Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
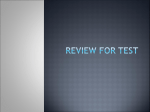
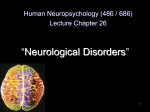
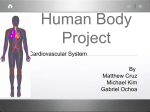
CASE OF THE MONTH SHRAWAN DR MERINA SHRESTHA RESIDENT 3RD YEAR IOM PATIENT’S PROFILE • NAME: SHARMILA MAJHI • AGE : 6 YEARS/F • ADDRESS: MAKAWANPUR • DATE OF ADMISSION: 062/4/12 • DATE OF DISCHARGE: 062/4/32 • ADMITTING DX: ACUTE STROKE SYNDROME • FINAL DX MOYA MOYA DISEASE HISTORY OF PRESENT ILLNESS • Sudden onset of weakness of left side of the body and deviation of face towards right for 1 day. • Mild headache for 4 days. • The weakness was non-progressive. • No H/O drooling or difficulty in swallowing or speech difficulty • No H/O fever, vomiting,ear discharge, sore-throat. • No H/O altered sensorium, visual disturbance, loss of consciousness or abnormal movements of the body. HISTORY OF PRESENT ILLNESS contd……… • No H/O SOB, palpitation. • No H/O bleeding from any site, rash, bone or joint pain or swelling in any part of the body • No H/O high colored and decreased urine output. • No H/O trauma or any pencil injury. • No H/O intake of any medicine. HISTORY OF PAST ILLNESS • Similar episode of sudden onset of weakness 5 months back _ Right side of the body. • Was admitted at KCH for 2 days and discharged and was referred to Nutritional rehabilitation center. • Resolved spontaneously in period of a month and was doing well since then. FAMILY HISTORY • Father : 25years/ painlter • Mother: 23years/ House-wife • Siblings: Elder : 10 years/F Younger: 3years/F • No H/ O similar illness/ TB in the family or in close contacts. • No H/O consanguinity of marriage. • BIRTH HISTORY—FT/S/F/NVD at Home ante-natal/intra-partum or postpartum period: Uneventful • IMMUNIZATION HISTORY: Completed according to EPI schedule. • DEVELOPMEENTAL HISTORY:Normal for her age • NUTRITIONAL HISTORY: Taking less than required calorie (70kc/kg/d). ON EXAMINATION: • Child looks comfortable and Alert. • Vitals: Pulse: 90/min R/R : 24/min B.P : 90/40 mm Hg Temp: 98.60C • No pallor, icterus, rash, lymphadenopathy,edema, Phakomas or any joint swelling or bony tenderness • ENT Examn: Normal • Anthropometry: HT : 101cms (93%) WT : 13kgs (72%) GRADE II PEM WT/HT : 86% CNS EXAMINATION: • • • • • • Conscious, cooperative and alert Oriented to time , place and person. Memory: Intact. Speech: Normal No signs of meningeal irritation CRANIAL NERVES: Pupils: B/L equal and reacting to light Fundus:Normal Left sided facial palsy ( UMN Type) MOTOR SYSTEM EXAM… upper limbs lower limbs BULK Right N Left N Right N Left N TONE N Less N Less POWER 5/5 2/5 5/5 3/5 DTJ N slight Increased N slight Increased Plantar RT: Withdrawl Lf: Withdrawl • SUPERFICIAL REFLEX: Normal • SENSOTY SYSTEM : Normal • COORDINATION : Intact • GAIT : Dragging of left foot • CARDIOVASCULAR SYSTEM; S1, S2 : Normal No added sounds • RESPIRATORY SYSTEM: B/L equal air entry with VBS • P/A : soft, no visceromegaly, BS- N PROV. DX: ACUTE STROKE SYNDROME • INVESTIGATIONS: • CBC: Hb : 12 gm% Platelet : 120,000/cmm TC : 5000/cmm P- 58%, L- 40% ESR : 20 mm/ 1st hour PBF : Normocytic Normochromic • Mantoux test : Negative CT SACN HEAD • MULTIPLE INFARCTS IN B/L CEREBRAL HEMISPHERE • S/O MOYA MOYA DISEASE CEREBRAL ANGIOGRAPHY Poorly opacified intracranial internal carotid artery and its branches • Stroke is defined as the abrupt or ictal onset of focal or global neurologic symptoms caused by ischemia or hemorrhage within or around the brain resulting from diseases of the cerebral blood vessels. • Annual incidence of cerebral infarction in children, all over the world, varies between 1.2 per 100,000 to 2.7 per 100,000. • less than 1% of all pediatric admissions and 510% of all stroke in young (<40 years) • The two primary pathophysiologic features of cerebrovascular disease are interruption of blood flow to part of the brain or rupture of blood vessels with bleeding into the cerebral parenchyma. Occlusive vascular disease is slightly more common (55%) than intracranial hemorrhage (45%) Ischemic causes: • Heart Diseases Congential heart disease Rheumatic heart disease Infective endocarditis Complication of surgery • Hematologic Disorders Thrombocytosis Polycythemia Leukemia Antithrombin 3, Protein C and Protein S deficiency • Infective Vasculitis Pyogenic Tuberculous Fungal AIDS • Non Infective Vasculitis SLE Polyarteritis nodosa Takayasu arteritis • Non specific Moya Moya Syndrome Trauma Blunt cervical arterial trauma Ischemic causes contd…. • Oral foreign bodies injuring the carotid artery • Hereditary Metabolic Homocystinuria Mitochondrial myopathy, encephalopathy, lactic acidosis and stroke like episodes (MELAS) • Toxic Phencyclidine Methamhateminne Phenylpropanolamine Cocaine Hemorrhagic Stroke Vascular Malformations Arteriovenous malformation Aneurysm Angiomas • Hematological Leukemia Thrombocytopenia Hemophilia • Disseminated intravascular coagulation • Trauma • Shaken baby syndrome • Prematurity Subependymal hemorrhage STANDARD EVALUATIONS: • Complete blood count , platelet