Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
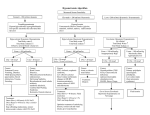
Fluid and Electrolyte Emergencies in Critically Ill Children Ahmed Khamis Bamaga MBBS Objectives At the end of this presentation learners will be able to: • 1) Recognize common fluid and electrolyte disorders in critically ill children • 2) List a diagnostic strategy for these disorders • 3) Apply appropriate management principles Case Study #1 • HPI: • A 3 month-old is in the PICU for shock following a two day history of fever and irritability. Blood and CSF cultures are positive for Streptococcus pneumoniae. • Hospital course: • Decreasing urine output (< 0.5 ml/kg/hr) over the last 24 hours. Case Study #1 What is your differential diagnosis? What diagnostic studies would you order? Case Study #1 Differential diagnosis Oliguria 1) Pre-Renal (decreased effective renal blood flow) Diminished intravascular volume, cardiac dysfunction, vasodilitation 2) Post-Renal Outlet obstruction (intrinsic vs. extrinsic), foley catheter occlusion 3) Renal Acute tubular necrosis, acute renal failure, SIADH, ... Case Study #1 Laboratory studies Serum studies Sodium 126 mEq/L Chloride 98 mEq/L Potassium 3.7 mEq/L Bicarbonate 25 mEq/L BUN 4 mg/dL Creatinine 0.4 mg/dL Glucose 129 mg/dL Osmolality 260 mosmol/kg Urine studies Specific gravity 1.025 Osmolality 645 mosmol/kg Sodium 58 mEq/L FeNa 2.4% What are the primary abnormalities? Case Study #1 Laboratory studies Major abnormalities 1) Hyponatremia 2) Oliguria (inappropriately concentrated urine) What is the most likely explanation for these findings? Case Study #1 Syndrome of Inappropriate Antidiuretic Hormone (SIADH) • Variable etiology • • • • • • • • • Trauma Infection Psychosis Malignancy Medications Diabetic ketoacidosis CNS disorders Positive pressure ventilation “Stress” Case Study #1 SIADH • Manifestations • By definition, “inappropriate” implies having excluded normal physiologic reasons for release of ADH: • 1) In response to hypertonicity. • 2) In response to life threatening hypotension. • Hyponatremia • Oliguria • Concentrated urine • elevated urine specific gravity • “inappropriately” high urine osmolality in face of hyponatremia • Normal to high urine sodium excretion Case Study #1 SIADH • Diagnosis • Critical level of suspicion. • Demonstration of inappropriately concentrated urine in face of hyponatremia urine osmolality, SG, urine sodium excretion ( FeNa) • Be certain to exclude normal physiologic release of ADH Frequently secondary to decreased perfusion Serum sodium, urine osmolality, urine sodium excretion (low FeNa) consistent with dehydration or diminished renal blood flow. Look at patient more closely !! Case Study #1 SIADH • Treatment • Fluid restriction. • 50-75% of maintenance requirements, be certain to include oral intake. • Daily weights. Case Study #1 The saga continues…. Hospital course: Four hours after beginning fluid restriction, you are called because the patient is having a generalized seizure. There is no response to two doses of IV lorazepam (Ativan®) and a loading dose of fosphenytoin (Cerebyx®) What is the most likely explanation? Case Study #1 The saga continues Seizure 1) Worsening hyponatremia 2) Intracranial event 3) Meningitis 4) Other electrolyte disturbance 5) Medication 6) Hypertension What diagnostic studies would you order? Case Study #1 The saga continues Stat labs: Sodium 117 mEq/L What would you do now? Case Study #1 Hyponatremic seizure • Treatment • Hypertonic saline (3% NaCl) infusion • To correct sodium to 125 mEq/L, the deficit is equal to (0.6)(weight[kg])(125- measured sodium) (0.6)(8)(125-117) = 38.4 mEq • Because patient is symptomatic with seizures, immediately increase serum sodium by 5 mEq/L mEq sodium = (0.6)(8 kg)(5) = 24 mEq • 3% NaCl = 0.5 mEq/L, therefore 24 mEq bolus = 48 mls, followed by slow infusion of remaining 14.4 mEq (29 mls) over next several hours Case Study #2 HPI: A 5 month-old girl presents with a one day history of irritability and fever. Mother reports three days of “bad” vomiting and diarrhea. Home meds: Acetaminophen and ibuprofen for fever PE: BP 70/40, HR 200, R 60, T38.3 C. Irritable, sunken