Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Birth control wikipedia , lookup
Epidemiology of metabolic syndrome wikipedia , lookup
HIV and pregnancy wikipedia , lookup
Women's medicine in antiquity wikipedia , lookup
Maternal health wikipedia , lookup
Prenatal development wikipedia , lookup
Pre-eclampsia wikipedia , lookup
Prenatal nutrition wikipedia , lookup
Prenatal testing wikipedia , lookup
Fetal origins hypothesis wikipedia , lookup
Maternal physiological changes in pregnancy wikipedia , lookup
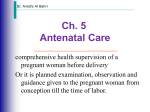
Medical Problems in Pregnancy Dr Suzy Matts FRCOG Consultant Obstetrics and Gynaecology George Eliot Hospital Introduction • Most women in pregnancy are healthy • However, those with medical disorders require expert care • Care may be by the obstetrician, +/- GP and/or medical specialist • May be through normal or specialised ANC • Most complex disorders may need multidisciplinary antenatal care in a tertiary centre Medical Disorders • What disorders can you think of that can affect pregnancy? Medical Disorders • • • • • • • • • • • • • Asthma Cystic fibrosis Hypertension/PIH/PET Arrthymias Valvular disease Cardiomyopathy Cyanotic heart disease VSD/ASD Pulmonary hypertension Epilepsy Multiple sclerosis Intracranial hypertension Benign cranial tumours eg pit adenomas • Obstetric Cholestasis • • • • • • • • • • • • • • Acute Fatty Liver of Pregnancy IBS Crohns/Ulceative colitis Thrombophilias VTE Antiphospholipid syndrome SLE Rheumatoid arthritis Sickle cell disease/thalassaemias Anaemia Diabetes Hypo/hyperthyroidism Adrenal disease Cancer Background • Medical disorders can impact on pregnancy in two ways – Disorders caused by the pregnancy eg • PET/PIH • VTE – Disorders pre-existing by exacerbated by the effects of the pregnancy eg • • • • Heart disease Asthma Immune disorders Epilepsy These conditions make major contributions to maternal deaths Condition 2003-5 2000-2 1997-9 Thromboembolism 41 30 35 Pre-eclampsia and eclampsia 18 14 16 Cardiac Disease 48 44 35 Epilepsy 11 13 9 Asthma 4 5 5 Diabetes Mellitus 1 3 4 Total-named diseases 123 (42%) 109 (42%) 104 (43%) TOTAL Direct + Indirect 295 261 242 Exercise-15 minutes • Prepregnancy actions/changes/ issues • Antenatal issues – Effects on mum – Effects on baby • Screening • Medication issues • Contraindications • Delivery issues • Postnatal issues • Neonatal issues GROUPS: • ASTHMA • EPILEPSY • DIABETES • ESSENTIAL HYPERTENSION • THROMBOPHILIA eg PROTEIN C DEFICIENCY and APLS DIABETES • Important issue in pregnancy – Major impacts on maternal and fetal health • Requires multidisciplinary care in combined clinic • Pre-existing Type 1 • Pre-existing Type 2 (increasing) • Gestational Diabetes (increasing) Diabetes Mellitus and Pregnancy-1 • Diabetes mellitus affects all systems in the body-actual or effective insulin deficiency • 3-4 per 1000 pregnancies • Before insulin in 1921, 40% women died during pregnancy (usually DKA) • Remainder died within 2 years of delivery • Fetal loss rate >50% Diabetes Mellitus and Pregnancy-2 • • • • • • • Introduction of insulin improved outcome Maternal mortality fell to 2-3% Now deaths very rare Fetal loss rates remained high Initially concentrated on reducing stillbirth but PNMR high 1970s-effect on fetus of abnormal glucose levels Optimisation of maternal control and fetal surveillance should lead to PNMR close to non-diabetic – Recent studies show PNMR still double non-diabetic – Fetal anomaly rates 4x those of non-diabetic • Effects of diabetes on pregnancy – Miscarriage – Fetal malformations • Cardiac • Neural tube • Caudal regressions syndrome (200x↑) – – – – IUGR Macrosomia Unexplained IUD PET • Effects of pregnancy on diabetes – Poorer control – Deterioration of renal function – Deterioration of opthalmic disease – Gestational DM Effects of Diabetes - fetus Maternal diabetes hyperglycaemia Fetal hyperinsulinaemia Increased fetal growth Fetal macrosomia Polyuria Polyhydramnios Increased oxygen demands Polycythaemia Risk of cerebral palsy Risk of preterm labour / malpresentation/ cord prolapse Risk of birth injury/ shoulder dystocia Neonatal hypoglycaemia Risk of unexplained term stillbirth Fetal effects • Macrosomia – Increased risks of birth injury/ shoulder dystocia*** – Major cause of obstetric litigation – LSCS recommended in DM where macrosomia and EFW >4000g • Polyhdramnios – Fetal malpresentations and possible increased risk preterm labour • Hyperinsulinaemia – Severe hypoglycaemia (risk of CP) • Polycythaemia – Thrombotic effects – Jaundice • Hypocalcaemia • HOCM Perinatal mortality by plasma glucose levels Pregnancy is diabetogenic • Fetus has little capacity for gluconeogenesis – enzymes are deactivated by low oxygen tensions • Glucose obtained from maternal blood – therefore dependent on maternal nutritional status • Maternal endocrine controls designed to keep blood glucose levels within tight limits – Insulin secretion prevents hyperglycaemia by increasing glucose utilisation for glycogen and fat synthesis and storage – Gut absorption and gluconeogenesis prevent hypoglycaemia Pregnancy is diabetogenic • Progesterone increases maternal appetite and stimulates deposition of glucose in fat stores – Also increases renal gluconeogenesis – Increased protein catabolism • Human placental lactogen (hPL, hPS) acts like growth hormone (GH) – – – – Placental variant of GH Polypeptide hormone Produced from end of 1st trimester onwards Mobilises fatty acids for maternal metabolism Pregnancy is diabetogenic • Relative insulin insensitivity in later pregnancy – Effects of hPL- exaggerated rate and amount of insulin release due to relative insulin insensitivity (requirements may increase by ~30%) – Reduced insulin sensitivity also due to effects of increased levels of cortisol, oestrogen and progesterone – Prolonged hyperglycaemia after eating – Reduced uptake of glucose by maternal tissues more by placental uptake – Facilitated diffusion only saturated at maternal levels of 20 mmol/l Gestational diabetes • Development of severe glucose intolerance in pregnancymay require insulin treatment • ADA recommends all women should have 50g OGTT 24-28 weeks • UK-women with specific risk factors screened – 75g OGTT • Limit to <32 weeks due to slower gastric emptying and unpalatability in late pregnancy • Alternatives: HbA1C, blood glucose series Risk factors for GDM • Family history – One first degree relative – Two second degree relatives • Poor obstetric history – Esp. death of previous macrosomic baby • • • • • • Significant glycosuria Polyhydramnios Macrosomic infant in this pregnancy Polycystic ovary syndrome Wt >100kg or BMI >30 South Asian, Middle Eastern or African origin Oral glucose tolerance test-interpretation (WHO) **=diagnostic of GDM 75g • OGTT Normal Impaired Diabetes Fasting mmol/l <6.0 <6.0 <6.0 or ≥6.0** 2 hours mmol/l ≤7.8 7.8-11.0 >11.0** Diabetes and Pregnancy-Key Points • Pregnancy is diabetogenic, worsening preexisting diabetes and precipitating gestational DM • Increasing obesity increases incidence gestational and Type 2 DM • Poorer control worsens fetal and maternal outcomes • Hyperglycaemia is associated with acute fetal demise: hypoglycaemia is associated with cerebral palsy Diabetes Antenatal Combined Clinic • One stop clinic for women with diabetes in pregnancy-all consultant units • See all professionals on one visit-may or may not be in same room, depending on size of clinic! • • • • • • • Obstetrician Diabetes physician Diabetes nurse Diabetes specialist midwife Sonographers Dietician (psychologist) Management • Pre-pregnancy – Optimise control-aim for BM 4-7 – HbA1C 6.0% or less – High dose folic acid 5mg/day – Stop smoking, weight reduction of BMI raised • Early Pregnancy – Early booking at 6 weeks – Combined clinic every 1-2 weeks – Early dating/viability scan Management • Screening • Combined test at 12 weeks (sl lower sensitivity in DM) – Detailed USS including extended cardiac views • Diabetic control – – – – – May need diet, oral HG or insulin Aim for BM 4-7 Keep HbA1C <6.0% Retinal screening every trimester Dietetic support Management • Pregnancy Care – Regular antenatal care – Serial growth scans 28. 