Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
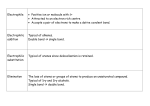
سبحان الذى هدانا و ما كنا لنهتدى لوال أن هدانا هللا Initial Assessment and Management ( ACS – COT ) Presented by Dr. M. Essam El Gammal (MSEM – MACEP ) In 1977 Male, 29 years old, involved in Bus turn over conscious, oriented, complaining of chest pain. Innocent chest wound, mild surgical emphysema. Dx # Rib Sudden death in Emergency Surgical Ward In 1984 Male 48 years old, MVA with multiple facial laceration conscious, oriented, complaining of chest pain. Respiratory distress, multiple # ribs Died in X-ray Department. In 1991 Child 4 years old with laceration above his right eyebrow. ALS, ACLS, ATLS, APLS Simple Safe Systematic RESUSCITATION How You Can Do It Clinical Skills: How to Diagnose (Dx) A - airway obstruction B - tension pneumothorax, sucking chest wound, flail chest C - cardiac tamponade, cardiac contusion, shock D – diagnostic: x-ray, U/S, ABG, ECG TECHNICAL SKILLS: How to Treat (Rx) A - B- CDE- Airway + C Spine stabilization ET intubation Crico thyrodotomy B.V.M. ventilation or IMV Needle thoracocentesis Intercostal tube insertion Canulation peripheral venous, central venous catheters urinary, NG DpL U/S bedside- FAST Extremities fixation (#) Initial Assessment and Management To have a systematic approach for the management of multiple trauma patients . To know how to identify and manage life threatening conditions . To know when and what diagnostic procedures you need . To know how to transfer the patients to definitive care Initial Assessment and Management Pre Hospital Phase :1. Airway – C spine 2. Immobilization 3. Control of bleeding 4. IV line 5. Immediate appropriate transfer Initial Assessment and Management Inter Hospital Phase :1. Policy and Procedures 2. Equipments 3. Recourses Lab., X-ray, BB., OR, Initial Assessment and Management Triage Sorting patients out according to priorities and capabilities . 1. Multiple casualties: Patient no. = capabilities 2. Mass casualties: patient no. > capabilities In this situation you treat those with best survival chances with the need of least time and supplies (1) 1ry. Survey and Resuscitation (3) Reevaluation ABCDE • Adjuncts to 1ry. Survey (2) 2ry. Survey (4) Definitive care Head to toe examination Tubes and fingers in every orifice • Adjuncts to 2ry. survey (5) Transfer Initial Assessment and Management 1ry. Survey and Resuscitation Identify and treat life threatening conditions A Air way + C spine protection B Breathing + Ventilation C Circulation + Control of Hemorrhage D Disabilities ( Neurologic evaluation ) E Exposure + Environmental control Initial Assessment and Management 1ry. Survey and Resuscitation Rule 1: Once A B C problem is identified it should be corrected Rule 2: Many of these activities can occur in parallel or simultaneously Rule 3: Priorities are the same for pediatric patient, pregnant and elderly are the same with special consideration Initial Assessment and Management 1ry. Survey and Resuscitation A Air way + C spine protection • Signs and causes of air way obstruction • Methods to open the air way • air way protection is needed when GCS<8 • In line stabilization of C spine : •Multi system trauma with altered LOC •Blunt trauma above the clavicle Rule 1: Frequently evaluate the air way Rule 2: Definitive air way is indicated if there is doubt Initial Assessment and Management 1ry. Survey and Resuscitation A Air way + C spine protection Pitfalls • Obese short neck patient • ET tube in patient with incomplete upper air way transection or laryngeal fracture • Inability to intubate after paralysis • Equipment failure Initial Assessment and Management 1ry. Survey and Resuscitation B Breathing and Ventilation 1. Expose the chest and Asses RR, R depth and Type 2. Give oxygen 3. Check chest wall, lungs and diaphragm by inspection , palpation, percussion and auscultation 4. Pulse oximeter 5. Identify and treat: Tension Pneumothorax Open Pneumothorax Flail chest Massive Hemothorax 6. Needs for assisted ventilation Initial Assessment and Management 1ry. Survey and Resuscitation B Breathing and Ventilation Rule 1: CXR is needed after intubation and ventilation, but not to diagnose Tension Pneumothorax Pitfalls • Differentiation of ventilation problems from air way obstruction may be difficult • Intubation of Pneumothorax patient with ventilation may result in further deterioration of the patient Initial Assessment and Management 