eyes and fontanelle, skin feels like Pillsbury Dough Boy Case Study #2 No one can obtain IV access after 15 minutes, what would you do now? Case Study #2 Place intraosseous line Bolus 40 ml/kg of isotonic saline Reassessment (HR 170, RR 40, BP 75/40) Serum studies Sodium 164 mEq/L Chloride 139 mEq/L Potassium 5.5 mEq/L Bicarbonate 12 mEq/L pH 7.07 pCO2 11 pO2 121 HCO3 8 BUN 75 mg/dL Creatinine 3.1 mg/dL Glucose 101 mg/dL Case Study #2 What is the most likely explanation of this patients acidosis? Case Study #2 Metabolic acidosis and the anion gap Anion Gap Sodium - (chloride + bicarbonate) Normal 12 +/- 2 meq/L Elevated anion gap consistent with excess acid Normal anion gap consistent with excess loss of base 164 - (139 + 12) = 13 Case Study #2 Metabolic acidosis and the anion gap 1. Normal gap 1. Renal “HCO3” losses Proximal RTA Distal RTA 2. GI “HCO3” losses Diarrhea 2. Increased gap 1. Acid prod Lactate DKA Ketosis Toxins Alcohols Salicylates Iron 2. Acid elimination Renal disease Case Study #3 • HPI: • A five year old (18 kg) boy was involved in a a motor vehicle accident two days ago. He sustained an isolated head injury with intraventricular hemorrhage and multiple large cerebral contusions. Three hours ago, he had an episode of severe intracranial hypertension (ICP 90mm Hg, MAP 50mm Hg, requiring volume plus epinephrine infusion for hypotension. Over the last two hours, his urine output has increased to 130-150 ml/hour (~8ml/kg/hr). What is your differential diagnosis? What test would you order? Case Study #3 Differential diagnosis Polyuria 1) Central diabetes insipidus Deficient ADH secretion (idiopathic, trauma, pituitary surgery, hypoxic ischemic encephalopathy) 2) Nephrogenic diabetes insipidus Renal resistance to ADH (X-linked hereditary, chronic lithium, hypercalcemia, ...) 3) Primary polydipsia (psychogenic) Primary increase in water intake (psychiatric), occasionally hypothalamic lesion affecting thirst center 4) Solute diuresis Diuretics (lasix, mannitol,..), glucosuria, high protein diets, post-obstructive uropathy, resolving ATN, …. Case Study #3 Laboratory studies Serum studies Sodium 155 mEq/L Chloride 114 mEq/L Potassium 4.2 mEq/L Bicarbonate 22 mEq/L BUN 13 mg/dL Creatinine 0.6 mg/dL Glucose 86 mg/dL Serum osmolality: 320 mosmol/kg Other Urine specific gravity 1.005, no glucose. Urine osmolality: 160 mosmol/kg What are the main abnormalities? Case Study #3 Laboratory studies Major abnormalities 1) Hypernatremia 2) Polyuria (inappropriately dilute urine) What is the most likely explanation? Case Study #3 Diabetes Insipidus Diagnosis Central Diabetes insipidus 1) Polyuria 2) Inappropriately dilute urine (urine osmolality < serum osmolality) May be see with midline defects Frequently occurs in brain dead patients What should you do to treat this child? Case Study #3 Diabetes Insipidus • Treatment • Acute: Vasopressin infusion - begin with 0.5 milliunits/kg/hour, double every 15-30 minutes until urine flow controlled • Chronic: DDAVP (desmopressin) • Warning • Closely monitor for development of hyponatremia Case Study #4 HPI: A six year old, 25 kg, boy with severe asthma (S/P ECMO for a previous exacerbation) presents with a two day history of severe vomiting and diarrhea to the Emergency Department. Home meds: Albuterol MDI two puffs QID, Salmeterol MDI two puffs BID, Prednisone 10mg daily, Fluticasone 220 mcg two puffs BID PE: BP 70/40, HR 168, R 40, T39.0 C. He is very lethargic (GCS 11). Poor perfusion with cool extremities, mottling, and delayed capillary refill, otherwise no specific system abnormalities. Case Study #4 What is your differential diagnosis? What diagnostic studies would you order? Case Study #4 Differential diagnosis Shock 1) Cardiogenic Myocarditis Pericardial effusion 2) Hypovolemic Hemorrhage, excessive GI losses, “3rd spacing” (burns, sepsis) 3) Distributive Sepsis, anaphylaxis Case Study #4 Laboratory studies Serum studies Sodium 130 mEq/L Chloride 99 mEq/L Potassium 5.7 mEq/L Bicarbonate 12 mEq/L BUN 43 mg/dL Creatinine 0.6 mg/dL Glucose 48 mg/dL Other WBC: 13k (60% P, 30% L), HCT 35%, PLT 223k Chest radiograph: no abnormalities What are the electrolyte