Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
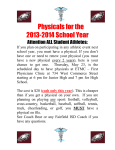
General Medicine Clinic Care Management Program Fern Ebeling, RN Lisa Tang, MEA Lindsay Evans, LCSW Julia Finch, BA Elizabeth Davis, MD Mr. P is a 49 year old man with congestive heart failure, active methamphetamine use, depression, severe coronary artery disease, and bilateral pulmonary emboli. Over the year prior to enrolling in our program he had been admitted three times (23 hospital days). He frequently missed appointments and did not regularly take his medications. General Medicine Clinic San Francisco General Hospital, UCSF SNAPSHOT OF OUR CLINIC Complex Care Management Team Level 3: Complex healthcare needs Level 2: Multiple chronic conditions: diabetes, HTN, COPD Level 1: Uncomplicated chronic disease or risk factors: obesity, pre-diabetes GMC Care Management Team Roles Team member Roles RN Care Manager Medical Assistant Health Coach Provider (Resident, attending, or NP) Initial assessment and Care Plan Complex clinical issues and medication issues Clinical back-up for Health Coach Outreach to patients Coaching toward care plan goals Focus on self-management Primary point of contact for patients Refer patients Collaborate with CM team Titrate medications, plan diagnostic work ups Coordinator Manages referrals, data tracking, reporting Social Worker Referrals to entitlements and community-based programs Physician CM lead Program development and evaluation Clinical back-up to team Lead quality improvement Home Assessment • Chart Review • Trust building • Self Management • Medication Reconciliation • Function • ADLs/IADLs • Social Support • Get family involved • Behavioral Health • Depression Screening • Substance Use • Safety • IPV and Elder Abuse screen • Home safety GMC Care Management Program: Enrollment and Levels of Care ASSESSMENT: The team RN and health coach conduct a comprehensive assessment, either in the home, in clinic, or by phone. From this information, they develop a care plan and assign the patient a level of care. CRITICAL CRITICAL Intensive case case mgmt mgmt in in Intensive st nd and 22nd wk wk postpost11st and discharge. discharge. or == 1x/wk 1x/wk check-ins check-ins >> or LEVEL LEVEL 11 Check-ins every every 22 wks wks Check-ins LEVEL LEVEL 22 WAIT LIST INITIAL CONTACT AND CHART REVIEW ASSESSMENT Check-ins every every 33 wks wks Check-ins LEVEL LEVEL 33 Monthly check-ins check-ins Monthly LEVEL LEVEL 44 PT DECLINED HAS OTHER SERVICES LEVELS OF CARE: The assigned level of care determines the intensity of our care management for each patient. Patients can move up and down the levels of care at any time depending on need. Pt calls calls team team PRN PRN Pt LEVEL LEVEL 55 GRADUATE Pt graduated graduated from from Pt program program Health Coaching • • • • • • Done over the phone • Freq depends on status Check-in Problem-solving • Pharm • DME • Appts Motivational Interviewing Role modeling Patient Education/Symptom Management • Health-O-Meters Health-O-Meter Mr. P, four months later • • • Upon enrollment to our program, we focused on building a relationship with Mr. P and with his family. He was hesitant about working with our team, but after three months of intensive involvement, he began to engage. He now feels comfortable calling us with his concerns. Over the first four months, we had 43 conversations with him and his family and had 6 in-person visits. We then decreased to much less frequent contacts. He has had no ED visits or admissions since enrolling in our program, and he has attended almost all of his appointments. At one of these visits, his primary care provider said “This is the first time I have seen him stable. He looks like a different person!” GMC Care Management Challenges Challenge Strategies Capacity •Assigning patients to levels •Weekly team discussion Engagement •System for deciding when to stop trying to engage •Learning from other programs Communication with PCPs •Email questions in bold •Huddles •Brochure •Case conferences GMC Care Management Lessons Learned • • • • • • • Interprofessional teams embedded in primary care Efficient data management Dashboard key to ongoing improvement Improvement in utilization and health despite complexity Effective care management takes time Partnership with local partners and stakeholders Patient Advisory Board Resident and Provider Experience • • All providers surveyed thought quality of care improved with care management "The largest impact that having teams at the GMC has had on me is this feeling that I'm not on my own advocating and caring for our patients--and that has been a huge emotional burden lifted." Patient Experience • “Another thing that makes me feel good is when people like Lisa and Fern and Dr. Hurstak reach goals with me. I know there’s someone on the other side fighting for me. I’m not by myself…They convinced me with facts that they are an asset for the patient’s care because they are always there for you.” GMC Care Management Outcomes Year prior to During CM enrollment in CM Percent reduction Hospital days per year per patient 9.75 4.53 53.5% ED Visits per year per patient 3.40 2.49 26.6% Utilization data for all patients who have been enrolled in Care Management (n=73). One patient was excluded from this analysis due to incomplete hospitalization data. Utilization data for patients in the program for less than one year was annualized. Key Stakeholders and Partnerships • SFGH and the SF Department of Public Health • Training from UCSF Center for Excellence in Primary Care • San Francisco Health Plan (Medicaid managed care) • Health at Home • In Home Supportive Services Thank you!