1ry. Survey and Resuscitation C Circulation with Hemorrhage control • Blood Volume and Cardiac output assessment depend on level of consciousness, skin color and the pulse • Start X2 I.V. lines, draw blood samples ( Central line ? ) • Identify the need of blood transfusion • Control Bleeding: Direct pressure on the wound Pneumatic splinting devices No Tourniquet except in amputation •Identify occult blood loss •Assess for the need of operative intervention Initial Assessment and Management 1ry. Survey and Resuscitation C Circulation with Hemorrhage control Pitfalls • P.R., ABP has little correlation with cardiac output in older patients • Children show few signs of hypovolemia • Use of medications affect the response to hypovolemia Initial Assessment and Management 1ry. Survey and Resuscitation D Disabilities (Neurologic Evaluation) Level of consciousness L.O.C. A alert V to verbal stimuli P to painful stimuli U unresponsive Pupils size and reaction Initial Assessment and Management 1ry. Survey and Resuscitation D Disabilities (Neurologic Evaluation) Rule: Depressed L.O.C: may be due to decreased Cerebral Oxygenation , Brian injury or Drugs Pitfalls • Lucid interval commonly occur with Acute Epidural Hematoma ( Talk and die ), this emphasizes the need for frequent Neurologic Re-evaluation Initial Assessment and Management 1ry. Survey and Resuscitation E Exposure / Environmental control • Undress completely ( use trauma scissor ) • Prevent hypothermia ( warm blanket, room temp. ) • Warm I.V. fluids and blood Pitfalls • Early control of hemorrhage will minimize hypothermia Initial Assessment and Management 1ry. Survey and Resuscitation: SUMMARY A Air way obstruction + C-spine stabilization B C Breathing problems: Tension Pneumothorax, Open Pneumothorax Circulation: Shock, Cardiac tamponade. D Disabilities: AVPU, Pupils E Exposure / Environmental control Initial Assessment and Management ADJUNCTS to 1ry. Survey and Resuscitation 1 ECG monitoring 2 Urinary and Gastric Catheters 3 Monitoring: RR, ABG, Pulse Oximetry, ABP, PR,Urine O/P, Temp.,CVP / JV 4 X-ray and diagnostic: CXR, Pelvis, Lat. C-spine and Diagnostic peritonel Lavage and abdominal ultra sound CONSIDER Need for patient transfer Initial Assessment and Management 2ry. Survey 1 Complete History 2 Head to toe examination 3 Re-assessment of vital signs 4 Complete neurological examination GCS. 5 Special procedures, Specific X-rays and laboratory studied Initial Assessment and Management 2ry. Survey 1 Complete History A allergies M medications P past illness / pregnancy L last meal E events / environment / mechanism of injury:blunt, penetrating, burn, hazardous environment Initial Assessment and Management 2ry. Survey 2 Head to toe examination 1. Head, Maxillofacial, Cspine and Neck 2. Chest 3. Abdomen 4. Perineum / Rectum / Vagina 5. Musclockeletal / Pelvis / Back 6. Neurologic evaluation Initial Assessment and Management 2ry. Survey 3 Re-assessment of vital signs Objectives: 1. Identify new Clinical findings 2. Discover deterioration 3. Assure that life threatening injuries are managed 4. Diagnose underlying medical problems Initial Assessment and Management 2ry. Survey 3 Re-assessment of vital signs Done by: 1. Clinical Reassessment 2. Monitoring of LOC, PR, Urine O/P, ABP, ABG, CVP 3. Review of Diagnostic results 4. Use of Analgesia Initial Assessment and Management 2ry. Survey 4 Complete neurological examination GCS. • LOC / GCS • Pupils Complete neurological examination GCS. • Laterilization • Deterioration of LOC / GCS Initial Assessment and Management 2ry. Survey 5 Special procedures, Specific X-rays and laboratory studied • Additional X-rays Extremities, Spine • CT • Contrast X-rays, Urography, Angiography • Endoscopy Not till the patient is stable Initial Assessment and Management 2ry. Survey 1 Complete History 2 Head to toe examination 3 Re-assessment of vital signs 4 Complete neurological examination GCS. 5 Special procedures, Specific X-rays and laboratory studied Initial Assessment and Management Definitive care According to the clinical and other data the patient will be taken to OR, ICU or others Initial Assessment and Management Transfer To other facility according to the patient need and the institution’s capability (1) 1ry. Survey and Resuscitation (3) Reevaluation ABCDE • Adjuncts to 1ry. Survey (2) 2ry. Survey (4) Definitive care Head to toe examination Tubes and fingers in every orifice • Adjuncts to 2ry. survey (5) Transfer