abnormalities? Case Study #4 Diagnosis Major abnormalities 1) Hyponatremic dehydration 2) 3) 4) 5) Hypoglycemia Hyperkalemia, mild Acidosis Azotemia What is the most likely explanation for these findings? Case Study #4 Adrenal Insufficiency • 1o adrenal insufficiency (Addison’s disease) • Adrenal gland destruction/dysfunction (ie. autoimmune, hemorrhagic) • most common in infants 5-15 days old • 2nd adrenal insufficiency • ACTH deficiency (ie. panhypopituitarism or isolated ACTH) • “Tertiary” or “iatrogenic” • Suppression of hypothalamic-pituitary-adrenal axis (ie. chronic steroid use) Case Study #4 Adrenal Insufficiency • Manifestations • Major hormonal factor precipitating crisis is mineralcorticoid deficiency, not glucocorticoid. • Dehydration, hypotension, shock out of proportion to severity of illness • Nausea, vomiting, abdominal pain, weakness, tiredness, fatigue, anorexia • Unexplained fever • Hypoglycemia (more common in children and tertiary) • Hyponatremia, hyperkalemia, azotemia Case Study #4 Adrenal Insufficiency • Diagnosis • Critical level of suspicion in all patients with shock • 1) Demonstration of inappropriately low cortisol secretion • Basal morning level vs. random “stress” level • 2) Determine whether cortisol deficiency dependent or independent of ACTH secretion. • ACTH, cortisol 1o adrenal insufficiency • ACTH, cortisol 2nd or tertiary insufficiency • 3) Seek a treatable cause Case Study #4 Adrenal Insufficiency • What should you do to treat this child? Case Study #4 Adrenal Insufficiency • Treatment • Do not wait for confirmatory labs • Fluid resuscitation - isotonic crystalloid • Treat hypoglycemia • Glucocorticoid replacement - hydrocortisone in stress doses - 25-50 mg/m2 (1-2 mg/kg) IV • Consider mineralocorticoid (Florinef®) Case Study #5 • HPI: • An eight month old infant with autosomal recessive polycystic kidney disease presents with irritability. She is on nightly peritoneal dialysis at home. The lab calls a panic potassium value of 7.1 meq/L. The tech says it is not hemolyzed. What do you do now? Case Study #5 Hyperkalemia • Treatment • Immediately repeat serum potassium. Do not wait for confirmatory labs especially if EKG changes present. • Anticipatory Stop potassium administration including feeds Cardiac Monitor • What is this rhythm? • What is your immediate treatment? Case Study #5 Hyperkalemia • Treatment (cont) • Control effects • Antagonism of membrane actions of potassium Calcium chloride 10-20 mg/kg over 5 minutes; may repeat x2 • Shift potassium intracellularly Glucose 1 gm/kg plus 0.1 unit/kg regular insulin Alkalinize (increase ventilator rate; Sodium bicarbonate 1 mEq/kg IV) Inhaled 2 adrenergic agonist (albuterol) • Removal of potassium from the body Loop / thiazide diuretics Cation exchange resin: sodium polstyrene sulfonate (Kayexelate®) 1 gm/kg PO or PR (or both) Dialysis Case Study #6 • HPI: • A three year old boy is recovering from septic shock. He received 150 ml/kg in fluid boluses in the first 24 hours and has anasarca. You begin him on a bumetanide infusion (Bumex®) for diuresis. He develops severe weakness and begins to hypoventilate. You notice unifocal premature ventricular beats on his cardiac monitor. What is your differential diagnosis? What tests would you order? Case Study #6 Laboratory studies Serum studies Sodium 134 mEq/L Chloride 98 mEq/L Potassium 2.4 mEq/L Bicarbonate 27 mEq/L BUN 11 mg/dL Creatinine 0.4 mg/dL Calcium 9.2 mg/dL Phosphorus 3.2 mg/dL Other EKG: Unifocal PVC’s What is the main abnormality? Case Study #6 Laboratory studies Major abnormality 1) Hypokalemia What would you do now? Case Study #6 Hypokalemia • Treatment • Oral • Safest, although solutions may cause diarrhea • IV • Peripheral: do not exceed 40-50 mEq/L potassium - Avoid temptation to rapidly bolus • Central: 0.5 -1 mEq/kg over 1-3 hours, depending on severity • Replace magnesium also if low • (25-50 mg/kg MgSO4) Summary • Disorders of sodium, water, and potassium regulation are common in critically ill children • Diagnostic approach must be considered carefully for each patient • Strict attention to detail is important in providing safe and effective therapy