Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Medical ethics wikipedia , lookup
Infection control wikipedia , lookup
Health equity wikipedia , lookup
Rhetoric of health and medicine wikipedia , lookup
Long-term care wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Electronic prescribing wikipedia , lookup
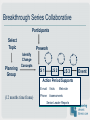
The Health Care Delivery System and Managed Car Health of Populations and Individuals • Delivery system exists within communities • Many other stakeholders with interests – Patients, employers, public health/government, community groups, educational system, payers • Chronic disease affects certain populations disproportionately • Collaboration needed (spectrum of relationships) to improve outcomes and reduce disparities • Collective accountability/responsibility the only answer • “If not us, who? If not now, when?” Disparities: Life Expectancy at Birth Overall White Overall Black 85 without Homicides White without Homicides Black without AIDS White 80 without AIDS Black without Both White without Both Black Years 75 70 65 2001 1999 1997 1995 1993 1991 1989 1987 1985 1983 1981 1979 1977 1975 1973 1971 1969 1967 1964 1962 1960 60 Life Expectancy by Census Tract Alameda County 100 95 Life Expectancy (Years) 90 85 80 75 70 65 60 55 50 0% 10% 20% 30% Pov erty Rate 40% 50% 60% Causes of Differences in Health Outcomes By Race • Genetics* 10-15% • Access to health care 10-15% 15% + 15% = only 30% What causes the other 70%??? *genes ≠ race Medical Model HEALTH CARE ACCESS Socio-Ecological -Bay Area Regional Health Inequities Initiative Expanded Model Chronic Care Model Community Resources and Policies SelfManagement Support Informed, Activated Patient Health System Health Care Organization Delivery System Design Productive Interactions Decision Support Clinical Information Systems Prepared, Proactive Practice Team Functional and Clinical Outcomes Health Care Organization • Quality as core strategy • Visibly support improvement at all levels, starting with senior leaders. • Promote effective improvement strategies aimed at comprehensive system change. • Encourage open and systematic handling of problems. • Provide incentives based on quality of care. • Develop agreements for care coordination. Chronic Care Model Community Resources and Policies SelfManagement Support Informed, Activated Patient Health System Health Care Organization Delivery System Design Productive Interactions Decision Support Clinical Information Systems Prepared, Proactive Practice Team Functional and Clinical Outcomes Delivery System Design • Multiple levels – Regional/National: macrosystem – Integrated Medical Care Organization: mesosystem – Practice level: microsystem • Alignment required for breakthrough improvement in community health Delivery System Design • Define population of patients • Define roles and distribute tasks amongst team members. • Use planned interactions to support evidence-based care. • Provide clinical care management services. • Ensure regular follow-up. • Give care that patients understand and that fits their culture Mesosystem: Practice Environment in Humboldt • 29 primary care practices in various sizes, types and stages of transformation (all in the Humboldt IPA) – 5 community health centers – Many 1-3 clinician practices in private practices (one 17 MD Internal Medicine practice) – No large integrated multispecialty group – Managed care covering 5% of population • How to rapidly improve chronic disease care in the community? Humboldt Diabetes Project • CHCF-funded research project started 11/02 • County-wide effort coordinated by IPA (>95% of all clinicians in the county, including MDs, advanced-practice clinicians, behavioral health providers) but… • IPA manages only 10% of lives in Humboldt County …but systems must apply to most patients in a practice • Problem: – Lack of access to most administrative data • Solution: – Information must come from clinical setting Getting Started • “Burning Platform” to capture hearts and minds (disease focus vs. abstract “redesign”) • Grant support for concept • Clinical champion presenting own data making it safe for others • “Inviting the implementers into the planning process” • Piloting systems • Kick-off conference (including patient voices) • Site champion network supervised by ½-time FNP • Feedback on practice-level and individual performance Humboldt Diabetes Project Clinician Education Patient Education reted Integ ion s D e ci r t o Supp Pat Invo ients lv Self ed In -C a re s a ye r Get P spitals Ho and Play to Registry and Flow Sheet Prompts and Reminders Case Management Buil d an C h r d Ma i n o t Infra nic Ca ain a re stru ctur e N e xt Chronic Diseas e es ct Offic Conne rnet for nte to the I l Clinica nd tion a Informa ication un C o mm DIABETIC PROJECT FLOW DIAGRAM Data from office visit PACES, CHCF chart audits Staged Diabetes Management Guideline Feedback to clinicians yes Pt. enrolled in diabetic study Data entered in registry Monthly audit of data in registry Prompts and reminders Office visit: scheduled, random