32. 36 weeks – Monitoring for PET – Fetal wellbeing monitoring from 34 weeks – Elective delivery IOL or LSCS • 38-39 weeks in pre-existing DM • 38 wks in GDM on insulin, may be 41 weeks if GDM on diet with normal BMs and fetal growth Management • Neonatal – Paediatric alert – Neonatal surveillance at delivery-may be with mother – Monitor BMs to ensure no neonatal hypoglycaemia • Postnatal – Pre-Existing: Return to prepregnancy insulin / oral HG agent regime – GDM: stop treatment and monitor BMs for 48 hours to ensure return to normal and no persistence of IGT Thyroid and Pregnancy • hCG has thyrotrophic function – May suppress TSH during first trimester – Thyrotoxicosis may be a feature of hydatidiform pregnancy where levels of hCG are extremely elevated • Thyroid function remains essentially normal in pregnancy – Marked increase in thyroid binding globulin (? Effect of oestrogen?) – Increase in bound thyroxin (T4) t3 (more active)and rT3 (inactive) – Free T4 and T3 are unaltered or slightly reduced • NOTE: increased BMR, tachycardia, elevated body temperature and increased CO are normal in pregnancy but may mimic the effects of hyperthyoidism Thyroid and Pregnancy • Hypothyroid: – Check TFT (TSH) at booking and every trimester – Likely to need increase in thyroxine dose during pregnancy – If anti-thyroid antibodies, inform paeds who will need to check fetal TFT at birth Thyroid and Pregnancy • Hyperthyroid – – – – May worsen due to HCG Risks-hyperemesis, miscarriage Can use carbimazole but not PTU (or radio-I2) to treat Regular TFTs and multidisciplinary care • If well controlled, no other impact on pregnancy care (fetal growth, delivery etc) • Inform Paeds to check fetal thyroid function, especially if pt has thyroid Abs Pre-Eclampsia Definition • Hypertension and proteinuria with onset ≥20 weeks – Oedema from classical definition dropped as not discriminating clinically • Diastolic ≥90mmHg on 2 occasions 4-6 hours apart OR ≥110mmHg on one occasion • Proteinuria >300mg/24 hours • Symptoms • Differentiation from PIH/renal disease PET/Eclampsia George Eliot Hospital, Nuneaton 32 Hypertensive disorders Raised BP in pregnancy > or = 140/90 Pregnancy induced hypertension (Raised BP after 20 weeks) No proteinuria PIH Mild and moderate PET PET/Eclampsia Chronic hypertension (Raised BP before 20 weeks gestation) Proteinuria and Raised BP Pre -eclampsia Severe PET Eclampsia George Eliot Hospital, Nuneaton HELLP 33 Incidence • 2-3% pregnancies • 5-7% primips • 1.8% PET will develop eclampsia (from Collaborative Eclampsia Trial = 49/ 100000) • Rates eclampsia 26.8/100 000 maternities (UKOSS reporting system 2003-5) • Worldwide 1.5-8 million develop PET with 150 000 deaths • Deaths 2003-5: 0.85/100000 maternities • 18 deaths • 10 cerebral haemorrhage, 2 cerebral infartion • 6 were eclamptic, 8 had HELLP syndrome PET/Eclampsia George Eliot Hospital, Nuneaton 34 Importance • Maternal morbidity – Blindness – Neurological – renal • Fetal death – Abruption, hypoxia, IUGR • Fetal morbidity – Prematurity (PET is cause of >40% iatrogenic preterm dels) with risks respiratory and neurodevelopmental complications (inc.learning difficulty/IQ in up to 60%) PET/Eclampsia George Eliot Hospital, Nuneaton 35 Risk Factors:-Pre-Eclampsia • Primiparous • First pregnancy with new partner • Family history (1 in 3 risk if mother had PET) • Twins/multiples • Pregestational Diabetes PET/Eclampsia • • • • Essential hypertension Renal disease SLE Antiphospholipid syndrome • Thrombophilias • Age >40 • Obesity George Eliot Hospital, Nuneaton 36 Pathophysiology • “The disease of theories” • Pregnancy specific syndrome • Placenta has a central role to play – Reduced placental perfusion – Inadequate vascular remodelling at ~16 wks • Genetic component in some women tho’ not in others – No candidate genes or consistent results PET/Eclampsia George Eliot Hospital, Nuneaton 37 Pathophysiology of PET PET/Eclampsia George Eliot Hospital, Nuneaton 38 2 stage process • Inadequate implantation • Poor remodelling STAGE 1:Reduced • Cytokines produced + growth factors • placental apoptosis/necrosis • Shedding of microparticles into circulation placental perfusion • Markers seen preceding PET • Inflammation and endotheial activation PET/Eclampsia STAGE 2: Maternal syndrome (multisystem disorder) George Eliot Hospital, Nuneaton 39 Prevention of PET: Aspirin • Several small trials suggested reduction in rates PET with low dose aspirin therapy • Large multicentre trial (CLASP) in 9364 women did not demonstrate benefit for wholescale prophylaxis for low risk women – Trend towards reduction in likelihood to preterm delivery – No significant increased risk of haemorrhages – No statistically significant effect on stillbirths/ neonatal deaths – Non significant (12%) reduction in incidence PET Lancet 1994; 343: 619-629 PET/Eclampsia George Eliot Hospital, Nuneaton 40 CLASP • Trial suggested only benefits in women at high risk of severe early onset IUGR ? How to identify • Benefits thus suggested in women with previous severe early onset PET and IUGR • ?relationships to APLS (not investigated in original trial) PET/Eclampsia George Eliot Hospital, Nuneaton 41 Prevention: Aspirin • More recent study showed aspirin treatment produced at RR of 0.9 (95% CI 0.84-0.97) for PET • Moderate but consistent reductions in PET, preterm delivery and serious outcomes Lancet 2007 PET/Eclampsia George Eliot Hospital, Nuneaton 42 Prevention: Calcium • Calcium levels lower in women with PET compared to ‘normal’ pregnancy • Australian Randomised Study in 456 singleton nullips from <24/40 showed reduction in risk PET with 1.8g calcium/day compared to placebo • RR 0.44 95% CI 0.21-0.90 Aus NZ J Obstet Gynaecol 1999; 39: 12-18. PET/Eclampsia George Eliot Hospital, Nuneaton 43 Prevention: Calcium • Calcium for Eclampsia Prevention Study (CPEP) Am J Obstet Gynecol 1997; 177: 1003-10 • 4589 US women in multicentre trial • All nullips • Analysis of risk factors for development of subsequent PET did not show any benefit from Ca++ supplementation PET/Eclampsia George Eliot Hospital, Nuneaton 44 Prevention: Calcium • • • • Cochrane Review Cochrane Database 2000 (3), OUS. 9 studies, all good quality Ca++ dose > 1g/day Modest reduction in risk PET for all women (RR 0.72, 95% CI 0.6-0.86) • Greatest effect where highest risk- RR 0.22, 0.11-0.43 and low dietary intake (0.32, 0.21-0.49) • No effect on preterm delivery • Smaller effects seen for hypertension – Ca++ appears of benefit for women at high risk of developing PET – Also women from communities with low dietary intake – Optimum dosage requires further evaluation PET/Eclampsia George Eliot Hospital, Nuneaton 45 Prevention: Antioxidants • Vitamin C 1000mg and Vit E 400 IU/day • 58% reduction in PET in treated group Chappell et al, Lancet 1999 354: 810-5 • A number of trials ongoing globally • All using above dosages • 3 reported so far-NO difference in rates treatment vs placebo. PET/Eclampsia George Eliot Hospital, Nuneaton 46 Diagnosis: Pre-Eclampsia • Classic triad – Hypertension 140/90 – Proteinuria >300mg in 24 hours (RCOG) – Oedema (least reliable) • BP rise should be from booking >30/15 • Proteinuria and raised BP x 2 occasions 6 hrs apart (or once if DBP ≥110 and heavy proteinuria >2+ (=1g/24h)) PET/Eclampsia George Eliot Hospital, Nuneaton 47 Mild PET • • • • Classically asymptomatic BP 140/90 (ish) Maybe trace-+ proteinuria Often incidental finding at CMW clinic attendance PET/Eclampsia George Eliot Hospital, Nuneaton 48 What questions should you ask? What questions should you ask? • Headache (classically severe) – Effects hypertension • Visual disturbances (‘flashing lights’) – Sign of cerebral vasospasm/impending eclampsia • Epigastric pain – Hepatic congestion/liver capsule stretching • Is baby moving normally? – Fetal wellbeing What investigations should you arrange? • Maternal • Fetal PET-Investigations • • • • • • FBCU+E Urate LFTs Clotting MSU PET/Eclampsia platelet count signs renal dysfunction (late) hyperuricaemia ( early ) elevated transaminases XXXX (not routinely if plts>100) to exclude UTI as cause of protein George Eliot Hospital, Nuneaton 52 PET • Fetal assessment – Clinical – USS for growth – CTGs • ?cervical assessment (depending on gestation) PET/Eclampsia George Eliot Hospital, Nuneaton 53 Monitoring • Monitor BP – CMW – Day assessment or Triage Unit • Monitor bloods – Weekly or twice weekly (depends on sitn) • Monitor fetus – CTG – Serial USS PET/Eclampsia George Eliot Hospital, Nuneaton 54 Definitive treatment • Deliver when – BP/protein or clinical condition deteriorates so become moderate or severe PET – Reaches 41 weeks and no change in condition – Fetal condition mandates delivery even if maternal condition stable PET/Eclampsia George Eliot Hospital, Nuneaton 55 Severe pre-eclampsia • Hepatic • SYSTOLIC 160-180 • DIASTOLIC >110 • CNS – Abnormal LFTs, dysfunction – RUQ pain – Epigastric pain – Headache – Visual disturbances – Disorientation/ irritability – Hyperreflexia – clonus PET/Eclampsia • Renal – Elevated creatnine, urea, urate – Oliguria – Heavy proteinuria >5g in 24 hrs • Haemtological – Thrombocytopaenia – haemolysis George Eliot Hospital, Nuneaton 56 Multisystem disease • Eyes – – – – – • Liver – Subcapsular haemorrhages – Liver rupture Arteriolar spasm Retinal haemorrhages Blindness Scotoma Papilloedema • Kidneys – Acute renal failure • Fetoplacental Unit • CNS – – – – Seizures Encephalopathy Cerebral haemorrhages CVA • Respiratory – Pulmonary oedema – ARDS PET/Eclampsia – – – – IUGR Abruption Fetal compromise Fetal death • Haemotological – DIC – haemolysis George Eliot Hospital, Nuneaton 57 Symptoms • • • • Headache (BP) Flashing lights (lightning) (cerebral oedema) Epigastric pain (stretching of liver capsule) Oedema (albumin/BP) • Asymptomatic PET/Eclampsia George Eliot Hospital, Nuneaton 58 Management of severe pre-eclampsia • Immediate admission to hospital • High dependency care/LW-QUIET – Invasive monitoring – NICU for baby if early gestation • Senior multidisciplinary involvement early-obs and anaesthetics PET/Eclampsia George Eliot Hospital, Nuneaton 59 Aims of treatment • Aims – Prevent seizures – Control hypertension (to prevent cerebral haemorrhage) – Deliver safely (stabilise, +/- IUT, +/- steroids) PET/Eclampsia George Eliot Hospital, Nuneaton 60 Maternal Assessment • • • • • BP-check every 15 minutes Urine output-hourly Urinary protein dipstix Strict fluid balance chart Bloods – U+E, urea, creatnine, urate – FBC esp. platelets (G+S) – LFTs • Deep tendon reflexes and presence of clonus • CTG PET/Eclampsia George Eliot Hospital, Nuneaton 61 Control blood pressure • Antihypertensives – aim for diastolic 85-95 – IV hydralazine (5mg every 15 minutes to acutely control BP) – IV labetolol (Not good if asthmatic or already signs of pulmonary oedema-first line in many places now) – Oral nifedipine 10mg NOT SUBLINGUAL – Methyldopa TOO SLOW ONSET (24-48 hours) for use in acute situation – Titrate IV antihypertensive vs. BP then infusion PET/Eclampsia George Eliot Hospital, Nuneaton 62 KEY POINTS: Hypertension Systolic blood pressure of 160 mm/Hg or more = anti-hypertensive treatment. (irrespective of diastolic) Consideration starting treatment at lower pressures if the overall clinical picture suggests likely rapid deterioration with anticipation of severe hypertension. PET/Eclampsia George Eliot Hospital, Nuneaton 63 Prevent Fits • Magnesium sulphate – – – – – – – – PET/Eclampsia All severe and moderate PET (MAGPIE) 4g IV over 15 minutes Then infusion 1g/ hour Monitor reflexes (present) urine OP (>30ml/hr) and respiratory rate (>12/minute) Slows neuromuscular conduction and decreases CNS irritability Best anticonvulsant in these circumstances AND IN ECLAMPSIA No effect on BP Tell anaesthetist if GA as potentiates effects of muscle relaxants George Eliot Hospital, Nuneaton 64 Magnesium toxicity • If urine OP OK then likely • Magnesium levels – Therapeutic 2-4 mmol/l not to accumulate (85% – Warmth, flushing, slurred speech renal excretion) 3.8-5mmol/l • If urine output falls, – Loss of patellar reflexes >5 mmol/l reduce dose to 0.5g/hour – Respiratory depression >6 mmol/l • If signs toxicity, stop – Respiratory arrest 6.3-7mmol/l • Antidote = Calcium – Cardiac arrest, asystole >12 gluconate 1g IV over 3 mmol/l minutes PET/Eclampsia George Eliot Hospital, Nuneaton 65 MAGPIE • 10141 women-99% received allocated treatment • 24% of women with MgSO4 reported side-effects compared to 5% of women on placebo • MgSO4 produced 58% reduced risk of eclampsia (0.8% cf. 1.9%)-across all categories of PET • Maternal mortality lower as well RR 0.55, CI 0.26-1.14 • Only improvement in maternofetal morbidity was reduced risk of abruption (0.67, 99% CI 0.45-0.89) • No substantial harmful risks to mother or fetus Lancet 2002; 359: 1877-90. PET/Eclampsia George Eliot Hospital, Nuneaton 66 MAGPIE PET/Eclampsia Lancet 2002; 359: 1877-90. George Eliot Hospital, Nuneaton 67 Deliver Baby • If severe PET, should NOT transfer • Ensure SCBU aware if baby premature • Give antenatal steroids if time but usually, if require IV therapy, delivery is indicated once stabilised • If cervix favourable and patient >36 weeks, consider short trial IOL • If cervix unfavourable and/or <36 weeks, deliver by LSCS • Anaesthesia epidural vs. general PET/Eclampsia George Eliot Hospital, Nuneaton 68 DELIVERY: Key Points 1 Risk of sharp rise of BP on intubation This may be obtunded by large dose alfentanyl or similar Need experienced and senior anaesthetist to give GA in these circumstances PET/Eclampsia George Eliot Hospital, Nuneaton 69 DELIVERY: Key Points 2 Syntometrine should not be given for the active management of the third stage if the mother is hypertensive, or if her blood pressure has not been checked. (ergometrine causes vasospasm and a sharp rise in BP which may precipitate hypertensive crisis, fits or cerebral haemorrhage) PET/Eclampsia George Eliot Hospital, Nuneaton 70 Eclampsia • Occurrence of fits – 44% postpartum – 38% antenatal) – ALWAYS GRAND MAL • • • • • • Due usually to cerebral vasospasm Do not try to shorten initial convulsion (self-limiting) Prevent maternal injury Maintain oxygenation Prevent aspiration ABC… PET/Eclampsia George Eliot Hospital, Nuneaton 71 Eclampsia • Beware known epileptics – If BP normal, no protein, typical for their type of fit-may be epilepsy BUT any fit must be considered as eclampsia until proven otherwise especially of BP slightly up etc • Any FOCAL fit is not eclampsia – Consider SOL eg cerebral bleed/infarction due to severe PET – Arrange head CT urgently PET/Eclampsia George Eliot Hospital, Nuneaton 72 Collaborative Eclampsia Trial • Multicentre international trial Lancet 1995; 345: 1455-63 • 1687 women • Comparisons: – MgSO4 vs. diazepam • 52% lower risk recurrent convulsions