Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
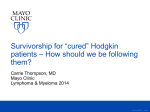
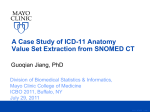
Joint PREP Class Shoulder Replacement T. Andrew Israel MD Mayo Clinic Health System Adult Reconstruction Goals for you and your family • Recognize shoulder replacement is a reliable operation to improve quality of life • Describe what to expect of the shoulder replacement procedure. • Discuss the risks of shoulder replacement surgery. ©2011 MFMER | slide-2 Goals of Your Shoulder Replacement • Improve your quality of life by: • Relieve your pain • Improved motion • Improved strength • Better function ©2011 MFMER | slide-3 Shoulder Joint Replacement Indications • Bone on bone osteoarthritis • Intact rotator cuff tendons Shoulder Arthritis • Loss of cartilage leads to narrowing of the joint space ©2011 MFMER | slide-5 Shoulder Arthritis • As the cartilage wears, bone spurs form and the shoulder becomes stiff ©2011 MFMER | slide-6 Surgical Technique of Total Shoulder Replacement • Replaces the worn bony surfaces with metal ball and plastic socket (glenoid) • Restores shoulder motion and stability ©2011 MFMER | slide-7 Hemiarthroplasty • A metal ball and stem go down into the humerus. • No plastic socket is placed. ©2011 MFMER | slide-8 Reverse Total Shoulder Indications Replacement Components • Completely torn rotator cuff with severe arthritis • Complex fractures • Previous failed shoulder replacement REVERSE TOTAL SHOULDER • Socket and ball are reversed • Humeral head (ball) becomes the socket • Glenoid (socket) becomes the ball ©2011 MFMER | slide-10 Surgical Technique Incision • The incision is made in the front of the shoulder • Your surgeon will make the incision long enough to see the joint area • Your surgeon will use techniques to spare muscle • Surgical techniques continue to improve as technology advances ©2011 MFMER | slide-11 Day of Surgery • Your surgeon will meet you in the Surgical Prep and Recovery area to initial your shoulder and answer final questions. • Family can wait with you in the Surgical Prep and Recovery area. • You will go to the Operating Room (OR). Surgery lasts 2 hours. • You will then go to the recovery room for 1-2 hours. ©2011 MFMER | slide-12 After Surgery in the Hospital Occupational Therapy is critical for a good outcome • Therapy will visit after surgery to educate you on practicing activities of daily living • Wear an arm sling immobilizer full time for 6-8 weeks • No forceful contraction of muscles such as pushing up out of chair or bed. • Follow the exercise program as instructed ©2011 MFMER | slide-13 Shoulder precautions • Do not overdo it! Early overuse may result in severe limitations of motion • Do not lift anything heavier than a glass of water for the first 68 weeks • Do not participate in contact sports or any repetitive heavy lifting after your shoulder replacement. • Avoid placing your arm in any extreme position for the first 68 weeks ©2011 MFMER | slide-14 Other Doctors in the hospital • Additional Doctors take care of non-orthopedic issues (such as high blood pressure or diabetes). • If you have an Internal Medicine doctor here, they will see you after surgery. • If your regular doctor does not see patients in the hospital, a Hospitalist will see you after surgery. • If you are not getting a medication you think you should, please ask. ©2011 MFMER | slide-15 Risks of Surgery Anesthetic Complications • Anesthesia providers meet with you the day of surgery. • They discuss anesthetic options for postoperative pain relief. • Nausea and vomiting are common but more serious side effects or complications may occur. • Please tell the anesthesia provider of any past experience with anesthesia. ©2011 MFMER | slide-16 Risks of Surgery Blood Clots • Lower risk for blood clots with total shoulder replacement • Clots can go to the lungs and be fatal • Your risk is reduced to <1% if treated with medication (aspirin) ©2011 MFMER | slide-17 Blood Clot Prevention • Enteric coated aspirin 325 mg twice a day while in hospital to prevent blood clots. Continue at home for 3 weeks. • SCDs (calf squeezers) are on in the hospital whenever you are in bed. • Exercising your legs and being up and walking promotes blood flow. ©2011 MFMER | slide-18 Risks of Surgery Infection • You will get antibiotics at the time of surgery and for 24 hours after surgery. • Surgeons, assistants and scrub techs wear “spacesuits.” • Using all precautions, risk of infection is ~1%. • Infection may occur months or years after surgery. • Infection may mean removal of your implants. ©2011 MFMER | slide-19 “ Spacesuits worn during surgery” ©2011 MFMER | slide-20 Risks of Surgery Blood loss • Bony surfaces bleed during surgery. • There may be some bleeding after surgery. • Your blood count will be checked each morning after surgery. • If you have symptoms from a low blood count, you may need a blood transfusion. ©2011 MFMER | slide-21 Risks of Surgery Medical Complications • Surgery is a stress to your body. • Heart and lung problems, stroke, stomach problems, constipation - all may occur. • A physical with your regular doctor and an EKG are required before surgery. • Despite precautions, unforeseen medical complications may still occur. ©2011 MFMER | slide-22 Risks of Surgery Dislocation • This is an artificial joint and may slip out of joint. • If it does dislocate, this often requires a trip to the hospital to have the shoulder put back in place. • You may be required to wear a brace if it dislocates. • Multiple dislocations may require revision surgery to fix the problem. ©2011 MFMER | slide-23 Risks of Surgery Need for Revision • We encourage patients to wait as long as possible before replacement. • Implants wear with time.. • Wear rate is about 1% a year • Revision surgery may involve changing the plastic or changing one or all metal parts. • Revision surgery is more challenging with a more difficult recovery. ©2011 MFMER | slide-24 Recovery time • 3-4 months: ‘normal’ activity • 6 months: ‘normal’ endurance • 12 months: maximal recovery • Focus on exercises for movement and then strength • Getting back to work is individual - check with your surgeon ©2011 MFMER | slide-25 Summary • Shoulder replacement is a reliable operation to improve quality of life with less pain, improved motion, strength and better function. • As with any operation, there are associated risks. • All of the precautions we take are to minimize risk and to provide for a “routine” operation ©2011 MFMER | slide-26 Patient Resource and Education Program Joint PREP Class Goals for you and your family • Discuss steps to take to get ready for the surgical procedure • Discuss what to expect of the surgical experience • Recognize why it is important for you to participate in your plan of care ©2011 MFMER | slide-28 Plan Ahead • Appointments: • Your regular doctor for pre-surgery; • Blood work, EKG, Physical exam, discuss • medications • Your surgeon for final discussion and update • Stop smoking – talk to your regular doctor to get help • Call your surgeon if you get a fever, cold, infection or rash before your surgery date ©2011 MFMER | slide-29 Plan Ahead • Plan for your return home • Identify who will take care of you after surgery. Plan for about 2 weeks • Identify who will assist you with shoulder exercises for 6-8 weeks • Practice daily activities not using the arm affected by surgery ©2011 MFMER | slide-30 Plan Ahead • Simplify meals. Plan for 2 weeks of easy or no preparation meals • Pick up throw rugs and other hazards that may cause you to trip • Place frequently used items in convenient locations…not too high or not too low • Any planned dental work should be finished about 1 month before your surgery date ©2011 MFMER | slide-31 What to bring to the hospital • Loose comfortable clothing to wear home • Non skid comfortable shoes • Personal items: toiletries, books, etc. • Medication list, inhalers, C-PAP mask and machine • Cell phones may be used in room ©2011 MFMER | slide-32 What not to bring to the hospital • Valuables/Jewelry • Credit cards, check book, or large sums of money • Your medications (except inhalers) ©2011 MFMER | slide-33 The day before surgery • A Surgical Prep and Recovery nurse will call you to: • Review your medications • Tell you what medications to take and not take the day of surgery • Review eating, drinking, and smoking restrictions • Give hygiene instructions • *You will call a toll free number after 4 p.m. the day prior to your procedure to establish your arrival time. ©2011 MFMER | slide-34 Day of surgery • Take medications at home as instructed • Check in at Mayo Clinic Health System registration desk ©2011 MFMER | slide-35 Day of Surgery • You will be taken to the Surgical Prep and Recovery area • You will be asked your name and date of birth by everyone who has contact with you – this is done for your safety • Family and friends are welcome. Try to limit to 2 people on day of surgery ©2011 MFMER | slide-36 Surgical Prep and Recovery • Nursing admission in the Surgical Prep and Recovery area - We will ask you many questions and get you ready for your surgery • Leg squeezers • Anesthesia visit • Surgeon visit ©2011 MFMER | slide-37 Leg Squeezers – SCDs ©2011 MFMER | slide-38 Going to the Operating Room ©2011 MFMER | slide-39 