Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
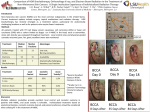
By: Joshua D. Sparling, M.D., F.A.A.D. Franklin Health Dermatology Franklin Memorial Hospital February, 2010 1. I have no financial incentive or conflict of interest from anything which will be discussed in this presentation. 2. This presentation’s purpose is purely to increase public knowledge in skin issues and not for individual diagnosis and treatment. 3. If you have specific questions about your own health, please see your primary care provider first and they may refer you to me or another dermatologist. However, I would be happy to answer general questions at the end of the presentation. 4. Dermatology is by definition a visual field. Some photos may be considered graphic in nature and may be shown without warning. 5. If I use words you don’t understand, please interrupt me! •“ Skin Cancer” does NOT equal “MELANOMA”! • There are 3 main types of skin cancer: •Basal Cell Carcinoma (BCC or BCCA) •Squamous Cell Carcinoma (SCC or SCCA) •Melanoma (Malignant Melanoma or MM) “pearly” or translucent papule (raised growth) typically on the face, ears, shoulders , neck, backs of hands 1.) The good news: BCCA almost never metastasizes! 2.) The bad news: BCCA is more common than ALL OTHER CANCERS COMBINED, and they can be very destructive, as seen above. BCCA makes up about 75% of all skin cancer. 3.) LESSON: HAVE ANY NEW GROWTHS CHECKED OUT AS SOON AS POSSIBLE. •A new growth that bleeds easily or for no reason should always be checked out immediately. •The smaller and sooner a BCCA is diagnosed, the less of a scar and cosmetic or even functional destruction (including nerve damage) will result. •Similar to BCCA but typically faster growing and does not have that “pearly” appearance to it, more “hyperkeratotic” or hard and crusty. •May bleed spontaneously or easily as with BCCA. •Found in generally the same locations as BCCA, the head and neck, ears, and back of the hands. Unlike BCCA , SCCA can grow into “cutaneous horns.” They can get amazingly large! Squamous Cell Carcinoma can be extremely destructive and lead to severe defects and even amputations and infections. Unlike BCCA, SCCA can metastasize and thereby lead to death! There are approximately 250,000 cases of SCCA in the US each year . It accounts for about 20% of all skin cancers. Animals can get skin cancers and SCCA on their noses and mouth Smoking and chewing tobacco can lead to SCCA of the tongue, mouth and throat, which can be devastating. 1.) Exposure to UV light (high cumulative dose of sunshine or tanning bed usage) 2.) Light skin; blonde or light brown hair; green, blue eyes 3.) History of prior nonmelanoma skin cancer 4.) Increasing age 5.) Chronic immunosuppression 6.) Chronic scarring conditions 7.) Human Papilloma Virus (or HPV) infection (specific subtypes) “But doctor I’ve been really good about wearing sunscreen and staying out of the sun for the last decade. How can I have skin cancer now? Skin cancer takes DECADES to develop, which is why young children don’t get nonmelanoma skin cancer. It’s a classic case of PAST sins catching up with oneself. What are they? Also referred to as simply “AKs.” They are pre-skin cancers and are almost ubiquitous over the age of 70 in light skinned people. A certain percentage can progress to become squamous cell carcinoma, which as was mentioned before, can be lethal. Treatment is relatively easy at this stage. Typically, the areas are frozen/treated with liquid nitrogen. Usually, this treatment is considered by most patients to only be slightly painful and heals with little or no scar/discoloration. Most common location is on the face and backs of the hands. However, they can be anywhere that sun has touched the skin, i.e., shoulders, arms, back, legs, etc. Must differentiate from dry skin. 1.) Mohs surgery: reserved for BCCA/SCCA on the ears, lips, around the eyes, and nose and for very large skin cancers : *covered by insurance but extremely expensive *NOT necessary for most skin cancers *only 2 Mohs surgeons in the state of Maine: Freeport and Portland * Cure rate 99% 2.) Excision: standard treatment for most skin cancers. Cure rate 95% 3.) ED+C (Electrodessication and Curettage): Cure rate 92%; only appropriate for BCCA and early SCCA not on the face or scalp 5th most common cancer in men and 6th most common cancer in women Individuals with >100 moles on their body’s are 47 times more likely to develop melanoma Melanomas discovered by a dermatologist vs. the primary care doctor are more likely to be thinner and hence more survivable Once melanoma metastasizes survivability is extremely low (7% 5 year survival rate) Most patients that come into my office and say they have been diagnosed with “melanoma” are mistaken. I want your pathology report – request a copy and please bring it with you to your appointment! A “dysplastic” or “atypical” nevus or mole is NOT the same thing as a melanoma, nor is a “melanoma in situ” or pre-melanoma. As we covered earlier, BCCA and SCCA are NOT the same thing as melanoma and carry a