with MgSO4 – MgSO4 vs. phenytoin • 67% lower risk recurrent convulsions with MgSO4 • Maternal mortality nonsignificantly lower in MgSO4 • Less risk of pneumonia, ventilation, ITU with Magnesium • Babies less likely to be intubated and go to SCBU PET/Eclampsia George Eliot Hospital, Nuneaton 73 Eclampsia • Treatment is IV magnesium sulphate-4g loading then 1g/hr • If recurrent fits or fit already on MgSO4, then further 2g IV bolus/increase infusion to 1.5g/hr • If fits persist, check magnesium levels, contact anaesthetists, consider CT, consider intubation and ventilation • If antenatal, stabilise and Deliver PET/Eclampsia George Eliot Hospital, Nuneaton 74 Postnatal care • Watch closely on HDU/LW until diuresis and condition improving • Anticipate possible worsening or seizures in first 1824 hours • Continue MgSO4 for 24 hours and then review • Do not need to taper off MgSO4 • Do not feed within 12 hours as significant risk ileussips H2O only until next morning then review for bowel sounds PET/Eclampsia George Eliot Hospital, Nuneaton 75 Postnatal Management-Hypertension • Hypertension may persist for some weeks • Switch to oral treatment when feasible – Atenolol – Nifedipine • Polypharmacy may be required to control BPconsult with physicians • Ensure regular BP checks arranged on discharge with review and follow-up by GP PET/Eclampsia George Eliot Hospital, Nuneaton 76 Postnatal Management-Fits • Eclampsia Survey showed 44% of fits occur postpartum • High index of suspicion • Beware worsening of condition • MgSO4 prophylaxis in all severe PET and all eclamptics • All women with severe PET should have MgSO4 for 24 hours following delivery or following last fit-whichever is longer PET/Eclampsia George Eliot Hospital, Nuneaton 77 Postnatal Management-Fluids • Fluid overload real danger after delivery – Relaxed vigilance – LSCS – PPH – Physiological oliguria • STRICT FLUID BALANCE PET/Eclampsia George Eliot Hospital, Nuneaton 78 Postnatal Management-Fluids • SHIP audit (1997) showed that many women have oliguria but intervention not required unless UO <100ml in 4 hours • Fluid overload carries risks of pulmonary oedema– Reduced plasma oncotic pressure – Hypertension thus increased gradient across microvasculature – Filtration of fluid into tissues – Pulmonary oedema PET/Eclampsia George Eliot Hospital, Nuneaton 79 Postnatal Management-Fluids • Women with PET are very vulnerable to Pulmonary oedema • Carries risk of ARDS if severe or not recognised rapidly • ARDS may be fatal • Fluid restriction is far SAFER – Renal function more likely to recover than pulmonary and less likely to kill pt PET/Eclampsia George Eliot Hospital, Nuneaton 80 Causes of death SHIP PET/Eclampsia George Eliot Hospital, Nuneaton 81 Fluid Balance • Take Home messages – Fluid restrict as pt already fluid overloaded – Scrupulous input and output – Do not fluid challenge – Do not give frusemide – Consider CVP line if urine output poor – Seek senior advice early – Multidisciplinary Mx-obs/anaesth/renal teams PET/Eclampsia George Eliot Hospital, Nuneaton 82 GI management • Don’t forget stress response to illness• H2 antagonists (eg Ranitidine) • Delay feeding until bowel sounds present – May develop ileus if v unwell PET/Eclampsia George Eliot Hospital, Nuneaton 83 Disease Progression • Often improve quickly • Some may deteriorate further immediately after delivery –may continue to worsen for 24 + hours – – – – Worsening BP Worsening bloods Oliguria/anuria Increased risk fits • Consult seniors and manage with multidisciplinary team PET/Eclampsia George Eliot Hospital, Nuneaton 84 HELLP syndrome • • • • • Haemolysis Elevated Liver Enzymes Low Platelets • 1-12% PET (usually severe end of spectrum) • Commoner in multips • Variable presentation – RUQ pain, epigastric pain, nausea + vomiting – 85% hypertensive at presentation • Present: 2/3 antepartum, 1/3 postpartum – mid 2nd trimester to several days postnatal PET/Eclampsia George Eliot Hospital, Nuneaton 85 Differential diagnosis in HELLP • Any liver problems – Biliary colic – Cholecystitis – Hepatitis • Gatroenteritis or reflux • Pancreatitis • ITP/ TTP PET/Eclampsia • Ureteric colic • Renal calculus • Rare-if severe pain: • Aortic dissection • MI George Eliot Hospital, Nuneaton 86 Management of HELLP • • • • • • • Treat as severe PET Stabilise Fluids Antihypertensives MgSO4 Anti-thrombotic agents Coagulation factors (if required) PET/Eclampsia • Assess baby – USS – CTG • (remember 20% risk of abruption) • PLAN DELIVERY ASAP • TRANSFER TO TERTIARY CENTRE IF REQUIRED • IOL or LSCS George Eliot Hospital, Nuneaton 87 Summary-PET, eclampsia, HELLP • Serious disease with potential for maternal and fetal mortality • Prevention not widespread ? Aspirin for some ? Calcium for all • Treatment depends on prevention of complications and timing delivery • Senior involvement in severe cases PET/Eclampsia George Eliot Hospital, Nuneaton 88 Essential Hypertension • Pre-existing raised blood pressure • May be on treatment or just under observation • May be known prior to pregnancy or detected at booking as raised BP Cardiovascular changes of Pregnancy • Massive changes in cardiac output and haemodynamics • Already occurred largely by 12 weeks Haemodynamic changes of pregnancy • Progressive rise in HR • Increase in SV by 10 weeks • rise in CO (CO=HR x SV) • BP falls from end first trimester (fall in TPR) • BP rises in late pregnancy Haemodynamic changes of pregnancy • Cardiac output – Increases by 40% (5l/min prepregnancy to 7l/min by 20 weeks) – Mainly due to increased SV (10-20 ml) • Maternal HR increases to 80-90bpm (15% ↑) – ‘palpitations’ • TPR falls due to vasodilation – Feeling hot • BP falls during pregnancy but rises towards term – fainting Supine hypotension • • • • • • • Affects 10-15% of women Aortocaval compression by gravid uterus (usually from 20-24 weeks) Reduces venous return reduces CO At term IVC may be totally occluded by uterus when supine CO may reduce by 25-33% Use of left lateral position or wedge/ tilt – Pregnant women feel uncomfortable and may refuse to lie flat – BP inaccurate in supine pregnant woman Blood pressure changes • Early pregnancy – Reduced DBP but little change SBP wider pulse pressure – Traditionally use 4th Korotkoff sound for BP but poorly reproducible-5th sound still more accurate in pregnancy • Changes reverse in 2nd half of pregnancy Risks to Mum • Worsening of BP • Superimposed preeclampsia • Medical overintervention Risks to Baby • Teratogenesis from certain drugs (eg ACEI) • IUGR • Pre-eclampsia • Hypoglycaemia if on labetolol and breastfeeding Pre-pregnancy • If planned, review medications – Take off tertaogenic meds eg ACEI or similar – Take off diuetics • Optimise diet • Stop smoking • Start folic acid Early pregnancy • • • • • • Review meds at booking Take off any teratogenic meds Start folic acid Early booking at hospital for risk review Dating scan +/- NT (combined) scan Plan for pregnancy – Including issues re: obesity, screening for GDM Pregnancy • Regular BP checks • May need to come off meds if BP ↓↓ • May need to start or restart meds later in pregnancy as BP rises • ? Growth scans • Joint care between MW and hospital Later Pregnancy • If BP well controlled and fetal growth normal, aim to labour spontaneously or induce as postdates • If BP raised, try control first with medications • If superimposed PET or fetal growth issues, consider delivering early • NO ERGOMETRINE at delivery-syntocinon only Post delivery • Watch BP for at least 24-48 hours • May need oral antihypertensives • Communicate closely with GP to ensure that BP monitoring is taken over and ongoing care is handed over to GP Cardiac