and coagulation profile • LFT • Electrolytes, BUN, and creatinine, Glucose • Total protein, Uric acid • Calcium, phosphate • Cholesterol, triglycerides • Electrocardiogram • Carotid duplex studies Optional tests • Lumbar puncture • Imaging studies Magnetic resonance angiography CT angiography • Tc-99m HMPO SPECT • Collagen vascular screen Rheumatoid factor Antinuclear antibody Lupus anticoagulant • Protein C and protein S • Antithrombin 3 • Other VDRL/HIV Blood cultures Urinalysis Lactate/pyruvate levels MOYA MOYA DISEASE • First described in Japan in the 1960s by Takeuchi. The term refers to something hazy, “ just like a puff of cigarette smoke drifting in the air”. • The disease has since been found in the United States, Europe, Australia, and Africa . • Sex: The female-to-male ratio is 1.8:1. • Age: 6 months to 67 years, with the highest peak in the first decade. Definition: • It is a rare, progressive cerebrovascular disorder characterized by the narrowing or occlusion of major blood vessels leading into the brain, and the formation of abnormal blood vessels called moyamoya vessels. (ie "puff of smoke") characterizes the appearance on angiography of abnormal vascular collateral networks that develop adjacent to the stenotic vessels. The stenoocclusive areas are usually bilateral, but unilateral involvement does not exclude the diagnosis. PATHOLOGY: • Intimal thickening in the walls of the terminal portions of the internal carotid vessels bilaterally which contain lipid deposits. • The anterior, middle, and posterior cerebral arteries that emerge from the circle of Willis may show varying degrees of stenosis or occlusion with fibrocellular thickening of the intima, waving of the internal elastic lamina, and thinning of the media. • Numerous small vascular channels can be seen around the circle of Willis. These are perforators and anastomotic branches. The pia mater also may have reticular conglomerates of small vessels. Causes of MOYA MOYA D/S: • Primary: strong hereditary predisposition among Japanese pop. gene is mapped on short arm of Ch 3. • Secondary(Moya Moya Syndromea) Infections: Tuberculosis Leptospirosis Hematologic disorders – Aplastic anemia, Fanconi anemia, sickle cell anemia, Congenital syndromes Apert syndrome Down syndrome Marfan syndrome, tuberous sclerosis, Turner syndrome, von Recklinghausen disease, Hirschsprung disease • In a case series of patients at Hospital of Sick Children, Toronto , the most common association was seen with Neurofibromatosis accounting for 54%. Moya Moya has been reported with Down,s syndrome as well. Bhalala Utpal S, Parekh Pankaj R Moyamoya syndrome in a child with down syndrome Indian Journal of PediatricsYear : 2005 | Volume : 72 | Issue : 7 | Page : 635-637 • Vascular dysplasia may lead to a structural defect which forms the basis for Moyamoya disease. It is believed that several proteins encoded on chromosome 21 are associated with an increased risk of vascular disease. • Another mechanism increased prevalence of autoimmune disorders • Upper cervical subluxation can also produce a cerebral circulatory insufficiency that predisposes to development of Moyamoya disease CASE STUDY • A 9-year-old girl, the first born of seconddegree consanguineous parents, presented with a sudden onset of inability to move the left upper limb and a limp while walking. The onset was preceded by an episode of giddiness and blurring of vision, which lasted for 2-3 hours. The weakness evolved over a period of 12 hours and when she was brought to the hospital, she had dense left hemiplegia and left sided upper motor neuron facial palsy. • Clinical course was marked by rapid improvement, and her muscle power improved to 4/5 (MRC grading) by the fourteenth day of hospital stay. Examination of the skin revealed large hypopigmented and hyperpigmented areas all over the body. Active skin lesions were suggestive of atopic eczema. The lesions did not follow any photosensitive pattern of distribution. Nail dystrophy was present, hair was sparse and seborrheic dermatitis of scalp was present. • CBC, ESR , RFT and LFT and Coagulation profile were normal. • ANA -negative. • Screening tests for homocystinuria and porphyria were negative. • Serology for leptospira was negative. • Chest x-ray was normal and Mantoux test was negative. • Moya moya collateral in cerebral angiogram • Magnetic resonance angiogram revealed partially filled up circle of Willis on the left side and occlusion of the circle of Willis on the right side with extensive collaterals Four types have been described: • Hemorrhagic type with subarachnoid bleeding • Epileptic type with repeated seizures • Infarct type with permanent paresis • Transient Ischemic attack characterized by recurrence. (most common) Clinical features: • Children may have hemiparesis, monoparesis, sensory impairment, involuntary movements, headaches, dizziness, or seizures. Mental retardation or persistent neurologic deficits may be present. • Chorea may be the only presenting feature.