Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
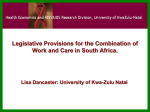
Reflective Presentation Olivia’s Journey Health Roundtable – Maternity Health Improvement Group 2011 Victoria Health Roundtable – Maternity Health Improvement Group 2011 2 Metropolitan Region Health Roundtable – Maternity Health Improvement Group 2011 3 BMI Spread Over 8 Months BMI >30 and Birth type Sum of BabyNum Data from 1/7/2010 to 2/3/2011 BMI BirthType 30 31 32 33 Elective Caesar with Forceps elective caesarean - labour Elective caesarean - no labour 2 1 2 12 11 10 8 1 1 Emergency Caesar with Forceps Emergency caesarean - labour 35 1 1 10 11 7 Emergency caesarean - no labour 2 6 1 3 Forceps 1 1 Normal 54 33 4 1 7 Total with BMI > 30 38 5 39 40 41 42 43 44 45 46 47 48 1 2 1 49 50 51 52 53 55 56 58 60 62 63 Grand Total 1 4 9 7 3 4 5 2 4 4 6 7 4 5 6 6 3 3 2 4 1 2 3 3 1 1 14 15 9 9 1 2 1 36 28 22 2 3 2 1 1 1 1 1 91 9 3 3 38 27 23 4 1 1 27 3 3 3 1 12 10 1 1 4 5 1 3 1 1 1 1 1 1 1 10 13 63 67 50 45 43 104 29 1 18 4 3 3 1 1 2 1 318 1 16 1 88 Total Births for period audited 37 1 Vaginal breech (assisted) Grand Total 36 1 13 Vacuum extraction 34 1 23 22 22 17 17 9 6 8 4 1 8 2 1 1 4 1 1 1 1 1 1 593 2886 593 20% Health Roundtable – Maternity Health Improvement Group 2011 4 Background •Sunshine Hospital is heading towards 4,500 births per year a 26% increase in 18 Months •We have no dedicated high BMI program •Use a case presentation to reflect on how we could improve the client journey at Western Health •Share our deficiencies as a learning opportunity Health Roundtable – Maternity Health Improvement Group 2011 5 Case Study Olivia booked into Sunshine Hospital for confinement of her first baby. The following is a reflection of her journey and the challenges experienced by both Olivia and her Carers. Health Roundtable – Maternity Health Improvement Group 2011 6 Patient History • 28 year old • VSD repaired 09/12 • Obesity since early childhood (8yrs +) • Morbid obesity weight 177kg, height 167cms, BMI 70 • Depression • Smoker – ceased four years ago • Vitamin D deficient Health Roundtable – Maternity Health Improvement Group 2011 7 Patient History • Past Pregnancy/Obstetric – – – – G1 P0 Implanon removed February 2009 Irregular menstrual cycle EDD calculated by 1st trimester USS • Medications – – – Elevit daily Ostelin daily Paracetamol PRN Health Roundtable – Maternity Health Improvement Group 2011 8 Patient History • Surgical – Gastric Lap Banding 2003 • Family History – – – Mental illness – Mother schizophrenic Diabetes High blood pressure • Social – – Lives at home with Husband Fulltime Carer for Mother – terminal cancer Health Roundtable – Maternity Health Improvement Group 2011 9 Patient History • Hb 142 • Ferritin 98 • B12 and Folate NAD • HepB, HepC and HIV negative • GTT at 16 and 27 weeks NAD • Varicella negative • Thalassaemia NAD • Syphilis NAD • Urine MCS negative • 1st trimester screening NAD Health Roundtable – Maternity Health Improvement Group 2011 10 First Antenatal Presentaion • Attended at 13 weeks gestation with CMC • Discussed high BMI and “difficulty with diet due to lap band” – appointment with Bariatric Specialist three weeks time • Referral made to Dietician, Medical OBS and Anaesthetics Department • GTT order 16/40 Health Roundtable – Maternity Health Improvement Group 2011 11 Second Antenatal Appointment • Presentation at 16+6 weeks • Reviewed by Bariatric Specialist – fluid removed from lap band • Medical review attended – ECHO NAD • Dietician review – diet plan • Routine Morphology USS requested 20/40 Health Roundtable – Maternity Health Improvement Group 2011 12 Ultrasound Limitations • USS repeated twice due to incomplete morphology secondary to body habitus • Growth scans booked for 32 and 36 weeks NAD • USS ordered again at 38 weeks due to midwives unable to auscultate FHH • O&G Registrar recommendation for Paed present due to family history of congenital heart defects and limited morphology Health Roundtable – Maternity Health Improvement Group 2011 13 30 Weeks Pregnant • Declined Social Work referral • Declined CBE