Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
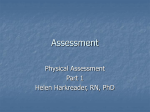
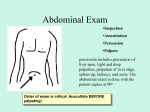
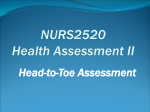
Basics of Patient Presentations Including History and Physical AFAMS Residency Orientation Objectives • Learn the different types of presentations • Master the techniques necessary to properly present a patient • Obtaining a History and Physical • Understand purpose of each physical exam maneuver Obtaining a History • Ask questions focused on the patient’s chief complaint • Questions shouldn’t be too specific • Allow the patient to fully answer the question • Your last question should be “Is there anything else that I didn’t specifically ask you about?” Formal Presentations • 7 minutes or less • Requires – Style – Substance • No time wasted on superfluous information • Follows standard template from history to assessment / plan Types of Presentations • New Patient – History, Physical, Assessment and Plan • Follow Up – Patient presented on a previous day – Abridged presentation referencing only major patient issues • Bedside – Ask the patient’s permission first – Student/resident presents to attending while standing next to the patient New Patient Presentation • History of Present Illness • Past Medical and Surgical History • Family and Social History • Medications and Allergies • Physical Exam Findings • Laboratory and Radiographic Findings • Differential Diagnosis • Assessment and Plan New Patient: History of Presenting Illness • Include symptom – – – – Quality Severity Location Duration • Last portion of History of Presenting Illness is review of systems – Complete head to toe review of any symptom the patient may have New Patient: Medical History • Past Medical History – Include the patient’s previous illness or diagnoses • Past Surgical History – Name of all previous procedures and surgeries – Include dates, indications, and complications New Patient: Further History • Family History – Include any medical conditions affecting patient’s parents or siblings • Social History – Occupation – Alcohol use – Tobacco use New Patient: Medications and Allergies • Allergies – Any medication allergies – Any major food or environmental allergies • Medications – Any current prescription medication – Herbal supplements – Over-the-counter medications New Patient: Physical Exam • • • • • • • Head and Neck Cardiovascular Respiratory Abdominal Extremity Musculoskeletal Neurological Physical Exam: Head and Neck • Lymph Nodes – Cancer – Infection • Feeling for enlarged, warm, firm, or tender • Palpate all lymph node chains Physical Exam: Head and Neck • Ear – External Exam (infection or cancer) – Internal Exam (infection) • Otoscope – Tympanic Membrane’s color, posterior structures, light reflex Physical Exam: Head and Neck • Auditory Acuity – Sensorineural Defects • Weber Test • Rinne Test – Conduction Defects • Weber Test WEBER RINNE Physical Exam: Head and Neck • Nose – Mucosal Color – Presence of Discharge • Sinuses – Maxillary Sinus – Frontal Sinus – Directly palpate and percuss sinuses – Examine for discharge – Tap teeth with tongue depressor (inflamed maxillary sinuses) Physical Exam: Head and Neck • Oropharynx – Using light and tongue depressor have patient stick out tongue and say “Ah” • • • • CN 9 dysfunction Nutrition Dental Hygiene Infection – Peritonsillar Abscess Physical Exam: Head and Neck • Thyroid Exam – Goiter – Nodule • Methods of examination – Palpation – Observation Physical Exam: Cardiovascular • Three components to Cardiovascular exam – Observation – Palpation – Auscultation • Observation – Jugular Venous Distension • IJ NOT EJ • Head at 45 degrees • Angle of Louis Physical Exam: Cardiovascular • Palpation – Palm on left sternal edge, fingers extended – Point of Maximal Impulse • Should be on midclavicular line, 5th intercostal space • Duration of impulse • Thrill? Physical Exam: Cardiovascular • Auscultation – Never listen through clothing – Know all four valvular regions Physical Exam: Cardiovascular • Discern S1 and S2 • Recognize systole and diastole • When a murmur is present – – – – Systole vs. Diastole Duration Intensity Associated Sounds Physical Exam: Cardiovascular • Murmurs are graded – I: Heard with careful listening – II: Easily audible with stethoscope – III: Louder than II – IV: As loud as III, but with additional thrill – V: Audible with stethoscope barely touching chest – VI: Heard without stethoscope Physical Exam: Pulmonary • Four components of the pulmonary exam – – – – Inspection / Observation Palpation Percussion Auscultation Physical Exam: Pulmonary • Observation – General Comfort – Breathing Pattern • Pursed Lips • Wheezing or gurgling – Use of Accessory Muscles • Intercostals • Sternocleidomastoids – Patient Color • Lips, Nail beds, face – Position of Patient • Upright or leaning forward Review of Lung Anatomy Physical Exam: Pulmonary • Palpation – Detecting Chest excursion – Tactile Fremitus will be altered by pathology: • Consolidation • Pleural Fluid Physical Exam: Pulmonary • Percussion – Normal: tapping on chest produces resonant note – Fluid filled cavity (consolidation or effusion): dullness – Conditions that lead to air trapping (emphysema and PTX): hyper resonant Physical Exam: Pulmonary • Percussion Percussion Technique Physical Exam: Pulmonary • Auscultation: first remember the location of each lobe in the lung fields • Anterior Physical Exam: Pulmonary • Posterior Physical Exam: Pulmonary • Normal breath sounds – Vessicular • Wheezes – Mucosal edema – Bronchoconstriction – Inspiratory vs. Expiratory • Rales or crackles – Result of fluid accumulation Physical Exam: Abdomen • Components of the exam are – – – – Observation Auscultation Percussion Palpation • Always think anatomically Physical Exam: Abdomen • Abdomen is divided into four quadrants Physical Exam: Abdomen • Observation – Appearance of abdomen • Distended • Flat • Symmetric or Asymmetric – Prior surgical scars – Signs of Peritonitis • Patient laying very still • In pain with minor movements Physical Exam: Abdomen • Auscultation – Listen in all four quadrants 15 seconds in each – Bowel sounds • Present vs. Absent • How frequently? – Renal Artery Bruits Physical Exam: Abdomen Percussion • Two solid organs produce dull sound – Liver – Spleen • Look for production of pain with percussion • Percussion can assist in determining source of abdominal distention – Fluid – Gas Physical Exam: Abdomen Palpation • Always in a normal area – If pain in RUQ, start in LLQ • Palpate lightly first • Then repeat with deeper palpation • Palpate internal organs if possible • Note pain or splinting • Palpate the aorta around the umbilicus • Is there any fluid or ascites? Physical Exam: Upper Extremities • Examine nail – – – – • • • • • Shape Color Deformity Capillary Refill Joint Deformity Cyanosis Radial pulse Edema Axillary Lymph Node Physical Exam: Lower Extremities • • • • • • • • Femoral Pulse Inguinal Hernia Popliteal Pulse Pedal Pulse Edema Knee joint swelling Gangrene Cellulitis Physical Exam: Extremities Palpation of Axillary Lymph Nodes Onychomycosis Cellulitis Gangrene Joint Deformity Cyanosis Physical Exam: Musculoskeletal Exam Physical Exam: Neurological Exam • Can be a comprehensive or cursory exam • Major Components – Mental Status – Cranial Nerves – Muscle strength, tone and bulk – Reflexes – Coordination – Sensory Function – Gait Physical Exam: Cranial Nerves • CN 1: Olfactory Sense • CN 2: Visual Acuity • CN 3, 4, 6: Extra-ocular muscle movement • CN 4: Superior Oblique muscle CN 6: Lateral Rectus CN 3: Inferior oblique Inferior rectus, superior rectus, and medial rectus Physical Exam: Cranial Nerves • CN 5 – Motor: Temporalis and Masseter muscles – Sensory • V1: Forehead • V2: Check • V3: Jaw • CN 7 – Most of the facial muscles • CN 8: Acoustic Acuity – Weber – Rinne Physical Exam: Cranial Nerves • CN 9: Glosopharyngeal • CN 10: Vagus • Together CN 9 and 10 raise the soft palate and produce gag reflex Physical Exam: Cranial Nerves • CN 11: Innervates muscles which permit shrugging of shoulders • CN 12: Responsible for tongue movement Physical Exam: Sensory • Spinothalamics: detect pain, temperature, crude touch • Dorsal Columns: detect position, vibratory and light touch Physical Exam: Motor Assessment • Observe muscle bulk • Look for asymmetry between extremities • Examine major muscle groups of upper and lower extremities – – – – – Biceps Triceps Deltoids Quadriceps Hamstrings Motor Assessment • Assessment of muscle strength • 0: No movement • 1: Slight flicker of muscle movement • 2: Can voluntarily move, but cannot overcome gravity • 3: Can overcome gravity, but not applied resistance • 4: Can overcome gravity and some resistance • 5: Normal Follow Up Presentation • 1-2 sentence summary of patient’s presentation and hospital course • Explanation of past 24 hour events • Physical Exam • Important Laboratory and Radiographic Studies • Assessment and Plan Questions You May Be Asked During the Presentation • Etiology of Symptoms • Pathophysiology of Disease • Diagnosis Criteria • Common Complications • Differential Diagnosis • Diagnostic Tests • Treatment Options Miscellaneous Tips • Include only essential facts in your presentation – Be prepared to answer any questions with more detail • Keep the same order and format for all presentations • Be thorough with your differential diagnosis and treatment plan Miscellaneous Tips • Try not read directly off paper • Presentation should be as conversational as possible • Expect questions and be prepared to answer them Conclusions • A tremendous amount of information can be obtained by a properly conducted history and physical • It is important to be an excellent presenter and be able to convey important information to other medical professionals