Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
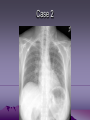
EM Clerkship: Dyspnea David Carlbom, MD Martin Makela, MD Objectives • Discuss approach to patient with dyspnea • Review differential diagnosis • Develop an understanding of the diagnosis and management of common and serious causes of dyspnea Background • Dyspnea: An uncomfortable sensation of breathlessness • Among the most common complaints of patients presenting to ED • May indicate a variety of underlying diseases, from non-urgent to life threatening General Approach • Approach all patients with dyspnea as having a serious cause until proven otherwise • H&P, diagnostic testing and treatment should proceed in parallel given range of possible conditions • Immediate visualization and rapid evaluation • Stabilize and treat prior to full evaluation Diag. Treat Primary Survey Working Dx Life-Saving Therapy Dx Plan Definitive Therapy General Approach • Primary Survey: ABCs & Vital Signs – Correct & support life-threatening issues • IV access, O2, Monitor • ECG • Lab – Electrolytes, CBC, Cardiac enzymes – Possibly D-dimer, BNP, ABG • CXR • Peak Flow if asthma or COPD History • Onset • Associated symptoms – Fever, cough, chest pain, edema, hives • • • • Aggravating/Alleviating factors Similarity to prior episodes PMH Medications Physical exam • Vitals • General appearance/color • Assess for respiratory distress – Accessory muscle use/retractions – Ability to speak full sentences (or not) • • • • Lungs Heart Extremities Abdomen Differential Diagnosis • What are serious causes of dyspnea? – – – – – – – – – PE PNA CHF ACS Asthma/COPD Anaphylaxis Pneumothorax/hemothorax Arrhythmia Airway obstruction Differential Diagnosis • What are other causes of dyspnea? – – – – – – Anxiety Anemia URI Pericarditis Pleural effusion Abdominal distention • Ascites • Pregnancy – Aspiration/chemical exposure – Acidosis – Neuromuscular weakness Case 1 • • • • 35yo F with h/o asthma c/o SOB No relief from repeated albuterol use VS 36.8 112 128/76 28 97%RA Appears uncomfortable, speaking 3 word sentences • Lungs with diffuse expiratory wheeze • Remainder of exam normal ACTIONS? Initial Management • • • • ABCs IV, O2, monitor, full VS CXR? Medications – – – – Steroids (IV vs. PO) Inhaled beta agonist and ipratropium Magnesium if severe exacerbation Antibiotics if infection Case 1: Course • CXR clear • Patient receives steroids and 3 nebs • On reexamination, patient still in moderate distress, states “I am (gasp) getting a bit (gasp) tired, Doc (gasp)!” • PMH: 3 intubations for asthma ACTIONS? Acute Asthma/COPD Exacerbation • Indications for Admission – Incomplete response after initial ED therapy – Failed road test (hypoxia with ambulation) • Indications for Intubation – Respiratory failure – Altered mental status – Patient fatigue after aggressive therapy – Clinical decision more than a laboratory decision Case 2 • • • • • • • 58yo F presents c/o sudden onset SOB +lightheaded, denies CP, denies cough or fever PMH: DM, depression/anxiety Meds: Metformin, tylenol, zoloft, premarin All: ASA SH: +tob, -ETOH FH: DM ACTIONS? Initial Management • • • • • ABCs IV, O2, monitor, full VS EKG pCXR Labs: CBC, M7, Coags, Cardiac enzymes Case 2 • VS 37.6 112 128/76 28 94%RA • Gen: Alert, obese female, slightly uncomfortable • Lungs: CTAB • Heart: Tachy, regular, no murmur • Legs: Trace edema bilaterally, L>R • Remainder of exam normal Case 2 Case 2 ACTIONS? What next? There’s the answer Pulmonary Embolism • 650,000 cases/year in the U.S. • Mortality – 2-12% if diagnosed and treated – 30% if undiagnosed • LE DVT is source in 80-90% of cases • Risk factors – Hormone use, malignancy, immobilization, recent surgery, smoking, peripartum/pregnancy PE Diagnosis • History: – – – – Pleuritic chest pain (49%) Dyspnea (82%) Tachypnea Tachycardia (44%) • Lab: – A negative D-Dimer in a low risk patient may r/o PE – D-dimer not helpful if pre-test probability moderate to high (or if risk is very low per PERC rules)* • Radiology: – CXR often normal – CTA Chest test of choice for diagnosis McGee, S. Evidence Based Physical Diagnosis. 2001 WB Saunders Company. Philadelphia, PA. PE Therapy • Heparin (UF or LMWH), transition to warfarin • Standard of care is hospitalization (for now…) • Thrombolytics, acute surgical or interventional radiologic intervention if in extremis (shock & impending death). Case 3 • 65yo M presents c/o progressive SOB • +dyspnea on exertion, feeling fatigued, abdominal distention • PMH: HTN, CAD s/p stents x 2 • Meds: ASA, Atenolol • All: latex • SH: +tob, +ETOH (social), occ cocaine • FH: CVA ACTIONS? Initial Management • • • • • ABCs IV, O2, monitor, full VS EKG pCXR Labs: CBC, M7, Coags, Cardiac enzymes, BNP Case 3 • VS 37.0 118 166/98 28 92%RA • Gen: Alert, obese male, sitting forward, uncomfortable • Lungs: symmetric crackles B, ½ way up • Heart: Tachy, regular, no murmur, +S4 • Legs: 2+ edema bilaterally • Abd: Obese, mild distention, nontender Case 3 CHF: Diagnostics • Labs – CBC, C7, coags, troponin, BNP • B-type natriuretic peptide – <100 ng/dL Good NPV – Most helpful relative to patient’s baseline – Can be elevated in: PNA, PE, pulm HTN • CXR* • EKG* CHF: Treatment • Reduce Preload – Venodilators (NTG): increase venous capacity – Diuretics: eliminate excess plasma volume • Reduce Afterload – Control BP (NTG): lowers LV work – Positive Pressure ventilation if in extremis • Improve Contractility if in shock – Dobutamine Case 4 • 77yo M presents c/o progressive SOB • +dyspnea on exertion, feeling fatigued. Denies CP • PMH: Denies any. No doctor for 20 years. • Meds: ASA “my daughter makes me” • All: NKDA • SH: -tob, +ETOH (social) • FH: parents lived to their 90s ACTIONS? Initial Management • • • • • ABCs IV, O2, monitor, full VS EKG CXR Labs: CBC, M7, Coags, Cardiac enzymes, BNP Case 4 • • • • • • VS 36.8 118 106/68 96%RA Gen: Alert, thin elderly gentleman, NAD Lungs: CTAB Heart: Tachy, regular, II/VI sys murmur Legs: No edema Abd: Soft, flat, mild epigastric TTP, no r/g Case 4 Case 4 Case 4 • What is your differential diagnosis now? Case 4 • Labs – Troponin, C7, BNP all normal – Charge nurse comes to inform you of a critical value • HCT=18 • Return to your patient – Detailed ROS reveals dark tarry stools x 3 days – Rectal exam reveals melena – Aha! A non-lung cause of dyspnea – You treat your patient for his GI bleeding anemia Dyspnea • Approach all patients with dyspnea as having a serious cause until proven otherwise • H&P, diagnostic testing and treatment should proceed in parallel given range of possible conditions











































![Creating a Clinical Case Study a 10 step model[1]](http://s1.studyres.com/store/data/006729594_1-443bbafc4f1c908ac5f13b3f4ddd91b9-150x150.png)