Disease • Pre-existing/congenital – Valvular disease – coarctation • Acquired – IHD – Aortic aneurysm – cardiomyopathy Importance • Leading Indirect Cause • Rate 2.27 / 100 000 of Maternal Death AND maternities -rising: the most common • 2002-2 2.20 single cause of maternal • 1997-9 1.65 death! • 48 women 2003-5 • 46% had substandard care Prepregnancy • Review by cardiologist – Including advice whether should risk pregnancy • • • • Optimise condition Advice regarding pregnancy Stop smoking Start folic acid New York Heart Association Heart Functional Classification. Class I Patients have no limitation of physical activity. Ordinary physical activity does not cause undue fatigue, palpitations, dyspnoea or anginal pain. Class II Patients have slight limitation of physical activity. Ordinary physical activity results in fatigue, palpitations, dyspnoea or anginal pain. Class III Patients have marked limitation of physical activity. Less than ordinary activity causes fatigue, palpitations, dyspnoea or anginal pain. Class IV Patients have inability to carry out any physical activity without discomfort. Symptoms of cardiac insufficiency or of anginal syndrome may be present, even at rest. If any physical activity is undertaken, discomfort is increased. Risk of Mortality <1% • • • • • • • ASD VSD PDA Pulmonary/tricuspid disease Corrected Tetraology of Fallot Mitral stenosis, Functional Classes 1 and 2 Prosthetic valve (animal) Risk of Mortality 5-15% • • • • • • • • Mitral stenosis with AF Artificial Valve Mitral stenosis (Class 3 and 4) Aortic stenosis Coarctation of the aorta Uncorrected tetralogy of Fallot Previous MI Marfan’s Syndrome with normal aorta Risk of Mortality 25-50% • Pulmonary hypertension (Primary and Eisenmengers)** • Coarctation of the Aorta, complicated • Marfan’s Syndrome with Aortic Involvement • Previous cardiomyopathy, residual ventricular dysfunction** • **would usually counsel against ever conceiving At Booking. • All women should have their health assessed and history of previous murmur, cardiac disease or risk factors for coronary artery disease (obesity, smoking, diabetes, hyperlipidaemia, preexisting hypertension, age >35, positive family history for ischaemic heart disease) – should be counselled to inform attendants should they develop any symptoms of chest/arm/jaw pain, shortness of breath, palpitations. • All immigrant women should undergo cardiovascular examination at booking by an appropriately trained professional (GP, obstetrician)6. • Women with known cardiac history should have early referral and details of their condition should be sought urgently from GP or cardiologist. – They should be urgently assessed by consultant obstetrician and/or cardiologist. Referral to tertiary centre (specific antenatal cardiology clinic at BWH) may be necessary. In Pregnancy • Should patient stay in your unit? – High risk cases should be transferred to unit with specialist antenatal cardiology service (eg BWH) • Is there a risk of cardiac defect in fetus? – Congenital cardiac disease eg Fallot, coarctation, ASD/VSD, valvular disease ALL carry increased risk of cardiac disease in fetus (2-5%) thus qualify for detailed fetal echocardiogram in BWH Fetal Medicine Centre In Pregnancy • Should you continue with the pregnancy? – Pulmonary hypertension carries 50% risk of death. Patients should be aware of the very real risks of dying and be given the choice • Is there anything special I need to do for pregnancy? – In terms of monitoring, medication, scans etc – Eg antibiotics to cover labour, no ergometrine at delivery In Pregnancy • Mode of delivery? – Caesarean or vaginal? – Allow pushing or shorten second stage? – Epidural to reduce rise in heart rate • Anaesthetic issues? • Care and monitoring following delivery? • Advice re: contraception following delivery Common Problems in Pregnancy • Palpitations • Common. • Many are merely ectopic beats but a few may be genuine SVTs. – Check Hb, Thyroid function and perform basic cardiovascular examination (pulse, BP, JVP, auscultation chest and heart, look for oedema). Pulse >100 should prompt immediate ECG and medical review. – Arrange ECG as outpatient if pulse less than 100 and regular. – Organise review with Physician – Further investigations may include 24 hour ECG tape but many women will be reassured and discharged back to normal care. Common Problems in Pregnancy • Supraventricular Tachycardias (SVT) • Not uncommon as known pre-existing condition • Investigate as palpitation but more urgently(if occur de novo)! • Drugs used to treat known cases (eg verapamil, flecainide) do not affect fetus and are not associated with teratogenic effects and patient should be reassured of this. • Ensure regular review with their cardiologist but treat pregnancy otherwise as normal. Common Problems in Pregnancy Heart Murmurs. Commonly heard in pregnancy. Many are flow murmurs but some may represent valvular disease or septal defects. • • • • • Investigations: Arrange Physician or Cardiologist review Check function status-any symptoms? Arrange ECHOCARDIOGRAM If valvular lesion seen (NOT mitral valve prolapse) ensure fetus has cardiac scan arrange at detailed USS . • • • Management. 1. If flow murmur only reassure patient. No further action required. 2. If valvular lesion (stenosis, incompetence or MVP) (see below for more details) give antibiotics to cover labour. – Refer cardiologist for assessment. – Arrange cardiac scan for fetus • 3. If septal defect (VSD, ASD), arrange cardiology review. – Antibiotics to cover labour or invasive procedures – Fetal cardiac scan Suspected Cardiac Disease In Pregnancy • Clinicians should have a low threshold for investigating women (especially those with the risk factors for cardiac disease) who complain of – severe chest pain, – chest pain that radiates to the neck, jaw or back, – chest pain associated with other features such as agitation, vomiting or breathlessness, tachycardia, tachypnoea or orthopnea. • Remember that shortness of breath, wheezing, palpitations and irregular heart beat may all be symptoms of/associated with heart failure. All women with these symptoms should be undergo and proper full cardiovascular and respiratory examination. If in doubt, seek senior advice. Suspected Cardiac Disease In Pregnancy • Management: – 15 minute observations and MEWS chart should be started with continuous electronic fetal monitoring if the pregnancy is 25 weeks or above. – The patient should be managed as a potential high dependency case. – Observations should include respiratory rate and oxygen saturations as well as temperature, pulse and blood pressure. • Appropriate investigations include chest X-ray (CXR), ECG, cardiac enzymes (Troponin T), Echocardiogram and CT pulmonary angiography. – NB: if the clinician is not confident or competent to interpret the ECG, he should show it to someone who is. Suspected Cardiac Disease In Pregnancy • The Medical Registrar, though familiar with management in non-pregnant patients, may not be so familiar with disease in pregnancy • He might benefit from input from obstetric team in jointly managing the case. • Teams are told to contact obs consultant and potentially the medical consultant if still unhappy with the advice given. If a patient is very short of breath and obviously pregnant, what is the first diagnosis you will think of? Venous Thromboembolism • Leading direct cause of maternal death • Second most common cause overall – 1997-9 – 2000-2 – 2003-5 35 deaths 30 41 – Rate 1.43/100 000 maternities – in pregnancy risk VTE 60/1000 • cf 1/1000 nonpregnant, no hormone, • 15/1000 3rd gen COCP, • 30/1000 2nd gen COCP Risk Factors for VTE • Known thrombophilias e.g. Protein S or Protein C deficiency, Factor V Leiden, Anti-Thrombin III deficiency • Antiphospholipid syndrome • Previous DVT or PE • Strong family history VTE (DVT/PE) • Obesity (BMI ≥30) • Age >35 • Pre-eclampsia • Parity >3 • Paraplegia • Sickle cell disease • Inflammatory disorders and infection e.g. inflammatory bowel disease and UTI Risk Factors for venous thromboembolism in pregnancy or the puerperium PRE-EXISTING – Previous VTE – Thrombophilia • Congenital • Acquired – – – – – – – – Obesity BMI>30 Para>4 Gross varicose veins Paraplegia Sickle cell disease Inflammatory disorders Some medical disorders Myeloproliferative disorders NEW ONSET OR TRANSIENT – Surgical procedure in pregnancy or puerperium – Hyperemesis – Dehydration – Severe infection eg pyelonephritis – Immobility >4 days bedrest – Pre-eclampsia – Excessive blood loss – Long haul travel – Prolonged labour – Midcavity instrumental delivery – Immobility after delivery Review of underlying physiology • Pregnancy is pro-thrombotic • Compounded by effects of Virchow’s triad – Stasis • Secondary to venous compression by pregnant uterus – Hypercoagulability • Effects of pregnancy – Vascular damage • Varicose veins Coagulation changes in pregnancy • Increased levels factors VII, VIII, X and Fibrinogen • Effects on both intrinsic and extrinsic pathways Reducing the Risk in Pregnancy • Score all women at booking (on basis weight/history etc) • If possible increased risk on basis of personal or family history but does not fulfil criteria for immediate prophylaxis, discuss with consultant. • One option is to investigate if persuasive reasons to do so (eg unexplained poor obstetric history, no family history available as adopted etc) – perform FBC, clotting studies, thrombophilias screen, anti-cardiolipin, lupus anticoagulant screening. – Be aware levels of Proteins S and C alter during pregnancy. • Even if patient does not require prophylaxis usually, reconsider if: – Dehydration e.g. hyperemesis, OHSS, prolonged vomiting+pyrexia – Immobility e.g. bedrest for symphysis dysfunction, illness including dehydration, paraplegia – Any surgery considered even if not gynaecological Which agent, how to start prophylaxis and how much? • Low molecular weight heparin is the default agent – George Eliot Hospital currently uses Enoxaparine • Dose dependent on booking weight – Warfarin is associated with 6% risk warfarin embryopathy so should only be used where heparin is considered unsuitable such as in some women with mechanical heart valves – Oral thrombin and Xa inhibitors (Dabigatran and rivaroxaban) are not licensed for pregnancy and there is no experience of their use. Therefore they should be avoided in pregnant women. Risk Who should have antenatal prophylaxis? History Prophylaxis Very high Previous VTE on long-term warfarin Antithrombin deficiency Antiphospholipid syndrome with previous VTE Recommend antenatal high-dose LMWH and at least 6 weeks postnatal LMWH/warfarin Requires specialist management by experts in haemostasis and pregnancy High Previous recurrent or unprovoked VTE Previous estrogen-provoked (pill or pregnancy) VTE Previous VTE + thrombophilia Previous VTE + family history of VTE Asymptomatic thrombophilia (combined defects, homozygous FVL) Recommend antenatal and 6 weeks postnatal prophylactic LMWH Single previous VTE associated with transient risk factor no longer present without thrombophilia, family history or other risk factors Asymptomatic thrombophilia (except antithrombin deficiency, combined defects, homozygous FVL) Consider antenatal LMWH (but not routinely recommended) Recommend 6 weeks postnatal prophylactic LMWH Recommend 7 days (or 6 weeks if family history or other risk factors) postnatal prophylactic LMWH Intermediate FVL = factor V ; LMWH = low-molecular-weight heparin What symptoms are you looking for in possible VTE? What symptoms are you looking for in possible VTE? • • • • Shortness of breath Pleuritic chest pain Haemoptysis Collapse • Symptoms of DVT– leg pains or discomfort, swelling and tenderness, oedema – More common on left – Usually iliofemoral in pregnancy Investigations-DVT Investigations-DVT • FBC, baseline coagulation screen, U&E, LFT • D dimer (negative predictive value still useful but almost ALL women test positive anyway in late pregnancy) • Thrombophilia screen not indicated at this stage Imaging in DVT • Compression duplex USS test of choice – If negative and low level clinical suspicion-discontinue Rx – If still high level clinical suspicion-continue LMWH and repeat USS in 1 week – Or try alternative modality • If suspect iliac DVT, consider MR venography or conventional venography Doppler ultrasound Investigations - PE Investigations - PE • Blood tests as above • ECG • Chest X-Ray PE • CXR should be performed in all women – Normal >50% women with objectively proven PE – But PE may cause atelectasis, effusion, focal opacities, regional oligaemia or pulmonary oedema • If negative, bilateral compression Duplex dopplers should be performed • Radiation dose to fetus is negligible at all gestations PE: next steps • CTPA if still clinical suspicion in non-massive PE – Lower radiation dose to fetus – Better sensitivity and specificity in non-pregnant women (BTS) – Can detect other pathology e.g. aortic dissection CTPA: radiation issues • Higher radiation dose to maternal breasts – (20 mGy)-dose of >10 mGy increases lifetime risk of Ca breast • Increased risk estimated at 13.6% (background 1/200) – Prob overestimate in non-pregnant woman – BUT breast in pregnancy more sensitive? • Women with +ve/strong FHx? CTPA: radiation issues (2) • 10% dose to fetus of V/Q scan • Risk of childhood cancer 1/1 000 000 after CTPA vs 1/280 000 with V/Q V/Q? • Traditionally investigation of choice • BUT geographically limited (travel to another unit) • Limited availability due to isotope availability (waiting for availability-bed occupancy, unnecessary anticoagulation, separation from family) • Also radiation issues V/Q • • • • Less sensitivity and specificity Equivocal results? High negative predictive value BUT Ventilation scan may be preferable in women with FHx Ca breast Pulmonary angiography • Highest radiation dose to fetus (0.5 mSv) and to maternal breast (5-30 mSv) Massive life-threatening PE • Medical emergency • Full medical team + consultant obstetrician + senior radiologist • Urgent portable ECHO +/- CTPA within 1 hour of admission • May decide therapy before confirmation (thrombolytic Rx/IV heparin/embolectomy etc) Suspected VTE in pregnancy • “Treat then see” • Immediately start therapeutic LMWH • (1mg/kg prepregnancy wt/12hrs) • Then arrange diagnostic tests Treatment • LMWH from suspicion • Treatment dose-1mg/kg bd • Continue until delivered (+6 weeks) or 6 months postnatal, whichever is longer Antiphospholipid Syndrome (APLS) • Presence of antiphospholipid antibodies(aPL)antiCardiolipin (aCL) and lupus anticoagulant (LA) with one or more of the characteristic clinical features = APLS Criterion Description Thrombosis Venous Arterial Small Vessel Pregnancy Morbidity 3 consecutive miscarriages <10 weeks 1 fetal death (>10 weeks gestation with fetal heart documented) 1 premature birth (<34 weeks gestation) due to pre-eclampsia or placental insufficiency APLS • First described in patients with SLE but now we know • Most APLS do not fulfil criteria for SLE • Those with primary ALSP do not progress to SLE usually • Though clinical features Primary and SLE-associated APLS are similar, the distinction is important and primary APLS should not be labelled as SLE • • • • aPL in general obstetric population is <2% About 30% SLE have aPL About 