Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
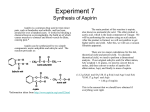
2008 Performance Improvement Project: Improving the documented use of aspirin in MSHO/MSC/MSC+ seniors with diabetes or ischemic heart disease Developed by Jackson Thatcher MD FACC FSCAI Presented by Theresa Zeman NP 2008 Performance Improvement Project Scope, Evidence & Disclosures The scope of this project is limited to seniors age 65-84 covered under the senior Medicaid plans: Minnesota Senior Health Options (MSHO), Minnesota Senior Care (MSC) or Minnesota Senior Care Plus (MSC+) The scientific statements in this PowerPoint are drawn from the Project Executive Summary and References and ACC-AHA Cardiovascular Disease Guidelines Why Diabetics and Patients with Vascular disease? Diabetics have a comparable risk of MI to that of matched non-diabetics with prior MI All diabetics and patients with vascular disease have an evidence-based guideline supported Class I indication for aspirin Why Aspirin? Aspirin is fundamental to the care of patients with cardiovascular disease Why Aspirin? There are very few patients with an absolute contraindication to aspirin Approximately 98% of patients may have a trial of aspirin therapy when indicated Why Aspirin? Aspirin is the only essential drug used in vascular disease and diabetes that is not well documented by claims data Claims data indicate senior Medicaid patients and their providers fail to use the OTC aspirin benefit provided by their plan Why Aspirin? Poor utilization of the senior Medicaid OTC aspirin benefit leaves aspirin use grossly under documented Many of these undocumented seniors are probably taking aspirin, but could utilize their OTC benefit to obtain their aspirin at little or no cost Why Aspirin? Utilizing the senior OTC aspirin benefit would provide data documenting the quality of care in eligible patients Platelets and Thrombosis Platelets are small cell-like particles in the blood that help patch leaks and promote blood-clotting In diseased arteries platelet thrombi (clumps) can completely block the narrowed vessel resulting in stroke or heart attack Platelets and Thrombosis Cholesterol rich Plaque Platelet Clump (White Thrombus) usually at a site of plaque fibrous cap rupture Thin fibrous cap prone to rupture So what happens if this occurs? Plaque rupture results in platelet activation Activated platelets release chemical signals that allow other platelets to attach So what happens if this occurs? Platelets release additional chemicals that constrict blood vessels slowing blood flow and allowing more platelets to accumulate Activated platelets start the clotting cascade and red clot forms So what happens if this occurs? Platelet thrombi (clumps) break loose from the white clot and embolize (clog) small branches downstream causing microvascular occlusion which results in rest angina (chest pain at rest) and eventual injury to heart muscle The entire vessel may close resulting in a full-blown heart attack Plaque Rupture Factors promoting plaque rupture (wall stress, inflammation, thin cap and large lipid core) Platelet thrombus (white clot) Platelet embolus Developing thrombin and blood cell clot (red clot) Fibrous plaque Semi liquid lipid core under thin cap Extruded lipid after cap rupture Angiogram of Acute Myocardial Infarction Acutely occluded right coronary artery Angiogram of Acute Myocardial Infarction Partial flow restored Angiogram of Acute Myocardial Infarction After stenting restored full blood flow stopping further damage to heart muscle Angiogram of Acute Myocardial Infarction Heart pumping after normal blood flow restored So How Does Aspirin Reduces the Risk of Heart Attacks and Strokes? Aspirin irreversibly binds to cyclooxygenase (COX-1) on the platelet Aspirin blocked COX-1 cannot catalyze the formation of thromboxane A-1, which stimulates platelet activation How Aspirin Reduces the Risk of Heart Attacks and Strokes Aspirin treated platelets are much less likely to activate and clump together Since there are over 80 separate pathways that initiate platelet activation aspirin therapy is not 100% effective in stopping platelet activation and clumping How Drugs Reduce the Risk of Heart Attacks and Strokes Some other agents that reduce platelet clumping include: (Plavix®) Didpyridamole (Persantine®, and combined with aspirin in Aggrenox®) Intravenous glycoprotein receptor inhibitors such as abciximab (ReoPro®) or eptifibitide (Integrilin®) Clopidogrel How Drugs Reduce the Risk of Heart Attacks and Strokes Some other agents that reduce platelet clumping include: Omega-3 fatty acids (Fish Oil) Some calcium channel blockers Beta-blockers Nitrates Fibrin split products - created when streptokinase is used as a thrombolytic (‘clot busting’ drug) How Many Seniors are at Risk? Risk increases in lower income populations Substantial numbers of seniors have lower income How Many Seniors are at Risk? A healthy lifestyle: principally reduced smoking and blood pressure treatment delays the onset of vascular disease until later in life But vascular disease remains a leading cause of morbidity and mortality even in seniors who were considered healthy through middle age How Many Seniors are at Risk? Hypertension, obesity, dyslipidemia and type 2 diabetes (metabolic syndrome) pose potent increasing risk factors in the elderly 20% of seniors are currently diabetic This number may approach 40% as the obesity epidemic peaks in seniors Seniors who live long enough will likely develop vascular disease What is the Current Data for Use? Patients with prior MI or diabetic patients have a 20% risk of new/recurrent cardiovascular events within 3 years Patients with diabetes and prior MI have a risk of over 45% What is the Current Data for Use? Aspirin use lowers that risk by about 25% 35% reduction nonfatal MI 25% reduction nonfatal stroke 15% reduction in vascular and other cause of death What is the Current Data for Use? For every 1000 indicated individuals treated with low dose aspirin, 10-20 fewer vascular events are expected each year What is the Risk of Treatment? Aspirin causes serious bleeding including hemorrhagic stroke in 1-2% of patients treated with low dose aspirin What is the Risk of Treatment? Statistically, unless vascular disease or diabetes is present low dose aspirin therapy provides no benefit in men prior to age 50 and no benefit in women prior to age 60 What is