Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
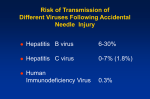
Occupational Exposures to Bloodborne Pathogens Arjun Srinivasan Johns Hopkins Hospital Outline • What’s an exposure? • 1st step in all exposures - Clean the site!! • Specific pathogens – Hepatitis C – Hepatitis B – HIV Scope of the Problem • Difficult to asses: up to 70% of exposures go unreported (Marcus, R. et. al. Ann Emerg Med 1995;25:776) • 1990 estimate: 500,000 exposures/year (Henry, K. Minnesota Medicine 1995;78:41-44) • Costs are also tough to asses but JHH spent $282,000 on post-exposure evaluation and treatment in 1998 Scope of the Problem Impossible to measure the psychological stress that an exposure places on a health care worker At Risk Exposures 1. Percutaneous injury Hollow needle > Solid sharp Visible blood Deep injury Device in patient’s artery or vein 2.Splash on non-intact skin 3.Splash on mucous membrane Risks From Body Fluids • Known to be infectious: – Blood – Any fluid visibly contaminated with blood – Semen – Vaginal secretions – Concentrated virus (used in labs) Risks From Body Fluids • Potentially infectious – CSF – Pleural fluid – Pericardial fluid – Peritoneal fluid – Amniotic fluid – Synovial fluid – Tissue samples Risks From Body Fluids • Not Infectious (if not visibly bloody) – Tears – Saliva – Urine – Feces – Sweat – Emesis The Solution to Pollution . . . • Exposure site should be cleaned IMMEDIATELY! This may be the most important part of PEP • Skin wounds should be washed with soap and water • No evidence that antiseptics are useful and caustic agents (bleach) may do more harm than good The Solution to Pollution (cont) • Mucous membranes should be flushed thoroughly with water • Eyes should be irrigated with a liter of saline A word from our lawyers . . . • ALL exposures should be reported to the proper people (Occupational health, Employee health etc.) • Disability claims can be denied if follow up reporting was not done right Hepatitis C Hepatitis C: Risk of Exposure • Risk of seroconversion following needlesticks involving Hep C positive patients is 0-7% (avg 1.8%) (Kiyosawa, K. et.al. Ann Int Med 1991;115:367) (Lanphear, B.P. et.al. Inf Ctrl Hosp Epi 1994;15:745) • Transmission via mucous membrane exposure described in one case (Sartori, M. Jnl Inf Dis 1993;25:270) Hepatitis C: Risk of Disease Hep C serconversion 15% Clear Spontaneously 85% Chronically Infected 80% Chronic Stable 20% Chronic Progressive (Cirrhosis) Risk of cirrhosis from needlestick= (.0-.07)(.85)(.2)= .0-1% Post Exposure Recommendations • Clean the site immediately • Hepatitis B immune globulin has NOT been effective • Interferon is NOT recommended at this time (Infect Control Hosp Epi 1994;15:742-4) (MMWR 2001;50(RR-11):1-67) Hepatitis C: Follow Up • Enzyme linked immunoassay (EIA) is screening test of choice • ALL exposed HCWs should have LFTs monitored • Average interval between exposure and seroconversion with EIA is 8-10 weeks • Follow up guidelines vary - CDC recommends follow up at 4-6 months Hepatitis C: Follow up issues • EIA is falsely positive in up to 50% of HCW and falsely negative in 5% - results must be confirmed by RIBA or VL • PCR may catch infection earlier but detection is highly variable • Immediate referral for treatment if HCW seroconverts Hepatitis C: Counseling • Risk of transmission to infants and partners is thought to be low • Exposed HCW do not need to modify sexual practices, stop breast feeding or refrain from becoming pregnant • Should not donate blood MMWR 2001;50(RR-11):23 Hepatitis B Hepatitis B: Risk of Exposure • Most infectious bloodborne pathogen • Risk of clinical hepatitis up to 30% in percutaneous exposures to patients who are “e” antigen positive (Werner, B.J. et.al. Ann Int Med 1982;97:367) • Risk from mucous membrane exposure less well defined but also felt to be high Hepatits B: Outcome of Infection • In patients who are infected with Hep B: – – – – 25% get jaundice 5% require hospitilization 6-10% become chronically infected .125% die of fulminant hepatitis Hepatitis B: Good News • Most HCWs have been vaccinated and vaccine offers virtually complete protection to responders Hepatitis B: Bad News • Some employees are NOT vaccinated • 6-10% of vaccinees do NOT develop antibody • Really bad news: CDC estimates that 50-75 HCW die from Hep B each year Hepatitis B: Post Exposure • Clean the site immediately • Determine the vaccine status of the HCW • Determine the surface antigen status