30% aPL have thrombosis Up to 30% early onset PET have aPL Diagnosis • Two or more positive reading for LA and/or aCL at least eight weeks apart as well as one of features in table Effects of Pregnancy on APLS • Thrombosis risk worsens due to hypercoagulable state of pregnancy • Pre-existing thrombocytopaenia may worsen Effects APLS on Pregnancy • • • • • • First trimester Miscarriage Second trimester fetal loss Third trimester fetal death PET IUGR Abruption Management • Prepregnancy – Screen for aPL if suspicious history – Detailed history of loss to ascertain cause • Antenatal – – – – – – – – – Early booking Viability scanning Low dose aspirin 75mg od and LMWH Switch from warfarin to LMWH by 6 weeks Detailed USS with uterine artery dopplers Serial growth scans Monitor for PET Fetal wellbeing assessment Elective delivery at 37-38 weeks Postnatal Management • Women on long term warfarin may restart on day 2-3 and stop LMWH when INR is 2.0 • All women should have postpartum LMWH for six weeks Thrombophilias • • • • • • Antithrombin III deficiency Activated Protein C resistence Protein C deficiency Protein S deficiency Prothrombin gene mutation Factor V Leiden • May be known or only suspected due to effects Thrombophilias • Risks – – – – – – VTE Recurrent miscarriage Second trimester Pregnancy Loss IUGR Pre-Eclampsia Stillbirth • All less common than in APLS but can still be serious in any individual woman Thrombophilias • Pre-pregnancy – Review history – Change off any medications eg warfarin that are contraindicated in pregnancy – Stop smoking, start folic acid • Early Pregnancy – Aspirin from +ve UPT – Early viability scan 6-8 weeks – Start LMWH OD from +ve fetal heart Thrombophilias • Pregnancy – Regular antenatal care – Anomaly USS +/- uterine artery dopplers – Serial growth scans – Consider early delivery eg 38-40 weeks – Plan stopping aspirin/LMWH prior to labour • Postnatal – LMWH for 6 weeks minimum VTE prophylaxis ASTHMA • Commonest chronic medical illness to complicate pregnancy • Up to 7% women of childbearing age • Often undiagnosed or undertreated Respiratory Changes in Pregnancy • Increased resp rate– Causes resp alkalosis • pH 7.43 (pH 7.40 non-pregnant) • pCO2 4.3 kPa (5.3 kPa) • HCO3- 20.0mmol (24.2 mmol) • Changes in PFTs due to mechanical effects of pregnancy on lungs… Respiratory Changes in Pregnancy • ↑O2 demand-20% • increased consumption • • Tidal volume increases • • (and with small ↑ in respiratory rate= large increase on ventilation-4050% ↑in minute ventilation) • • Inspiratory capacity increases Residual volume decreases Expiratory reserve decreases Marked reduction in functional residual capacity – Diaphragmatic elevation – Increase in subcostal angle and transverse thoracic diameter FEV1 and PEFR are unchanged Respiratory Changes • Increased tidal volume –marked increase in ventilation – Enhanced gas transfer (also helped by improved pulmonary blood flow) – pCO2 is reduced by 15-20% while pO2 is only marginally altered – This is offset by increase in 2,3 DPG in maternal RBC shifts dissociation curve to RIGHT so that maternal O2 saturation changes little – This enhances O2 transfer to fetal RBC which have dissociation curve shifted to LEFT • Fetal Hb much higher affinity for oxygen than adult Hb • Fetal Hb much less sensitive to 2,3 DPG Respiratory Changes • Progesterone effect probably underlies changes in ventilation and reduction in CO2 • Directly on respiratory centre • Increases carbonic anhydrase in maternal RBC – Increased breakdown of CO2 and excretion of HCO3 through maternal kidneys • Functional changes though facilitate airflow along bronchial tree • Women with chronic respiratory disease tend to deteriorate less in pregnancy • Peak expiratory flow and FEV1 can still be valid in pregnant asthmatics • Shortness of breath is common symptom in pregnancy • Individual variations in chemoreceptors • Physiological increase in proportion of blood shunted away from functioning alveoli Effects of Pregnancy on Asthma • May improve, deteriorate or remain unchanged • Mild disease-unlikely to experience problems • Severe disease-greater risk of deterioration, esp in 3rd trimester • Improvement in 3rd trimester may experience postnatal deterioration • Deterioration often due to reduction or cessation of medications due to (unfounded) safety fears Effects of Asthma on Pregnancy • Most women-no adverse effects on pregnancy outcome • Severe, poorly controlled-asthmatics associated with hypoxaemia may adversely affect fetus • Adverse effects on pregnancy rare and associated with poor control – – – – – PIH/PET PTL/birth LBW IUGR Neonatal morbidity eg TTN, hypoglycaemia, seizures, NNU admission Management • Emphasis on prevention rather than treatment • Treatment in pregnancy is no different to nonpregnant women – Optimise control prior to pregnancy – Achieve control asap in new diagnosis – Use of B2 agonist +/- inhaled corticosteroids mainstay Medication Issues • B2 agonists – Safe in pregnancy – Serevent experience growing and ALSO appears safe • No adverse fetal effects reported with the use of the following inhaled drugs – Disodium chromoglycate – Nedocromil – Anticholinergics Medication Issues • Steroids – Inhaled: • minimal absorption • No evidence fetal malformations or adverse fetal effects – Oral • Should not be withheld in acute attacks • No strong evidence of fetal malformations, miscarriage, stillbirth or neonatal death • Will worsen glycaemic control in diabetics or may increase risks GDM with long-term use • Long-term high dose steroids ↑risk premature ROM Acute Asthma Attack • Manage as non-pregnant – – – – IV rehydration O2 B2 agonists as O2 nebuliser (may be repeated) CXR if suspicion pneuthorax/pneumonia or failure to improve – If PEFR fails to improve to >70% predicted, ADMIT – Give steroids JUST AS IF pt was not pregnant! (often inappropriately withheld) – If not improving, may need IV steroids, IV aminophylline or IV B2 agonists Pregnancy Care • Regular antenatal care in conjunction with professional in charge of asthma care • Growth scans only in poorly-controlled disease-if well-controlled, treat as normal • GTT if on oral steroids • Induce only for good obstetric reasons – Induction (PGE2) drugs are NOT contraindicated (they actually act as bronchodilators) Intrapartum Management • No contraindication to induction • If oral steroids for >2 weeks prior to labour, will need IV hydrocortisone • Prostaglandin F2a can cause bronchospasm so should be used with caution (but not withheld if lifethreatening haemorrhage) • All forms of pain relief may be used • Ergometrine associated with bronchospasm-avoid • Encourage breastfeeding to reduce risk of atopic disease in child (1 in 10 or 1 in 3 if both parents atopic) – All drugs discussed above safe in breastfeeding EPILEPSY • About 0.5% women of childbearing age • Most diagnosed (known) prior to pregnancy • All seizure types may be affected by pregnancy • Associated with risks maternal death due to aspiration and SUDEP Effect of Pregnancy on Epilepsy • 25-30% ↑seizure frequency • 54% no change • If seizure free unlikely to have seizures UNLESS stops medications • Poorly-controlled (>1/month) likely to deteriorate in pregnancy • Risk of seizures highest in peripartum period Reasons for Deterioration of Control • Pregnancy • Poor compliance (Fears of teratogenesis) • Decreased drug levels due to nausea and vomiting • Decreased drug levels due to ↑volume of distribution and ↑drug clearance • Lack of sleep towards term and during labour • Lack of absorption of drugs during labour • Hyperventilation during labour Effects of Epilepsy on Pregnancy • Fetus is relatively resistant to