far better prognosis. If you have truly had melanoma, YOU are the one with the disease, so LEARN about it and ask questions!! Know your Breslow depth. Don’t forget the most important letter – E – for Evolution or change! It’s simple. Anyone can do it. It could save your life! Dermatologists’ most important job is to find and eradicate skin cancer. It is for this reason that I offer all my patients referred for a new/changing growth a full skin exam (all clothes off for men and all but the lower underwear in women – I have removed numerous skin cancers on the breasts). Often, I find skin cancers that were not the reason for initial referral. It is your choice to refuse, but a few minutes of potential minor embarrassment could be life saving. There is no cure for psoriasis. For mild psoriasis on small parts of the body, topical steroids are the mainstay of treatment and are the most appropriate. Daily topical moisturization is also critical. For moderate to severe psoriasis where a significant portion of the patient’s body surface area is affected, light therapy is a great option. It has been noted for 1000’s of years that sunlight can improve psoriasis. Psoriasis is one of the earliest known skin diseases. “Leprosy” in the Bible was probably really psoriasis, according to scholars. However, a sun burn can severely flare psoriasis: So, a little sunlight is good, but a lot of sunlight is bad for psoriasis. Why? Scientists have determined that psoriasis is due to one’s immune system overacting , too many T cells in the skin. Small amounts of sunlight or Ultraviolet light downregulate or decrease the local immune system in the skin, thereby improving psoriasis. So, how about tanning? Tanning is not safe. The tanning industry is poorly regulated and the amount of ultraviolet light exposure is widely variable. One can EASILY burn or get too much exposure and worsen psoriasis. Tanning booth employees are NOT trained to treat psoriasis, nor is the type of ultraviolet light the best for psoriasis patients. It is also much more likely to lead to skin cancer than the light therapy used in a dermatologist’s office. Light therapy or Narrow Band Ultraviolet Light B (NBUVB) is not for every psoriasis patient. It requires 2-3 times per week visits to use the booth. It carries a small increased risk for long-term skin cancer. Therefore, it should not be used for patients with localized or mild psoriasis who “just don’t like having to apply topical steroids.” Many “rashes” are truly just dry skin. Most people NEED to use a moisturizer EVERY DAY in the winter to prevent and improve rashes/dry skin. I recommend Vanicream. Many rashes that are not dry skin are due to allergic or irritant contact reactions from over-the-counter products and even prescriptions from well-meaning primary care doctors. Simplify, simplify, simplify. Use only Vanicream, Aquaphor, Vaseline, or Cetaphil and you can’t go wrong. Cetaphil should be used as a soap-substitute for all body soap and face wash. Shampoo: California Baby Shampoo (Target stores in the baby section), next best is J+J Baby Shampoo. If none of this works, consider a change in your environment or situation. Consider seeing an allergist, if you also have upper respiratory symptoms. Contrary to popular belief, dermatologists cannot always figure out what’s causing a rash. You need to play an active role in figuring it out! By far most hair loss is genetic Your hair loss is most likely genetic if you have had gradual hair loss, non-scarring hair loss, diffuse hair loss, no redness of the scalp, on few/no oral medications, have a healthy diet, are otherwise healthy (few chronic medical issues) and have a family history of hair loss (male of female ). However, there are many non-genetic causes of hair loss which was treatable and reversible, so lab evaluation is necessary, but don’t be surprised if the labs are normal and the cause is ultimately found to be genetic. Some of the non-genetic causes of hair loss that your doctor can evaluate include the following: *thyroid or liver disease *protein deficiency and anemia (common with vegetarian diets) *hepatic or renal failure *anorexia or bulimia *too much vitamin A or other extreme diets *childbirth *local fungal infection (ringworm) *starting or stopping birth control pills *stress or high fever *some medications: chemotherapy, bromocriptine , beta blockers, ACE inhibitors, amphetamines, anticholesterol agents *lupus or other autoimmune disease Alopecia areata -- focal smooth hair loss, no redness Tinea capitis or ringworm – red, angry, tender hair loss Diffuse hair loss from a metabolic disorder or medications – The entire scalp hair is evenly affected Males and females loose hair in different places on the scalp. Males lose hair first at the temples and frontal forehead and have a receding hair-line. Then, the hair is lost on the crown. Females lose hair starting on the crown and vertex of the scalp and typically do not lose Hair in the front. They will also eventually lose hair diffusely and the hair will become thin throughout the scalp. Thank you!!