Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
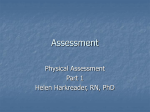
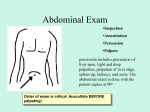
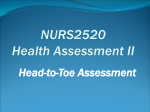
Basics of Patient Presentations Including History and Physical AFAMS Residency Orientation Objectives • Learn the different types of presentations • Master the techniques necessary to properly present a patient • Obtaining a History and Physical • Understand purpose of each physical exam maneuver Obtaining a History • Ask questions focused on the patient’s chief complaint • Questions shouldn’t be too specific • Allow the patient to fully answer the question • Your last question should be “Is there anything else that I didn’t specifically ask you about?” Formal Presentations • 7 minutes or less • Requires – Style – Substance • No time wasted on superfluous information • Follows standard template from history to assessment / plan Types of Presentations • New Patient – History, Physical, Assessment and Plan • Follow Up – Patient presented on a previous day – Abridged presentation referencing only major patient issues • Bedside – Ask the patient’s permission first – Student/resident presents to attending while standing next to the patient New Patient Presentation • History of Present Illness • Past Medical and Surgical History • Family and Social History • Medications and Allergies • Physical Exam Findings • Laboratory and Radiographic Findings • Differential Diagnosis • Assessment and Plan New Patient: History of Presenting Illness • Include symptom – – – – Quality Severity Location Duration • Last portion of History of Presenting Illness is review of systems – Complete head to toe review of any symptom the patient may have New Patient: Medical History • Past Medical History – Include the patient’s previous illness or diagnoses • Past Surgical History – Name of all previous procedures and surgeries – Include dates, indications, and complications New Patient: Further History • Family History – Include any medical conditions affecting patient’s parents or siblings • Social History – Occupation – Alcohol use – Tobacco use New Patient: Medications and Allergies • Allergies – Any medication allergies – Any major food or environmental allergies • Medications – Any current prescription medication – Herbal supplements – Over-the-counter medications New Patient: Physical Exam • • • • • • • Head and Neck Cardiovascular Respiratory Abdominal Extremity Musculoskeletal Neurological Physical Exam: Head and Neck • Lymph Nodes – Cancer – Infection • Feeling for enlarged, warm, firm, or tender • Palpate all lymph node chains Physical Exam: Head and Neck • Ear – External Exam (infection or cancer) – Internal Exam (infection) • Otoscope – Tympanic Membrane’s color, posterior structures, light reflex Physical Exam: Head and Neck • Auditory Acuity – Sensorineural Defects • Weber Test • Rinne Test – Conduction Defects • Weber Test WEBER RINNE Physical Exam: Head and Neck • Nose – Mucosal Color – Presence of Discharge • Sinuses – Maxillary Sinus – Frontal Sinus – Directly palpate and percuss sinuses – Examine for discharge – Tap teeth with tongue depressor (inflamed maxillary sinuses) Physical Exam: Head and Neck • Oropharynx – Using light and tongue depressor have patient stick out tongue and say “Ah” • • • • CN 9 dysfunction Nutrition Dental Hygiene Infection – Peritonsillar Abscess Physical Exam: Head and Neck • Thyroid Exam – Goiter – Nodule • Methods of examination – Palpation – Observation Physical Exam: Cardiovascular • Three components to Cardiovascular exam – Observation – Palpation – Auscultation • Observation – Jugular Venous Distension • IJ NOT EJ • Head at 45 degrees • Angle of Louis Physical Exam: Cardiovascular • Palpation – Palm on left sternal edge, fingers extended – Point of Maximal Impulse • Should be on midclavicular line, 5th intercostal space • Duration of impulse • Thrill? Physical Exam: Cardiovascular • Auscultation – Never listen through clothing – Know all four valvular regions Physical Exam: Cardiovascular • Discern S1 and S2 • Recognize systole and diastole • When a murmur is present – – – – Systole vs. Diastole Duration Intensity Associated Sounds Physical Exam: Cardiovascular • Murmurs are graded – I: Heard with careful listening – II: Easily audible with stethoscope – III: Louder than II – IV: As loud as III, but with additional thrill – V: Audible with stethoscope barely touching chest – VI: Heard without stethoscope Physical Exam: Pulmonary • Four components of the pulmonary exam – – – – Inspection / Observation Palpation Percussion Auscultation Physical Exam: Pulmonary • Observation – General Comfort – Breathing Pattern • Pursed Lips • Wheezing or gurgling – Use of Accessory Muscles • Intercostals • Sternocleidomastoids – Patient Color • Lips, Nail beds, face – Position of Patient • Upright or leaning forward Review of Lung Anatomy Physical Exam: Pulmonary • Palpation – Detecting Chest excursion – Tactile Fremitus will be altered by pathology: • Consolidation • Pleural Fluid Physical Exam: Pulmonary • Percussion – Normal: tapping on chest produces resonant note – Fluid filled cavity (consolidation or effusion): dullness – Conditions that lead to air trapping (emphysema and PTX): hyper resonant Physical Exam: Pulmonary • Percussion Percussion Technique Physical Exam: Pulmonary • Auscultation: first remember the location of each lobe in the lung fields • Anterior Physical Exam: Pulmonary • Posterior Physical Exam: Pulmonary • Normal breath sounds – Vessicular • Wheezes – Mucosal edema – Bronchoconstriction – Inspiratory vs. Expiratory • Rales or crackles – Result of fluid accumulation Physical Exam: Abdomen • Components of the exam are – – – – Observation Auscultation Percussion Palpation • Always think anatomically Physical Exam: Abdomen • Abdomen is divided into four quadrants Physical Exam: Abdomen • Observation – Appearance of abdomen • Distended • Flat • Symmetric or Asymmetric – Prior surgical scars – Signs of Peritonitis • Patient laying very still • In pain with minor movements Physical Exam: Abdomen • Auscultation – Listen in all four quadrants 15 seconds in each – Bowel sounds • Present vs. Absent • How frequently? – Renal Artery Bruits Physical Exam: Abdomen Percussion • Two solid organs produce dull sound – Liver – Spleen • Look for production of pain with percussion • Percussion can assist in determining source of abdominal distention – Fluid – Gas Physical Exam: Abdomen Palpation • Always in a normal area – If pain in RUQ, start in LLQ • Palpate lightly first • Then repeat with deeper palpation • Palpate internal organs if possible • Note pain or splinting • Palpate the aorta around the umbilicus • Is there any fluid or ascites? Physical Exam: Upper Extremities • Examine nail – – – – • • • • • Shape Color Deformity Capillary Refill Joint Deformity Cyanosis Radial pulse Edema Axillary Lymph Node Physical Exam: Lower Extremities • • • • • • • • Femoral Pulse Inguinal Hernia Popliteal Pulse Pedal Pulse Edema Knee joint swelling Gangrene Cellulitis Physical Exam: Extremities Palpation of Axillary Lymph Nodes Onychomycosis Cellulitis Gangrene Joint Deformity Cyanosis Physical Exam: Musculoskeletal Exam Physical Exam: Neurological Exam • Can be a comprehensive or cursory exam • Major Components – Mental Status – Cranial Nerves – Muscle strength, tone and bulk – Reflexes – Coordination – Sensory Function – Gait Physical Exam: Cranial Nerves • CN 1: Olfactory Sense • CN 2: Visual Acuity • CN 3, 4, 6: Extra-ocular muscle movement • CN 4: Superior Oblique muscle CN 6: Lateral Rectus CN 3: Inferior oblique Inferior rectus, superior rectus, and medial rectus Physical Exam: Cranial Nerves • CN 5 – Motor: Temporalis and Masseter muscles – Sensory • V1: Forehead • V2: Check • V3: Jaw • CN 7 – Most of the facial muscles • CN 8: Acoustic Acuity – Weber – Rinne Physical Exam: Cranial Nerves • CN 9: Glosopharyngeal • CN 10: Vagus • Together CN 9 and 10 raise the soft palate and produce gag reflex Physical Exam: Cranial Nerves • CN 11: Innervates muscles which permit shrugging of shoulders • CN 12: Responsible for tongue movement Physical Exam: Sensory • Spinothalamics: detect pain, temperature, crude touch • Dorsal Columns: detect position, vibratory and light touch Physical Exam: Motor Assessment • Observe muscle bulk • Look for asymmetry between extremities • Examine major muscle groups of upper and lower extremities – – – – – Biceps Triceps Deltoids Quadriceps Hamstrings Motor Assessment • Assessment of muscle strength • 0: No movement • 1: Slight flicker of muscle movement • 2: Can voluntarily move, but cannot overcome gravity • 3: Can overcome gravity, but not applied resistance • 4: Can overcome gravity and some resistance • 5: Normal Follow Up Presentation • 1-2 sentence summary of patient’s presentation and hospital course • Explanation of past 24 hour events • Physical Exam • Important Laboratory and Radiographic Studies • Assessment and Plan Questions You May Be Asked During the Presentation • Etiology of Symptoms • Pathophysiology of Disease • Diagnosis Criteria • Common Complications • Differential Diagnosis • Diagnostic Tests • Treatment Options Miscellaneous Tips • Include only essential facts in your presentation – Be prepared to answer any questions with more detail • Keep the same order and format for all presentations • Be thorough with your differential diagnosis and treatment plan Miscellaneous Tips • Try not read directly off paper • Presentation should be as conversational as possible • Expect questions and be prepared to answer them Conclusions • A tremendous amount of information can be obtained by a properly conducted history and physical • It is important to be an excellent presenter and be able to convey important information to other medical professionals