short-term hypoxia (during seizures) • No evidence adverse effects • No increased risks of miscarriage or obstetric complications (IUGR, PTL, PET etc) • Status Epilepticus <1% pregnancies BUT dangerous for mum and baby-TREAT VIGOROUSLY! • Major risk is teratogenicity of drugs • Even women on no Rx have ↑risk malformations (4% vs 3% in general population) • Risk of chid developing epilepsy • • • • 5% if either parent has epilepsy 15-20% if both 10% if affected sibling and <2 parents affected 9-12% if parent has idiopathic generalised-only 3% if partial seizures Teratogenic Risks of Anticonvulsants • ALL are teratogenic-newer drugs thought to be safe but now shown to have risks associated with use • Major malformations are: – Neural tube defects (esp valproate 1-2%) and caramazepine (0.51%) – Orofacial clefts (especially phenytion) – Cardiac defects (esp phenytion and valproate) • Minor malformations (fetal anticonvulsant syndrome) – Dysmorphic features (V-shaped eyebrows, lowset ears, broad nasal bridge, irregular teeth) – Hypertelorism – Hypoplastic nails and distal digits Teratogenic Risks of Anticonvulsants • Little difference in risk levels between drugs • Risk for any one drug is 6-7% (2-3x↑) • Risk increases with number of drugs (polypharmacy)- taking 2 or more: risk 15% • If take phenytion, valproate AND carbamazepine, risk to fetus is up to 50% • Benzodiazepines are not teratogenic • Mechanism of teratogenesis though to be folate deficiency – All women should be on high dose folate (5mg/day) preconceptually and throughout pregnancy Management in Pregnancy • Preconceptually: • take folic acid 5mg/day from at least 12 weeks prior to conception • Pregnancy • Continue folic acid throughout as risks folic deficiency anaemia • Continue current drugs if well controlled except • Wean off/change phenobarbitone due to risks of neonatal withdrawal convulsions • Detailed fetal scan at 18-20 weeks with detailed fetal cardiac scan at 22 weeks • Advise shallow bath or shower (risks of drowning if fit) • Relatives advised re: recovery position of fits • If give steroids, ↑dose if enzyme inducing drugs (phenytoin, phenobarbitone, carbamazepine) • Vit K 10-20mg orally from 34-36 weeks if on enzyme inducers due to risks of fetal Vit K deficiency and Haemorrhagic Disease Newborn Intrapartum Management • Most have normal deliveries – LSCS only if recurrent generalised seizures in late pregnancy/labour • Increase in fits around time of delivery – 1-2% fit during labour – 1-2% fit within 24 hours delivery • Continue antiepileptic drugs in labour • Offer early epidural to reduce pain/anxiety Postpartum Management • Neonate should have 1mg IM Vit K • Encourage to breastfeed • Advise re shallow baths/showers-door not locked • Risks of SUDEP ↑ in pregnancy and postnatal period Obstetric Cholestasis • Disease unique to pregnancy • 1% in European womenhigher in women from S Asia • Diagnosis of exclusion • +ve family history in 33% • Thought precipitated by high levels circulating oestrogens • Can recur with COCP Diagnosis • Severe pruritis-limbs and trunk, especially palms and soles • Second half of pregnancy (usually 3rd trimester) • No rash • LFT are abnormal • May be associated dark urine, anorexia, steatorrhoea • If HCV antibody +ve, onset symptoms earlier (mean 29/40) compared to HCV –ve (mean 34/40) Diagnosis 1. Typical history of pruritis without rash 2. Abnormal LFTs 3. Exclusion other causes pruritis and abnormal LFTS • LFTs – – – – Moderate (<3x↑) ALT Raised GGT (20% cases) Mild ↑bilirubin (uncommon) ↑total serum bile acids-may be only abnormality • Pruritis may precede abnormal LFT-serial measurements advised in women with typical persistent itching How to exclude other causes? • Liver USS (presence of gallstones WITHOUT extrahepatic obstruction does not preclude D of OC) • Viral serology (Hep A, B, C, EBV, CMV) • Liver autoantibodies – Anti-smooth muscle Abs for chronic active hepatitis – Anti-mitochondrial Abs for primary biliary cirrhosis Maternal Risks • Vit K deficiency • Increased risk PPH • Iatrogenic interventions Fetal Risks • Intrapartum fetal distress (12-22%) • Amniotic fluid meconium (25-45%) • Spontaneous preterm delivery (12-44%) • Iatrogenic PTD • Intrauterine death • Fetal intracranial haemorrhage Fetal Risks • Reduced from 11% PNMR in early studies to 23.5% more recently • Most recent studies suggest outcomes same to normal population with treatment • • • • Mechanisms of fetal effect not known Increases towards term ?correlate with serum bile acid levels Prediction fetal compromise difficult • No reliable acceptable means (USS, Doppler, CTG) Management • Carefully counsel regarding risks • Regular LFTs and clotting (PT/INR) and BA • Monitor fetal wellbeing – CTGs, Dopplers, USS • Drug treatment – Vit K, antihistamines, ursodeoxycholic acid (UDCA) • Early delivery at 37-38 weeks Drug Therapy • Vitamin K • 10mg orally OD –preferably water soluble preparation • Commence from 32 weeks as risk PTL • Offer to all • Antihistamines • Chlorpheniramine or promethazine may help pruritis • UCDA • Reduces bile abids • Unlicensed in pregnancy but no adverse effects reported • Evidence lacking to support beneficial effect but widely used • Dexamethasone • Can relieve pruritis and lower bile acids-12mg OD orally, evidence lacking, risks associated with steroid therapy Intrapartum Management • If don’t labour spontaneously, induce at 37-38 weeks • Continuous monitoring in labour as risks fetal distress • Neonate should have 1mg IM Vit K at delivery Postpartum Counselling • Recurrence risk is 90% • Avoid oestrogen-containing OCP as may provoke recurrence symptoms – If wishes to use, must monitor LFTs • HRT though does not need to be avoided as only gives physiological levels oestrogens Acute Fatty Liver of Pregnancy (AFLP) • Rare – 1 in 9000-1 in 13000 pregnancies • Potentially lethal – 10-20% maternal mortality – 20-30% perinatal mortality • Some consider as variant PET • Commoner in: – Primigravidae – Male fetus 3:1 – Multiple pregnancy Clinical Features • Presents after 30/40, usually near to term • Gradual onset nausea, anorexia and malaise • Severe vomiting and abdominal pain should alert to diagnosis • Often co-existing features PET but usually MILD • Jaundice appears within 2 weeks onset and there may ascites • LFT abnormal with 310x↑transaminases and raised AlkP • Coagulopathy due to DIC • Associated renal impairment • Polyuria and features diabetes insipidus may occur (AFLP and DI assicated) • May develop fulminany liver failure with hepatic encephalopathy Symptom HELLP AFLP Epigastric Pain + + Hypertension ++ + Proteinuria ++ + Elevated liver enzymes + ++ Hypoglycaemia +/- ++ Hyperuricaemia + +++ DIC + ++ Thrombocytopaenia (no DIC) ++ +/- Raised WCC + ++ USS/CT Normal/Haematoma Normal/steatosis Multiple pregnancy + Primiparous ++ + Male fetus 50% 70% Differentiating from HELLP • See chart • Profound hypoglycaemia (not invariably present) • Marked hyperuricaemia Management • Deliver ASAP • Multidisciplinary team management in ITU • Treat coagulopathy and hypoglycaemia aggressively prior to delivery – Including albumin, FFP, 50% glucose – May sometimes use plasmapheresis • Multiorgan failure may require ventilation and dialysis • Fulminant hepatic failure and encephalopathy should prompt transfer to specialist liver unit – Liver transplantation may be required Outcomes • Prompt reversal of clinical and lab findings usually follows delivery • Significant morbidity is common • May need repeated operations to control PPH due to severe DIC • If survives, complete recovery without longterm liver damage is the norm • Recurrence has been described Any Questions?