd dosage Betoptic-S® (betaxolol 0.25% ): β1-selective • Less pulmonary and CNS side effects • Less systemic absorption than timolol Beta Blockers: Side Effects Bronchospasm Bradycardia, arrhythmia CHF Syncope Hypotension Depression Sexual dysfunction Beta-Blockers: Contraindications Asthma (Reactive Airway Disease) Bradycardia Heart block Acute CHF Alpha 2 Agonists:Dosing & Preparations Iopidine® (apraclonidine 0.5%, 1%) BID-TID - α1, α2 Decreases aqueous production May lose efficacy after 4-6 months Alphagan-P® (brimonidine 0.1%, 0.15%), generic brimonidine 0.2% BID-TID - α2-selective ↓aqueous production; ↑uveoscleral outflow May lose efficacy after 1 year Neuroprotection? BRIMONIDINE : THE NEUROPROTECTIVE a2 AGONIST Brimonidine neuroprotection may be mediated through up-regulation of Brain-derived neurotrophic factor BDNF in the retinal ganglion cells RGCs. Brimonidine may be (potentially) used clinically as a neuroprotective agent. Arch Ophthalmol. 2002;120:797-803. Alpha 2 Agonists: IOP Response Expected IOP lowering: 20-25% Peak Effect 2 hours Wash Out 1-3 weeks Alpha 2 Agonists: IOP Response A recent study conclude that Brimonidine 0.2% has a higher potency of lowering IOP than brimonidine Purite 0.15% at trough when used twice-daily. However, ocular allergic reaction was more frequent and severe with brimonidine 0.2% than with brimonidine Purite 0.15%. Journal of Ocular Pharmacology and Therapeutics. 2007, 23(5): 481-486. Alpha 2 Agonists: IOP Response One study suggests: brimonidine purite BID= dorzolamide BID ??? British Journal of Ophthalmology956-88:953;2004 Alpha 2 Agonists: Side Effects Follicular conjunctivitis 50% apraclonidine 15% (at least) brimonidine Less with Alphagan P Need more non-pharmaceutical company data Fatigue, drowsiness Eye lid retraction Dry mouth Hypotension Alpha 2 Agonists: Side Effects Apnea in infants and young children weight > 20 Kg age > 6 Years Alternative glaucoma therapy should be considered . Ophthalmology Volume 112, Issue 12, December 2005 CAIs : Dosing & Preparations Topical Trusopt® Dorzolamide 2%: BID – TID Azopt® Brinzolamide 1%: BID – TID Oral Diamox® Acetazolamide: 250mg QID, SR 500 BID Neptazane® Methazolamide: 50-100mg Once/Day-TID CAIs: Mechanism of Action Inhibit CA enzyme in ciliary body epithelium Decrease aqueous production Improve ocular blood flow? Topical CAIs : IOP Response Expected IOP lowering: 15-20% Wash Out Topical: 1 week Oral: 3 days Topical CAIs : Side Effects Ocular surface irritation Contact allergy Contraindication: Sulfonamide allergy Oral CAIs: Side Effects Paresthesias Tinnitus Depression Loss of appetite GI symptoms Kidney stones Metabolic acidosis Electrolyte imbalance Oral CAIs: Side Effects Anaphylaxis Stevens-Johnson Syndrome Bone marrow dysfunction Idiosyncratic Can be any cell line aplastic anemia most described Some reversible some not Potentially lethal CAIs Oral is additive to topical (1-2mmHg) Topical not additive to oral Methazolamide 75% liver metabolized Safer in renal disease Eg. Diabetic with CRF and NVG Parasympathomimetics: Dosing & Preparations Pilocarpine 0.5% - 4% BID-QID 4% gel once daily (QHS) Carbachol 0.75% - 3% BID-TID Parasympathomimetics: Mechanism of Action Increase TM outflow Believed secondary to contraction of smooth muscle fibers inserting into scleral spur Parasympathomimetics: IOP Response Expected IOP lowering: 10-20 % Lowers IOP by 1 hour post instillation Wash Out: 3 days Parasympathomimetics: Side Effects Pro-inflammatory Break down blood ocular barrier Miosis Brow ache (<~40 y.o.) P.S. Shallowing of A.C. Possible worsening of pupil block RD Cataract Fixed Combination Cosopt Combigan Xalacom DuoTrav Ganfort Fixed Combination XALACOM QD = TIMOLOL BID + XALATAN QHS (1) XALACOM QD > COSOPT BID (2) XALACOM QD > BRIMONIDINE BID + TIMOLO BID (3) 1-Ophthalmology. 2006 Jan;113(1):70-6 2-Ophthalmology 2004 .Feb;111(2):276-8 . 3-Acta Ophthalmol Scand. 2003 Jun;81(3):242-6 Fixed Combination Martinez et all study showed a significantly higher IOP-lowering effect of a once-daily evening dose of the BTFC compared to that of a oncedaily evening administration of the LTFC. (1) (1) Current Medical Research and Opinion, Volume 23, Number 5, May 2007 , pp. 1025-1032(8) EXAMPLE Main outcome measure To evaluate the efficacies of bimatoprost and travoprost for lowering of IOP for the treatment of glaucoma and ocular HTN. Result: The mean reduction in the bimatoprost group were greater than the reduction in the travoprost group at every study visit, but these differences were not significant (p >0.207). Abstract conclusion: Bimatoprost provided greater mean IOP reduction than travoprost. Br J Ophthalmology 2006; 90:1370-1373. COMPLIANCE: THE HIDDEN CHALLENGE OF GLAUCOMA MANAGEMENT Patient Compliance: Glaucoma Patient compliance is a particularly important issue in glaucoma because: Asymptomatic Long term therapy Benefit of treatment not apparent Several medications Expense of treatment Inconvenience of treatment Side effects of treatment Ref: J of Glaucoma 1992; 1: 134-136 Patient Non-compliance: Glaucoma Available literature suggests that between 28% and 58% of glaucoma patients do not use their medications as prescribed Non compliance is probably 30%-40% Ref: http://www.escrs.org/April 2003 assessed on 27/03/04 Preservatives BAK has demonstrated cytotoxic effects in cell culture, as well as in animal and human studies. Physicians should consider treatment with newgeneration preparations containing low-risk preservatives, especially in patients receiving multiple ophthalmic medications . Adv Ther. 2001 Sep-Oct;18(5):20515. Preservatives A study on rats corneas suggest that glaucoma medications with low levels of BAK, alternative preservatives such as Purite®, or preservative-free formulations are more benign to the ocular surfaces. Cornea. 2004 Jul;23(5):490-6. Preservatives British Journal of Ophthalmology:2002-86-418-423 Preservatives Alphagan P Alphagan Lumigan Combigan Trusopt Cosopt Azopt Timoptic Betoptic Travatan Xalatan Xalacom Purite 0,005% 0,005% 0.005% 0.0075% 0.0075% 0.01% 0.01% 0.01% 0.015% 0.02% 0.02 % A Little Perspective… “The risk and cost, including side effects of treatment to lower pressure, must be weighed against the risk of pressure itself.”Hodapp If you light a lamp for somebody , It will also brighten your path