the Risk of Treatment? Seniors with vascular disease or diabetes have unequivocal benefit unless excess risk is identified So I have Good News and Bad News, Which news do you want first? Lecturer’s prerogative First the Bad News The Bad News Medicine can be expensive OK then, so what’s The Good News? The Good News At least we can afford aspirin Relative Generic Costs per Year Aspirin $5.00 X Lisinopril $30.00 6X Carvedilol (Target/Sam’s) $48.00 10X Lovastatin (Target/Sam’s) $48.00 10X Metoprolol (QD formulation) $75.00 15X Simvastatin $200.00 40X Atorvastatin (not generic) $1300.00 260X Clopidogrel (not generic) $1900.00 380X What are the Current Criteria for Use? What is Anticipated in the Future? Aspirin, along with beta-blocker, converting enzyme inhibitor and a statin are AHA-ACC Guideline Indicated (Class 1) in vascular disease and diabetes unless contraindicated Studies in diabetics like the ACCORD trial examining the results of optimal glucose control on top of hypertension control, lipid treatment, beta blocker, and aspirin therapy may reduce cardiovascular events by over 50% results anticipated by 2011 Where Does All This Lead? A recent early report from ACCORD indicates that the most aggressive glucose lowering arm: HgBA1c < 6.5 was associated with more deaths than standard care: HgBA1c < 7.4 Because of this the treatment arm was softened to aim for an HgbAIc < 7.0 Where Does All This Lead? While aggressive glucose lowering may not have been tolerated by some, researchers expect both arms will do better than ‘average’ care which still tends to be suboptimal. MCOs don’t need to wait until 2011 to prepare to compare their results in their ‘average’ diabetics to the ACCORD populations and see where they stand Where Does All This Lead? If we plan now we could have a real jump on a DHS Senior performance improvement project for 2011! Changing Lanes Moving from what we need to do, To what may make it difficult to accomplish Despite our best effort, tools, and successes to date Why is ASA Treatment Documentation so Poor? As an OTC product aspirin is not routinely administered via written prescription Why is ASA Treatment Documentation so Poor? Although DHS provides an OTC aspirin benefit for Medicaid patients, CMS does not cover OTC products for Part D-Medicare patients Why is Aspirin Treatment Documentation so Poor? While providers may prescribe aspirin for eligible patients they are: Why is Aspirin Treatment Documentation so Poor? Largely unaware of the benefit and Unlikely to remember to use it Common reason for non-use: Majority of patients seen by providers don’t need or cannot make use of an aspirin prescription - it’s just not something a busy provider will automatically think of Providers ≠ Physicians Providers include: Physicians MDs DOs Mid Level Providers (MLPs) Physician Assistants Nurse Practitioners Advanced Practice Nurses Workable solutions for this problem must include all care providers So how do we make a measurable improvement? Educating all Minnesota providers to write OTC aspirin prescriptions for all eligible patients will prove a difficult task Getting all eligible patients to submit this prescription may also prove difficult They may already have aspirin at home They may forget to bring the prescription since it is not required to obtain the medication and aspirin is inexpensive So how do we make a measurable improvement? Clinicians will often provide what a patient requests Such as an aspirin prescription So how do we make a measurable improvement? Care Coordinators can help by ensuring all eligible patients are aware of the benefit Patients must understand their use of the aspirin prescription benefit will also document their receipt of Best Care Assisting the clinician with the name/fax+phone number of the patient’s preferred pharmacy might expedite the process So how do we make a measurable improvement? While the preferred contact with the provider is an office visit, situations will arise in which patient transport or provider availability limit access within a reasonable timeframe This may result in a phone contact whether from the patient or the coordinator in order to obtain the prescription So how do we make a measurable improvement? Assisting the clinician’s office staff by providing 2 patient identifiers, such as name and birthdate as well the fax + phone number of the patient’s preferred pharmacy may expedite and reduce the hassle of another office call So how do we make a measurable improvement? In process improvement an average solution that is very well executed will always beat a better solution that is not well disseminated or multiple conflicting solutions So how do we make a measurable improvement? Work hard Never give up If the first plan fails consider alternative solutions Why We Fight… to improve healthcare Why We Fight is the national leader in reducing cardiovascular death Minnesota without peer Why We Fight This success is shared by our hardworking & healthy general population It includes public health success in reducing smoking rates and second-hand smoke Why We Fight It also includes our progressive employers who realize the benefits of insuring for a healthy workforce And our managed care organizations who have stressed preventive services and healthy lifestyles to reduce the costs of disease management Why We Fight Along with our tireless providers: physicians, mid-levels, and nurses who have embraced evidence-based medicine and stressed broad application of guideline indicated therapies across diverse patient populations Why We Fight Our hospitals that have focused on coordinated, fast and efficient care with a passion to reduce medical error Why We Fight And finally, our informed and educated patients who ask the right questions and are fully vested in seeing they receive optimal healthcare Why We Fight But our work isn’t finished until we fully address one of the greatest discriminations against the poor of our state - Why We Fight But our work isn’t finished until we fully address one of the greatest discriminations against the poor of our state - poor healthcare Promoting the use of the OTC aspirin benefit in covered Medicaid seniors Is a big step in the continuing effort to provide superior healthcare to all Minnesotans Good Luck with your project Improving the documented use of aspirin in MSHO/MSC/MSC+ seniors with diabetes or ischemic heart disease Questions