Services delivered? Registry note returned? Data analysis Patient visit sheet no A1c > 9 Pharmacy data yes Risk stratification Lab data BASICS Case management To improve outcomes in chronic illness… • Patients must be prescribed and taking proven therapies • Patients must be managing their illness well Microsystem: Frustration • Patients are frustrated by waits and discontinuities, often don’t receive proven services and often feel they are not heard. • Providers feel they have little control over their work life, are stressed by demands for productivity despite older, sicker clientele and the reduced variability in their clinical day. Is There Time for Management of Patients With Chronic Diseases in Primary Care? • METHODS – Applied guideline recommendations for 10 common chronic diseases to a panel of 2,500 primary care patients with an age-sex distribution and chronic disease prevalence similar to those of the general population, estimated the minimum physician time required to deliver high-quality care for these conditions. • RESULTS – Top 10 chronic diseases (STABLE) 828 hours per year, or 3.5 hours a day – Top 10 chronic diseases (Poor Control) 2,484 hours, or 10.6 hours a day. • CONCLUSION? What we know about primary care visits • 50-70% are largely informational or informative (including check-backs for chronic illness care) yet they are organized like acute visits • US average is 16.3 minutes • Patients are given an average of 20 seconds to tell their story before they are interrupted How would I recognize a productive interaction? Informed, Activated Patient Productive Interactions Prepared Practice Team •Assessment of self-management skills and confidence as well as clinical status •Tailoring of clinical management by stepped protocol •Collaborative goal-setting and problem-solving resulting in a shared care plan •Active, sustained follow-up Microsystem: Defining roles and tasks across team to achieve productive interactions “It is naïve to bring together a highly diverse group of people and expect that, by calling them a team, they will in fact behave as a team. It is ironic indeed to realize that a football team spends 40 hours a week practicing teamwork for the two hours on Sunday afternoon when their them work really counts. Teams in organizations seldom spend two hours per year practicing when their ability to function as team counts 40 hours per week." Harold Wise, Making Health Teams Work Team Meetings • Regular intervals • All members of care team (groups of < 10) • Agenda: – Old business – New Business – What isn’t working? – Opportunities for excellence? Defining Tasks Example of task distribution Microalbuminuria testing • Receptionist recognizes patient has diabetes, attaches requisition to chart • MA collects specimen • RN reviews slip, recognizes out-of-range tests, orders confirmatory test, discusses possible need for ACE inhibitor • MD discusses and prescribes ACE inhibitor • RN calls pt. to check on med. adherence and side effects Use planned interactions to support evidence-based care One-on-one, group, telephone, email, outreach….the possibilities are endless What is a Planned Visit? • A Planned Visit is an encounter with the patient initiated by the practice to focus on aspects of care that typically are not delivered during an acute care visit. • Planned care elements can be inserted into acute visits if needed (small practices, patients refusing to come in for planned care, etc.) • All visits contain elements of both (patient agenda/clinician agenda) • The more planned care functions done by other members of the team, the more time for the patient agenda in the exam room (improves clinician-patient relationship, higher patient satisfaction) What does a Planned Visit look like? • The provider team proactively calls in patients for a longer visit (individual or group) to systematically review care priorities. • Visits occur at regular intervals as determined by provider and patient. • Team members have clear roles and tasks. • Delivery of clinical management and patient self-management support are the key aspects of care. How do you do a Planned Visit? You Plan It! Example: Diabetes • Choose a patient sub-population, e.g., all patients with diabetes not seen in 6 months with A1c > 7 • Identify patients from registry • MD reviews list for patients at highest risk (via evidence-based guidelines): BP>130/80; LDL>100, etc and prioritizes visits Patient Outreach • Have receptionist or provider call patient and explain the need for planned visit using script explaining different nature of visit • Personal appeal by clinician works best • Ask patient to bring in bag of all medications they are taking (including OTCs and herbals) Preparing for the Visit • “Team Huddle” at start of clinic session • RN/LPN/MA prints any relevant patient summaries from registries and attaches to front of chart • MD reviews medications/labs prior to visit REGISTRY FLOW OFFICEVISITS Planned Visit Chart visit in normal fashion Prep chart no Registry Patient? yes Download most recent Progress Note Place PN on