Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
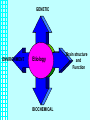
Schizophrenia all rights reserve Austin Community College Psychosis • A Symptom • Affects ability to perceive and process information. • Behaviors associated with psychosis are often severe, long-lasting and difficult to understand. • Goal is patient recognition of symptoms and development of strategies to manage symptoms resulting in stabilization. Schizophrenia • • A serious persistent neurological brain disorder: the exact cause is unclear Theories of causation include – • genetics, biochemistry, and psychosocial factors 1. Age of onset 2. Role of Stress 3. Need for dopamine agonist (medication) Symptoms vary greatly among different patients depending on the area of the brain effected. – Psychosis: the individual is not able to distinguish the external world from internally generated perceptions. • Treatment varies to meet individual needs – Includes: • • • psychotropic medications education social support BIOCHEMICAL • Dopamine overwhelms the brain and binds with too many receptors – Research has been unable to determine if this is due to: 1. Higher levels of dopamine 2. Increased sensitivity to dopamine • Ratio between serotonin and dopamine – atypical anti-psychotics effect serotonin also. • Endogenous dopamine is an antagonist is GABA – Relatively high levels of dopamine result in ANXIETY • Can you induce psychosis? – Marijuana, LSD, Amphetamines – How do these affect dopamine GENETIC ENVIRONMENT Etiology BIOCHEMICAL Brain structure and Function GENETICS • Probability of Schizophrenia in Families – – – – – 1 parent 10% probability 1 sibling 10% Identical twin 50% Both parents varies 40% A gene identified ---research continues Review of Neurobioloby • Frontal lobes – The executive; decision maker, reliant on other parts of the brain for data. Prefrontal is the personality • Temporal Lobes – Hearing • Parietal Lobes – Perception, interpertation touch body perception • Occipital Lobes – Sight Schizophrenia and Neurotransmitters • Overactive dopaminergic pathways in the mesolimbic (innervates the limbic system) system • Important in reaction to stress • Hypofunction in the prefrontal areas and an imbalance between dopamine and serotonin BRAIN STRUCTURE AND FUNCTION PET SCAN ILLUSTRATES FUNCTIONAL DIFFERENCES IN THE LIVING BRAIN PET Scan and Schizophrenia MRI Comparing Identical Twins: One without Schizophrenia and One with Schizophrenia • When the ventricles are enlarged the brain has lost mass (VBR Ventricular Brain Ratio) ENVIRONMENTAL • • • • Inherited susceptibility to schizophrenia Prenatal infections Poor Family Communication Greater % of patients come from lower socio-economic class • STRESS • What about prevention? Incidence and Prognosis • In all societies, occurs in 1% of population with slightly higher incidence in males • Prognosis: approx. 25% remain highly functional • 50% remain non-functional • 25% are in-between, in and out of hospital • Age of onset is late adolescence/ early adulthood Prognosis • Acute phase – Severe psychotic symptoms • Stabilizing phase – Patient is getting better • Stable phase – May still have hallucinations and delusions – Not as severe • Most patients alternate between acute and stable phases STRESS: Onset or Relapse • Biological (medical illness) – People with schizophrenia: • Can misperceive physical symptoms • Have poor pain recognition • Leads to neglect by health care providers • Psychological (loss of a relationship) • Sociocultural (homeless) • Emotional (persistent criticism) • Identification of symptoms and early triggers Bleuler’s 4 A’s • Affective Disturbance: – Inappropriate, blunted or flattened • Autistic Thinking: – Preoccupation with the self – Little concern for external reality • Associative Looseness – Stringing together of unrelated topics • Ambivalence – Simultaneously opposing feelings Positive symptoms of Schizophrenia • Positive Symptoms (+) Person with schizophrenia does more (+) than Person who is functioning normally – – – – – agitation/aggression delusions hallucinations formal thought disorder:loose associations, word salad bizarre behavior – Disorganized Speech (loose associations and word salad) – Grossly disorganized or catatonic behavior • Typical Anti-psychotic medications control these symptoms Negative symptoms of Schizophrenia • Negative Symptoms (-) Person with schizophrenia does less (-) than Person who is functioning normally • Atypical antipsychotics will help these symptoms • Typical antipsychotics can make these worse – flat affect – avolition; lack of direction or purpose – ambivalence; – indecisive – constricted – concrete thinking – alogia: poverty of speech – social withdrawal – anhedonia – deep apathy – minimal or poor self care Schizophrenia Subtypes • Paranoid • Catatonic • Disorganized • Undifferentiated • Residual Paranoid • Preoccupation with: 1. Delusions • Persecutory /Paranoid • Grandiose 2. Hallucinations • Command • Auditory 3. No disorganized speech Usually neat and clean. 4. Issues for Nursing care – Fearful-mistrusting – Aware of authority • Can be VERY dangerous to others and self. Can get themselves into situation where they think they are protecting themselves and they get themselves killed. Catatonic – Stupor – Negativism – Rigidity – Posturing: waxy flexibility Characteristics of Catatonic Patient • • • • • Acute onset, often in response to stress Rigid, weird positions Waxy flexibility May not eat-often very angry Good prognosis • What are the Nursing Interventions for someone who is not eating and stays in the same position for many hours? Disorganized – Disorganized speech – Disorganized behavior – Flat or inappropriate affect – Disheveled appearance Undifferentiated – Positive symptoms – Does not meet criteria for: • Paranoid Schizophrenia Residual – No positive symptoms – Mostly negative symptoms – Chronic Other Psychotic Disorders – Psychotic Disorder NOS – Delusional Paranoid Disorder – Schizophreniform Disorder • Symptoms of schizophrenia last one month but no longer than six months – Schizoaffective disorder • A puzzle • Characterized by: – Symptoms schizophrenia are dominant – Accompanied by major depressive or manic symptoms Nursing Diagnosis for Schizophrenia • • Altered thought processes: Delusions Sensory/perceptual alterations: specify Hallucination Social isolation Potential for violence Self-care deficit Impaired verbal communication Sleep pattern disturbance Altered nutrition Impaired home maintenance management Related to: Neuro chemical imbalance; Disturbed thought process; Auditory Hallucinations Secondary to: Schizophrenia Treatment • Antipsychotic Medication • Supportive Psychotherapy and Education – – – – Individual Group Milieu Family • Social supports – – – – Follow-up mental health care/Medication Housing Day treatment Employment Therapeutic Relationship • TRUST – Be honest; do what you say. • Do not be too warm and friendly – – – – – Be consistent and honest Be careful with touch AND eye contact At first, may need to just “be there” or “offering self Don’t expect too much of yourself or the patient Improvement happens slowly Therapeutic Communication for Hallucinations • • • • • Ask “Are you hearing voices?” Ask “What are they saying?” May want to know for safety reasons. Ask “What are they like, are they loud, or male or female.” Can ask patient “What helps you with the voices” Can state,” I know they distract you, but can you focus with me for a minute.” • Patient may miss voices after they are gone. Elements of the Effective Milieu 1. Safety (examples) Psychological and physical Restraint and seclusion No contraband (cans, glass, lighters) 2. Structure (examples) Unit schedules, meals, bedtime Groups Visiting hours 3. Norms (examples) Individual responsibility Rules 4. Limit setting (examples) cannot harm self or others; cannot smoke 5. Balance (examples) Rights of one person to talk loud –VS- rights of others to quiet Nursing judgment and critical thinking Environmental Modification- bending rules when necessary to be