(Indian Pediatrics 2000;37: 1005-1009 DIAGNOSIS • CT / MRI head to be done as the early diagnostic modality. • Cerebral angiography is the criterion standard for diagnosis. The following findings support the diagnosis: -Stenosis or occlusion at the terminal portion of the internal carotid artery or the proximal portion of the anterior or middle cerebral arteries -Abnormal vascular networks in the vicinity of the occlusive or stenotic areas -Bilaterality of the described findings. TREATMENT • Pharmacologic therapy for MMD is disappointing. Therapy is directed primarily at complications of the disease • If intracerebral hemorrhage has occurred, then management of hypertension (if present) • In cases of severe stroke, intensive care unit (ICU) monitoring is indicated until the patient's condition stabilizes. • If the patient has had an ischemic stroke, consider anticoagulation or antiplatelet TREATMENT contd….. • The rationale behind anticoagulation and antiplatelet agents is to prevent further strokes, especially in stenotic vessels where further infarction can occur if occlusion progresses. These medications are not approved by the Food and Drug Administration (FDA) specifically for use in MMD, so the decision to treat with anticoagulants, ie, heparin (and in some cases, warfarin for long-term anticoagulation), or antiplatelet agents (eg, aspirin) rests on the following: angiogram findings, severity of stroke, and risk/benefit analysis by physicians who are experienced in stroke treatment. SURGICAL MANAGEMENT • Patients who present for treatment while symptoms are evolving have a better prognosis than those who present with static symptoms (which probably indicate a completed stroke). Various surgical procedures have been used: • superficial temporal artery–middle cerebral artery (STAMCA) anastomosis, encephaloduroarteriosynangiosis (EDAS), • encephaloduroarteriomyosynangiosis (EDAMS), • omental transplantation. • All of these operations have in common the concept of a blood and oxygen “starved” brain reaching out to grasp and develop new and more efficient means of bringing blood to the brain and bypassing the areas of blockage . PROGNOSIS • Kim S K et al:Moyamoya disease among young patients: its aggressive clinical course and the role of active surgical treatment .Neurosurgery. 2004 Apr;54(4):840-4; discussion 844-6. • A total of 204 patients with MMD who underwent encephaloduroarteriosynangiosis, were categorized into three groups according to their ages at the time of surgery, i.e., Group A (n = 23, <3 yr of age), Group B (n = 50, 3-6 yr of age), and Group C (n = 131, >6 yr of age). For each group, patterns of presentation and the occurrence of subsequent preoperative or surgery-related infarctions were assessed. Clinical outcomes and postoperative hemodynamic status were analyzed. • RESULTS: • At initial presentation, infarctions were significantly more frequent in Group A (87%) and Group B (58%) than in Group C (46%). Subsequent preoperative infarctions occurred significantly more frequently in Group A (39%) than in Group B (6%) or Group C (0.8%). The median interval between the onset of symptoms and a subsequent preoperative infarction was 3 months (range, 1-14 mo). No significant difference in the rates of surgery-related infarctions among the three groups was observed. The rate of favorable clinical outcomes was significantly lower in Group A (58%) than in Group B (84%) or Group C (86%), although the rates of postoperative hemodynamic improvements were similar among the groups. The poor clinical outcomes for Group A were caused mainly by preoperative infarctions. • CONCLUSION: Young-age MMD demonstrates rapid disease progression and results in poor clinical outcomes. These findings indicate the necessity of early surgery for young patients with MMD; however, the actual benefits should be verified with additional controlled studies, with long-term follow-up monitoring. • Stroke. 1984 Sep-Oct;15(5):873-7. • Intelligence in children with moyamoya disease: evaluation after surgical treatments with special reference to changes in cerebral blood flow.Ishii R et al. • The effect of surgical treatment upon the intelligence of 20 children with moyamoya disease was evaluated and related to changes in cerebral blood flow (CBF). The patients were treated by various surgical revascularization procedures • The degree of reduction in the intelligence quotient (IQ) correlated well with the age of the patients; the older patients revealed a more marked reduction of IQ, and the patients with lower intelligence scores in general showed a tendency for more marked depression of mean CBF. Postoperatively, most of the patients showed increase in IQ, especially in performance IQ which improved significantly in 10 patients, remained unchanged in 3 and deteriorated in 2. Mean CBF increased by an average of 11.4%, and postoperative changes in mean CBF correlated well with the changes in IQ in most patients. This may show that the postoperative increase in CBF is quite possibly responsible for the THANK YOU