Operating Room (OR) • Monitors • Anesthesia • Surgical scrub • Staff will communicate to your family if the surgery is longer than 2-3 hours ©2011 MFMER | slide-40 Recovery Room/Post Anesthesia Care Unit (PACU) • Your nausea and pain are managed as you awaken • When you are ready, you will be transferred to a hospital room ©2011 MFMER | slide-41 Arrival in your Hospital Room • You will have… • Oxygen • An IV • Your affected arm will be in a shoulder immobilizer after surgery • A pulse oximeter – a device that fits on your finger to measure blood oxygen level ©2011 MFMER | slide-42 Pulse Oximeter ©2011 MFMER | slide-43 Arrival in your Hospital Room • We will check on you, take your vital signs • You will be able to start drinking and eating when ready • Activity as you tolerate • Help you with control of pain and nausea. ©2011 MFMER | slide-44 Pain Management It is vital for you to describe your pain and where it is located. Rate your pain: The Pain Scale 0—1—2—3—4—5—6—7—8—9—10 NO PAIN MODERATE PAIN WORST POSSIBLE PAIN We must work together to treat your pain-what makes it better/worse? Using medication, deep breathing-relaxation, distraction, position change are some ways to help manage pain and discomfort ©2011 MFMER | slide-45 Pain Management Our goal is NOT to scare you, but PREPARE you for the pain you may have after surgery. ©2011 MFMER | slide-46 After Shoulder Surgery • The nurse will check your bandage on your shoulder • Report any soreness, numbness or tingling in your arm or fingers to the nurse • Ice will be applied to your shoulder to reduce pain and swelling ©2011 MFMER | slide-47 Post operative day You will have…. • Blood work • Medication • For pain control • Aspirin 325 mg for blood thinning to prevent blood clots • Activity – Occupational Therapy to assist with activities of daily living • You are a partner in your care! ©2011 MFMER | slide-48 Discharge Planning You will be discharged home from the hospital when: • Your medical condition is stable • You are able to manage safely at home with assistance • You are able to do your exercises safely • Your pain is under acceptable control ©2011 MFMER | slide-49 Discharge Day • The person who will be taking care of you after you go home needs to come to the hospital to learn about: • Safety • Exercises – Therapy • When and how to use shoulder immobilizer, sling • Lifting restrictions ©2011 MFMER | slide-50 Day of Discharge • Prepare for discharge between 11a.m. and noon to home or transitional care • Receive discharge instructions for: • Incision care/bathing instructions to keep incision clean and dry • Icing and how to keep swelling down • How to take pain medications correctly • Continuing aspirin 325 mg at home for blood thinning for 3 weeks • When to contact your surgeon ©2011 MFMER | slide-51 To control swelling and pain at home • Apply ice to your shoulder after exercises (do not apply heating pad) for 6-8 weeks as directed • Pain medication as directed especially before exercises • Physical therapy/exercises as directed ©2011 MFMER | slide-52 After Discharge • A person to care for you will need to be available 24 hours a day to: • assist you at home the first two weeks • drive you to appointments • encourage you in your home exercise program • Change your incision dressing every day • Wear the immobilizer sling for 6-8 weeks, according to your surgeon’s directions ©2011 MFMER | slide-53 Bathing 1. You may shower when your incision is dry (no drainage) Support your arm as directed by nursing 3. Wash under arm, 2. Place a plastic barrier over the incision, taped in place, prior to showering 4. Place a new dry thoroughly and place dry padding to absorb moisture dressing on the incision after shower ©2011 MFMER | slide-54 Driving No driving. Talk with your surgeon about when you will be allowed to drive again After permission you must : Be off narcotic pain medicines to drive Able to sit in car comfortably Drive in a safe area ©2011 MFMER | slide-55 A Follow-Up Appointment with your surgeon will be made 10-14 days after surgery At your appointment: • X-ray will be done of your shoulder • Your stitches will be removed • We will give you care instructions about your: incision, bathing, exercises, and a handout titled ‘Joint Replacement- Dental Procedures and Antibiotics’ ©2011 MFMER | slide-56 Total Shoulder Replacement Rehabilitation Services: Focusing on Function Purpose • Identify precautions (Do’s and Don’t’s) • Discuss what to expect from therapy • Explain home exercise program ©2011 MFMER | slide-58 After Surgery • You will wear a sling except when performing self-cares and exercises • You can move your elbow, wrist and