therapeutic. Milieu: Therapeutic Manipulation of the Environment • Disruptive Patients – Set limits – Decrease environmental stimuli – Frequent observation • Early intervention • Verbal intervention so physical intervention is not needed – Safety • Who will work with the patient? – No threats • (If you……then) • • Suspicious Patients – Matter of Fact – No laughing or whispering – Proximics • Approach form the side • Avoid close physical contact – Eye contact Withdrawn Patients – Non threatening activities – Provide a connection with reality – Give support • Decision making • Hygiene Milieu: Therapeutic Manipulation of the Environment • Impaired Communication – Protect self-esteem • Activities where success is assured – Provide support • Connection – Patience – No pressure • Disorganized – Decreased stimulation – Provide a calm environment – Safe and simple activities • Rely on long term memory • Hallucinations – Engage in activities – Attempt to separate patients who have similar psychotic thoughts – Connection to reality • Talk about real people and real events – Monitor television – monitor for command hallucinations Consistency in the Milieu • Do not argue • Do not belittle • Show acceptance and empathy and speak to them “That must be difficult to believe that.” • Do not patronize • Can reassure- “You are safe here.” • Orient patient to what is happening Nursing Care • • Give information in a kind matter-of-fact – Thoughts provide a sense of identity • Pay attention to key words – Speech represents cognitive functioning – Identify one or two verbal or non-verbal responses. • • Seek Validation Assist with decision making (in the here and now) in a nonpunitive supportive manner – Initiation and completion of tasks The client – Is sleeping 2 hours a night – Will not eat – Has poor hygiene – Is afraid of another client – Does not like their doctor – Wants to stay in their room – States they are on a special mission to save the United States Psychosis-Induced Polydipsia • • • Compulsive water drinking (6% to 20%) Thirst and Osmotic dysregulation Hyponatremia – – – – – – – • Confusion Convulsions Coma Lightheadedness Nausea and vomiting Weakness Muscle Cramps Treatment – – – – Weigh Restrict fluid Sodium replacement Constant supervision Antipsychotic Medications • Typical – Rarely a scheduled medication – Acute phase: controls positive symptoms – Identification and treatment of side effects • Atypical (97%) Four Major Dopaminergic Tracts • 1. Nigrostriatial (movement) • 2. Tuberinfundibular (pituitary; elevation in prolactin) • 3. Mesolimbic (emotion and sensory) • 4. Mesocortical (cognitive processes) Typical Antipsychotics • High Potency Neuroleptic – Haldol (Haloperidol) – Prolixin (Fluphenazine) – Available in pills, liquid, Intramuscular and Depo (decanoate) injection • Low Potency Neuroleptic – Thorazine (Chlorpromazine) – Mellaril (Thiroidazine) • In-betweens – Stelazine – Trilafon – Navane Antiparkinsonian Agents • • • • Cogentin (benztropine) Artane (trihexyphenidyl) Benadryl (diphenhydramine) Symetrel (amantadine) • Ativan (Lorazepam) Acetylcholine and Dopamine • A balance between dopamine and acetylcholine is required for normal movement • Antipsychotic medication decrease dopamine, causing EPS symptoms • Antiparkinsonian meds act by decreasing ACH, thus restoring balance • All antiparkinsonian meds increase the anticholenergic effects Side effects of Typical Antipsychotic • Extrapyramidal Side Effects (EPSE) – Acute Dystonia – Akathisia – (Psuedo)Parkinsonism – Tardive Dyskinesia • Anticholenergic effects – – – – – – Drowsiness Dry mouth Skin reactions, sunburn Constipation Urinary retention Orthostatic hypotension Acute Dystonia • Oculogyric Crises – Early onset – Abnormal posture – Involuntary, sustained, muscle spas – Sustained twisted contracted positioning of the limbs, trunk, neck or mouth – This is PAINFUL – Treated with parenteral anticholinergics due to the gravity of the situation • Torticolis Akathisia • “Ants in the pants” • Subjective feeling of restlessness • Nervous