classes • Numerous appointments DNA (documented drove to Hospital but unable to park within close walking distance) • Support by Palliative Care Services – Mother died • Anaesthetic Team and O&G Medical Team review • Normotensive Health Roundtable – Maternity Health Improvement Group 2011 14 Third Trimester Management • Carpal Tunnel Syndrome symptoms • Ankle Oedema • 38 weeks HT 180/90 – headache, protein urea 2+, oedema, bloods NAD. Commenced Labetolol • Presented 39 weeks with decreased FM • Presented PIH assessment – weekend Birthing Suite midwives unable to detect FHH – USS attended • Planned twice weekly CTG in PDSU • Admitted to Maternity Ward 40 weeks PIH • Non ambulant >38weeks - wheelchair Health Roundtable – Maternity Health Improvement Group 2011 15 41+5 IOL • Admitted to Birthing Suite for IOL due to PIH and post maturity • Prostin 2mg x 2 doses • Documented difficulty with “monitoring fetal heart” • Patient non ambulant • IVC – FBE, E&E, SUA, LFT’s GS • O&G Team aware of IOL • Anaesthetic Team aware of IOL • ARM and Syntocinon commenced following day by O&G Registrar • Midwives unable to accurately assess contractions • Patient requesting “early epidural” • GBS positive HVS @ 36 weeks – antibiotic coverage intrapartum Health Roundtable – Maternity Health Improvement Group 2011 16 Intrapartum • O&G plan “to deliver during the day” • Epidural inserted, but catheter accidentally dislodged by patient • Complaining of palmitations and noted IRR pulse – ECG NAD • Discussed at “O&G handover 0800” • Normotensive intraprtum • Labour duration 7:41mins • Failure to progress • Emergency CS – general anaesthetic – Baby born 1641hrs • Arterial line inserted in OT prior to surgery • Four extra staff in OT to hold abdominal apron • Baby 3780g – Apgars 6 @ 1min and 8 @ 5min • Estimated blood loss 1200ml PPH Health Roundtable – Maternity Health Improvement Group 2011 17 Postpartum Care Plan • Returned to Birthing Suite for 24/24 postpartum for 1:1 midwifery care • Clexane 40mg after 6hrs and then daily until discharge • Routine pain management – Morphine PCA • Pain Management Team • TED Stockings too small • IV antibiotics • Physiotherapy referral • Sleeping in chair • Early mobilisation encouraged but “reluctant” • Social work referral due to grief • Discussed daily at O&G handover 0800hrs • Daily O&G Registrar and Resident RV Health Roundtable – Maternity Health Improvement Group 2011 18 Postpartum Care • Day 5 – – – Discharged home – Clexane ceased Domiciliary Care Breastfeeding • Day 10 – – Complaining of backache – non ambulant, wheelchair dependent Abdominal wound moist – alternate sutures removed with remaining for removal day 14 Health Roundtable – Maternity Health Improvement Group 2011 19 Postpartum Care • Day 16 – – – – – – – – – – Presented A&E – Hx bilateral aching calves and shoulder tip pain Diagnosed Bilateral Pulmonary Embolus and Pleural Effusion Respiratory Consultancy referral Diagnosed Abdominal Wound Infection Blood cultures under USS guidance by Anaesthetist due to numerous failed attempts Ceased breastfeeding Transferred to Respiratory Unit – Footscray Commenced Clexande 120mg Returned to Recovery Room for removal of remaining abdominal sutures Commenced BD wound dressings Health Roundtable – Maternity Health Improvement Group 2011 20 Postpartum Care • Day 16 – – – Commenced oral antibiotics Management plan ICU Liaison Nurse Sleeping in chair • Day 17 – – – Physiotherapy referral Complaining of constant backache, but unaided ambulation Documented weight 200kg Health Roundtable – Maternity Health Improvement Group 2011 21 Postpartum Care • Day 18 – – Occupational Therapy referral Assessment, but nil follow up • Day 19 – Discharge HITH • Day 21 – – Ongoing Physiotherapy referral – offered bariatric crutches to assist with mobility in the community Social Work referral due to grief following death of mother, but nil follow up Health Roundtable – Maternity Health Improvement Group 2011 22 Learnings • Clinical • Systems Health Roundtable – Maternity Health Improvement Group 2011 23 Obstetric Challenges in the Obese Patient