fingers with your arm at your side • You should not move your shoulder until you have been shown the proper ways to do so (nursing/therapy) ©2011 MFMER | slide-59 After Surgery • You will learn how to move your arm safely when: • Taking care of yourself • Taking sling on/off • Walking/moving about • Exercising ©2011 MFMER | slide-60 Activity After Surgery • No ACTIVE motion of your operative shoulder • Control pain and swelling—ICE OFTEN! • Try to keep the muscles around your shoulder relaxed, “quiet” • Keep moving elbow, wrist and fingers to control swelling ©2011 MFMER | slide-61 Therapy for home • You will learn a home exercise program that includes: • Passive range of motion for your shoulder (no muscle flexing) • Active range of motion for your elbow, wrist and fingers (moving them on your own) • Techniques to control swelling and pain • It is recommended that a person be available at home to assist you ©2011 MFMER | slide-62 Exercises Codmans “Pendulums” Elbow Bend “Fist-Five” ©2011 MFMER | slide-63 At home you will: • Continue with range of motion exercises • Wear immobilizer/sling • Practice your total shoulder precautions • Call your doctors office with questions or concerns ©2011 MFMER | slide-64 You are a Partner in Your Care! • Make your plans… • Start getting ready for surgery! ©2011 MFMER | slide-65 JOINT PREP Social Sevices ©2011 MFMER | slide-66 Roles of Social Services and Case Management in Your Care Work in teams of Social Workers and RN Case Managers to assist with: • Transition Planning • Insurance and Funding Issues • Advance Directives for Healthcare • Counseling and Advocacy ©2011 MFMER | slide-67 Insurance-Prior Notification/Authorization • Prior to surgery, you will need to notify your insurance company of your surgery plans. • Also make sure the clinic/hospital has your correct insurance information for preauthorization purposes. • Prior authorization for surgery can take anywhere from 15-30 days to process, so call your insurer as soon as you know your scheduled surgery date. ©2011 MFMER | slide-68 Insurance-Denial • If for any reason your insurer denies your prior authorization request, the hospital will be notified and we will contact you to let you know your request was denied. ©2011 MFMER | slide-69 Insurance-Notification • Notification of elective surgery is NOT required for those who have only Medicare as their insurer. Medicare rules do not require pre-authorization of elective surgery. • Many Medicare Advantage plans and private insurance companies do require notification of elective surgery by both the surgeon’s office and the patient himself. Although this is not the case for every Medicare Advantage plan and private insurance plan, play it safe by notifying your Medicare Advantage plan or private insurance plan yourself about your surgery plan. ©2011 MFMER | slide-70 Insurance-Contact Once You are Admitted • Once you are an inpatient in the hospital, your RN case manager will monitor your approved stay days and be a contact person for your insurance company for any questions or concerns. ©2011 MFMER | slide-71 Counseling and Advocacy • Surgery and hospitalization are stressful life events. • Meeting your emotional needs is important to all staff at Mayo Clinic Health System. • If you have any concerns about your care or wish to talk to someone, please let your nurse know. ©2011 MFMER | slide-72 Transition Planning-Length of Stay • Length of stay in the hospital is decreasing nation-wide. • Your insurance company will authorize days of stay based on your medical needs. • The usual hospital stay for joint replacement surgery ranges from less than a day to four days depending on your needs. ©2011 MFMER | slide-73 Transition Planning • Once you are in the hospital, a Social Worker or RN Case Manager will meet with you to discuss your transition plan. • You, your support people, doctor, and therapists will help determine what transition plan will best suit your needs. ©2011 MFMER | slide-74 Transitional Care Options • Home with outpatient services • Home with Home Care • Skilled Nursing Facilities • Transitional Care Units or Swing Beds ©2011 MFMER | slide-75 Transitional Care Options-Home with Outpatient Services • Home with outpatient services is an option for the person who is generally in good health, has someone available to stay with them the majority of the time for a few weeks, has progressed sufficiently in therapies during hospitalization, and is self-motivated to perform their exercises at home on a consistent basis. ©2011 MFMER | slide-76 Transitional Care Options-Home Care • Home with Home Care services is an option for the person who has a