energy • Most common EPSE (Psuedo)Parkinsonism • Tremor at rest • Pill rolling • Muscle rigidity • Bradykinesia Stiff, shuffling gait Tardive Dyskinesia – Involuntary movements, – Especially of the face and tongue – IRREVERSIBLE if not corrected immediately – LONG TERM USE OF TYPICAL ANTIPSYCHOTIC Tardive Dyskinesia Neuroleptic Malignant Syndrome • Syndrome is very RARE but can be LETHAL – 1% of patients taking antipsychotics – 5% to 20% will die without treatment • Predisposing factors; – Youth – male – high potency neuroleptic – new patient Cardinal symptoms – Lead pipe rigidity – Autonomic instability • High fever • Tachycardia LOC changes Elevated CPK • • • Neuroleptic Malignant Syndrome (Malignant Hyperthermia) • • • • Medical emergency STOP all medication may resume meds after crisis. Rx: Dantrolene (Dantrium): skeletal muscle relaxant and Bromocriptine (Parlodel): a dopamine agonist Atypical Antipsychotics • • Clozaril (Clozapine) Risperidal (Resperidone) – Invega (Palperidone) • • • Zyprexa (Olanzapine) Seroquel (Quetiapine) Geodon (Ziprasidone) • Novel Antipsychotic • Abilify (Aripiprazole) Atypical Antipsychotics • Decease both Positive and Negative symptoms – Keep dopamine available in some areas (frontal lobe and cortex) of the brain while blocking the effects of dopamine in others. – Increase availability of Serotonin • Very little risk of Tardive Dyskinesia and Extrapyramidal Side Effects Clozaril (Clozapine) • • • • • • • • Atypical antipsychotic Decreases negative symptoms of schizophrenia No Extrapyramidal symptoms (EPS) May decrease symptoms of tardive dyskinesia Effects both dopamine and serotonin Side effects: drowsiness and drooling Expensive Side effects – Agranulocytosis, weekly blood draws – Sedation, excessive salivation, dizziness, seizures – Hyperglycemia/Wt. Gain, Type 2 DM Risperidal (Resperidone) • • • • Atypical; effects serotonin and dopamine. 1st line; effects both positive & negative symptoms Can cause EPS, but lower incidence Side effects: CNS, drowsiness (most common, given at night) • Insomnia agitation, headache, anxiety --Orthostatic hypotension Hyperglycemia • GI: Constipation, nausea, vomiting and dyspepsia • Available in long lasting IM form (2weeks) Invega (Palperidone) • Available in extended release • A metabolite of Resperidone • Similar profile to Resperidone Zyprexa (Olanzapine) • Positive and negative symptoms • Side effects: Drowsiness, constipation, dry mouth, headache. Rare EPS, NMS, • Effects both serotonin and dopamine • Weight Gain long term/Hyperglycemia/ • Type 2 DM • Available in short acting IM form and ZYDES Seroquel (Quetiapine) • • • • • • Atypical antipsychotic, low potency Effective in positive and negative symptoms EPS profile same as placebo No increase in prolactin levels No sexual dysfunction problems Side effects: somnolence and hypotension • Available in IM injection Ziprasidone (Geodon) • Geodon/Atypical Antipsychotic-Antagonizes Dopamine and Sertonin/ • Low EPS • No increase in prolactin levels • Side effects-somnolence in short term and insomnia in long term use • Weight Gain neutral • Big issue-prolongs the QT interval • Patient cannot have any cardiac or electrolyte imbalance • Monitor serum potassium and magnesium • Available in short acting IM form (Aripiprazole ) Abilify NOVEL ANTIPSYCHOTIC • Atypical antipsychotic, effects both dopamine and serotonin, antagonizing some receptors and serving as a partial agonist for others • Decrease in the EPS side effects and minimal Wt. Gain, minimal sedation, no problems with QT interval • Side effects: headache, Anxiety, Insomnia, somnolence, occasional stomach upset • Akathisia Education • Teach about the importance of: – – – – Stay on Medication Keep stress down Seek help if symptoms exacerbate Avoid use of drugs or alcohol Community Supports • Austin Travis County Integral care – http://www.integralcare.org • Palidin Community Mental Health Center – http://www.paladincmhc.com • Capital Area Counicling – http://camhc.org • National Alliance for the Mentally Ill (NAMI)