front of chart Medical Assistant tells patient: “Take off your shoes” Progress Note employed in visit Pull chart Progress Note returned to office staff Patient Info sheet sent to patient Walk-in Visit Updated Progress Note faxed to office and placed on Registry web-site IPA updates registry Progress Note faxed to IPA The Visit • Ask patient open-ended questions – “How’s your health? Any issues you want to discuss? • Review patient’s data • Identify interventions, labs, referrals and selfmanagement needs • Problem solve adherence/other issues with patient • Create an patient action plan (if indicated) • Schedule follow-up Group Visits: Introduction • Fun and efficient • Patients can receive: Self-management support training Social support Specialty service as needed/available One-on-one with medical provider Medication counseling • Multiple models for Group Visit agendas: open-ended vs. curriculum-based; single disease vs. multiple; newly diagnosed vs. range of experience; professional vs. peer-led Patient Survey: Less Frustrated? In general, would you say your health is: (check one box) B F : Excellent Very Good Good Fair Poor 4% 19% 37% 30% 10% 5% 27% 42% 22% 4% How effective do you believe your health care provider is in managing your diabetes? Not effective at all Not very effective Somewhat effective Effective Very effective B 1% 3% 18% 45% 34% F <1% 1% 13% 44% 41% Clinician Survey: Less Overwhelmed? How effective do you believe you are in caring for your diabetic patients? Not effective at all Not very effective Somewhat effective Effective Very effective Baseline - 3% 32% 57% 8% F/U - 27% 56% 17% - Compared to a year ago, how effective are you in caring for your diabetic patients? Less effective F/U - Somewhat less effective Somewhat more effective Same - 27% 41% Note: The sum of the categories may not add to 100% due to rounding. More effective 33% What is care management? Many different things to different people • Resource coordination • Utilization management • Follow-up • Patient education • Clinical management Features of effective care management • Regularly assess disease control, adherence, and self-management status • Either adjust treatment (best practice) or communicate need to physician immediately (less effective) • Provide self-management support • Provide more intense follow-up • Assist with navigation through the health care process Effect of Group SMS on HbA1c Group SMS (Basics) vs. Control and Sustainability 7.80 7.60 7.40 7.20 7.00 Pr e Ba sic No s v0 De 5 c0 Ja 5 n0 Fe 6 b0 M 6 ar -0 Ap 6 r-0 M 6 ay -0 Ju 6 n0 Ju 6 l-0 Au 6 g0 Se 6 p06 6.80 Basics Oct 05 Grads(n=135) non Basics (n=3400+) Ensure regular follow-up by the primary care team •The trick is noticing when it isn’t happening •Can be accomplished in many different ways Humboldt Diabetes Project Data Measure October, 2003 October, 2004 January, 2007 Results Results Results (n=802) (n=778) (n=4330) 5.2% HbA1c control: >9% (poor control) 7.7% 6.9% HbA1c control: <7% (good control) 52% 55% Patients with BP <140/90 62% 59% 59% 67% Patients with BP <130/80 32% 33% 37% Patients with LDL<130 60% 73% 78% Patients with LDL <100 32% 44% 49% New Methods for Teaching the Chronic Care Model IHI National Forum December 10, 2007 Breakthrough Series Collaborative Participants Select Topic Planning Group Prework Identify Change Concepts P A P D A S LS 1 P D A S LS 2 D S LS 3 Action Period Supports (12 months time frame) E-mail Visits Web-site Phone Assessments Senior Leader Reports Event Experience with Collaboratives • More than 1,000 different health care organizations and various diseases involved to date • Began with national BTS, now regional, state-based & facility specific • HRSA’s Health Disparities Collaboratives600+ community and migrant health centers, now academic medical centers & small practices • External evaluations of early efforts by Chin et al., RAND Lessons Learned from the Teams • Teams spent considerable time searching for/developing tools • Some teams felt intimidated by taking on the whole model – asked for a sequence • Collaboratives were time & resource intensive • Many changes were made in ways that were not sustainable financially Challenges Remaining Reaching beyond early adopters Try less timeintensive learning Target small practices Create supportive systems Trying New Ideas • Virtual • Collaboratives On Wheels • Coaching • Combos Integrating Chronic Care and Business Strategies in the Safety Net The Intervention Practice Coach _________________ STEP-UP Methodology PLUS Toolkit ______________ Business & Clinical Tools The Toolkit Sequence Getting Started Organize Your Improvement Team Familiarize Team With Strategies Use Data To Set Priorities Assess Data & Set Priorities Select Performance Measures Build Measurement Capacity Redesign Care and Business Systems Organize YourYour Care Team Organize Care Team Clearly Define PatientPatient Panels Clearly Define Panels Create Infrastructure Support Pts Create Infrastructure To Support Patients Plan Care Plan Care Support Self-Management Assure Support For Self-Management