skilled nursing need such as complex dressing changes or IV antibiotics. Physical Therapy is available through home care agencies but, generally the maximum amount of home therapy they can provide is 2 times a week. In addition to having a skilled nursing or skilled therapy need, home care also requires that you are “homebound,” meaning leaving your home requires a great deal of effort. ©2011 MFMER | slide-77 Transitional Care-Skilled Nursing Facilities • Skilled Nursing Facilities are area nursing homes that offer short-term rehabilitation stays along with their longterm care. This is an option for the person who requires more medical care than family or friends can safely provide. • After shoulder surgery, you may not have any skilled physical therapy or occupational therapy for an extended period after your surgery. As a result, you may not qualify for Medicare or your private insurance to pay for your nursing home stay. • Supportive care like help with bathing, dressing, meal preparation, etc. is not paid for by Medicare. ©2011 MFMER | slide-78 Transitional Care-Swing Beds • Transition Care Units or Swing Beds are located in a rural hospital with care provided by hospital staff and physician. This is an option for the person who has a more skilled nursing care need. Examples would include complex dressing changes or difficult to control blood sugar levels or a pre-existing medical issue such as cardiac disease. Swing Beds can also provide more intensive rehabilitation therapies than the Skilled Nursing Facilities. ©2011 MFMER | slide-79 Insurance and Medicare Coverage for Transitional Care Options • Home with Home Care-Medicare Supplements and private insurance companies vary in what they cover and how much they cover; it’s a good idea to call these insurers to find out the details on what and how much they will cover for each transition care option. ©2011 MFMER | slide-80 Funding Options-Home Care • Medicare will pay for home care services if you are homebound and have a skilled nursing or skilled therapy need. Medicare will not pay for home care services such as help with meals, shopping, personal care, or housekeeping services. ©2011 MFMER | slide-81 Funding Options-Transitional Care Skilled Nursing • Skilled Nursing Facilities-Medicare requires a skilled nursing and/or therapy need plus a three overnight inpatient status stay in the hospital to cover a skilled rehabilitation stay in a nursing facility. • Some Medicare Advantage plans do not require the three overnight stay. • Private insurance coverage varies tremendously. It is important to check your benefits and which facilities are available to you under your plan. ©2011 MFMER | slide-82 Funding Options-Swing Bed • Swing Bed-Medicare requires a skilled nursing and/or therapy need plus a three overnight inpatient status stay in the hospital to cover a skilled rehabilitation stay in a swing bed. • Not all Medicare Advantage Plans will cover swing bed stays. Check your insurance plan to find out if swing bed is an option for you. • Private insurance coverage for swing bed stays varies greatly. Check with your insurance company regarding this. ©2011 MFMER | slide-83 Advance Directives for Healthcare • What are advance directives? • What are the 2 types of advanced directives? ©2011 MFMER | slide-84 Declaration to Physicians or Living Wills • Describes the kind of life-sustaining care you would want only if you had a terminal condition or were in a persistent vegetative state • Living wills direct your physician regarding lifesustaining treatment and use and withdrawal of feeding tubes • Living wills do not give authority to anyone to make health care decisions on your behalf ©2011 MFMER | slide-85 Power of Attorney for Health Care • Your health care agent can tell your physician what kind of care you would want in all types of health decisions, not just concerning life-sustaining treatment • You appoint an agent to make all health care decisions for you in collaboration with your physician • Guardianship can usually be avoided if a health care power of attorney has been completed. ©2011 MFMER | slide-86 Who Can Help you Complete an Advance Directive? • Mayo Clinic Health System Social Services • Mayo Clinic Health System Spiritual Care Chaplains • Your personal attorney ©2011 MFMER | slide-87 Safekeeping of Advance Directives • Store the original document in a safe place. • Give a copy of the document to family members, especially those named in the document. • Bring a copy of the document to the clinic or hospital. It will be scanned into your medical record. ©2011 MFMER | slide-88 QUESTIONS? • THANK YOU!! ©2011 MFMER | slide-89