Improve & Sustain Changes • Integrated CCM & Business Changes Reexamine Outcomes & Adjust Reexamine Outcomes & Make Adjustments Capture Incentives • Organized into four phases The Toolkit Business CaseCase The Toolkit&&theThe Business Coaching Outline Tasks Philosophy Assessment Day Focus on motivation, consultation & education ½ day presentation on CCM & PDSA On-going meetings by phone, email & in-person Coaching of the leaders & the teams Be mindful of the timing of interventions Fix processes relevant to the task at hand Well-structured & supported groups benefit most CCM Developments • Guides several state programs • Adaptations undertaken by European countries, World Health Organization, and several Canadian provinces. • Foundation for NCQA and JCAHO certification for chronic disease programs. • Part of new Patient-centered Medical Home Models of Primary Care proposed by AAFP, ACP, AAP, AOA. • Several practice assessment tools now available for large and small practices. • Assessments now used in some pay for performance programs (NCQA). Challenges Remaining Early Adopters Try less timeintensive learning Target small practices Create supportive systems What will it Take to Improve Care for Chronic Illness for the Population? Three Options When Selecting a Strategy 1. Assume that competition, financial incentives and computers will improve care. 2. Rely on direct to patient disease management. 3. Improve medical care by helping practices change care systems. What can we learn from successful larger health systems? Organizational factors supportive of high quality chronic care: • Strategic values and leadership support long-term investment in managing chronic diseases • Well-aligned goals between physicians and corporate managers • Investment in information technology systems and other infrastructure to support chronic care • Use of performance measures and financial incentives to shape clinical behavior • Active programs of Quality Improvement based on explicit models BMJ 2004;328:223-225 What’s needed to improve chronic illness care for the population? Build a regional healthcare “system” • Collaboration and Leadership • Measurement (& incentives) • Infrastructure • Active program of practice change •Care will not improve unless we change the systems of care •The goal is to transform health care delivery across a region Leadership •Someone needs to take and then assure leadership •Major stakeholders need to be involved and committed to improvement •Need outcome and patient experience data as well as process data to assess effort, performance, and improvement •Practices will have to be able to provide valid and complete data on these indicators; claims will not suffice •Practices should be able to use these data in clinical care, not just periodically send them off •Smaller practices need info. and technical support to develop such data systems •Need strategies and infrastructure to help ALL practices change their delivery systems •Strategies – QI methods, Provider networks •Infrastructure—IT, guidelines, care managers •More activated and informed consumers may help push improvement •Public disclosure of performance data may spur improvement •Create incentives for providers to make the investments needed to improve chronic care •Create benefit plans that reward consumers for making costeffective choices A Framework for Regional Quality Improvement Leadership Is geographic improvement possible? State efforts Is geographic improvement possible? Indiana • Health Commissioner and Medicaid Director to improve care for 80,000 chronically ill Medicaid recipients • State leadership and money creating a Medicaid care system • Statewide Collaborative Program PLUS -call center -community-based nurse care managers linked to practices -statewide Web-based patient registry -registry updated with claims data -considering performance incentives -embedded RCT • Reported cost-savings to the Governor Is geographic improvement possible? North Carolina • State leadership and money has created a visionary Medicaid care system • Measurement system, Guidelines, Physician networks, Care Managers, Collaboratives • Financial rewards for participating • Early results promising • Plans to extend to include all patients regardless of insurance coverage Is geographic improvement possible? Washington State •Diabetes Surveillance •Regional Collaboratives •Laid groundwork for PSHA Is geographic improvement possible? Pennsylvania •Governor brought disparate interests together •All the major players at the table •Timeline & ?budget to make it happen Lessons Learned Indiana Make your effort bipartisan & protect it from political winds. North Carolina Reach out! Provider networks can engage small practices in quality improvement Rhode Island Bring all the “p”s to the table: providers, purchasers, payers, patients, policy-makers Colorado Connect with local foundations and groups already doing the work Washington/ Political leadership involvement can be Penn. critical catalyst Maine/ California Organizing diffuse efforts is a big but important job