of the source patient Hep B: HCW Never Vaccinated • HCW should receive vaccine ASAP 1. Source patient is sAg positive: HCW should also receive one dose of Hep B immune globulin (HBIG) .06ml/kg (1 vial=5 ml) ASAP and absolutely within 7 days of exposure 2. Source patient sAg neg or unknown Vaccine alone Hep B: HCW Vaccinated (one or more doses) • Source patient should be tested for sAg AND HCW should be tested for sAb • If HCW has adequate Ab >10 IU/mL (now or at any time) then no additional treatment Hep B: HCW Vaccinated • IF HCW has inadequate Ab: 1. If pt is sAg negative: HCW should get booster dose of vaccine (or complete series) 2. If pt is sAg positive: HCW should receive HBIG AND a booster dose of vaccine at different sites (complete series if necessary) Hep B: HCW Vaccinated (cont.) If HCW has inadequate Ab: 3. Unknown source: Give vaccine booster or complete series Vaccine non-responders • If HCW has inadequate Ab after 3 dose series they should get another series: 3050% chance of responding to 2nd series • If no response to 2nd series HCW should be considered susceptible • PEP for known non-responders exposed to Hep B positive or high risk unknown sources: 2 doses of HBIG- 1 at exposure then 4 weeks later Hep B: Follow Up Testing • Hepatitis B sAg is the test of choice as it rises in about 6 weeks • LFTs should be monitored at regular intervals Post Exposure Counseling • Risk of transmission to infants and partners is thought to be low • Exposed HCW do not need to modify sexual practices, stop breast feeding or refrain from becoming pregnant • Should not donate blood MMWR 2001;50(RR-11):23 HIV HIV: Risk of Exposure • Risk of transmission from percutaneous expsosures involving HIV positive pts estimated at 0.3% • Risk from mucous membrane exposure estimated at 0.1% • As of 2000 there were 56 confirmed and 138 possible cases of occupational transmission in the US Rationale for PEP • HIV infects dendritic cells and then regional lymph nodes before becoming systemic • AZT blocks infectivity of HIV infected dendritic cells • Goal of PEP is to halt viral replication before systemic infection is established Does It Work? • Several animal studies showing efficacy • Peri-natal prophylaxis has been effective • Retrospective study showed that risk of seroconversion after exposure was 81% lower in HCWs who took AZT PEP. (NEJM 1997;337:1485) Time is Virus • Animal studies show that PEP should be given within 2-8 hours of exposure for maximal effect (JID 1991;163:625 - Within 2 hrs optimal) (JID 1993;168:825 - Within 8 hrs optimal) • PEP may have some benefit up to 36 hrs but seems to be ineffective if given later What To Use? • Before: AZT+3TC +/- IDV or NFV • Now: Becoming more difficult to answer! • Regimens may need to be tailored based on the treatment history of the source patient Surveillance study from 1998-1999 found that 39% of virus from source patients had some NRTI resistance and 10% had some PI resistance. Nucleoside Reverse Transcriptase Inhibitors (NRTI) • Still form the backbone of most regimens • AZT has been formally studied thus it should be included if possible • Addition of 3TC is recommended because: 1. It appears non-toxic 2. It has some synergistic effect with AZT with respect to mutations NRTI (cont) • If source patient’s virus is felt to be resistant to AZT or 3TC alternatives include: • d4T + 3TC • d4T + ddI • Role of abacavir? • Role of tenofovir? Protease Inhibitors (PI) • Are very potent anti-virals and work very well in patients • BUT they have significant side effects and can cause HCW to stop PEP altogether • PI should be recommended primarily when the exposure is high risk • Any PI can be used but indinavir and nelfinavir have been used the most Non Nucleoside Reverse Transcriptase Inhibitors (NNRTI) • Not much experience using these for PEP • Use should be reserved for situations when source patient’s virus is thought to be resistant to all PIs • Nevirapine should probably be avoided as PEP: from 1997-2000 there were 22 reports of serious toxicity in HCW taking it for PEP Toxicity of PEP • 50-90% of HCWs report some side effects from PEP • 24-36% of HCWs stop PEP because of side effects • PEP only works when taken - More may not be better! Side Effects of PEP • All side effects have been described in some degree in HCWs on PEP • Serious side effects appear rare: isolated reports of hepatitis and pancytopenia • Excluding problems with nevirapine, all side effects have reversed with stopping meds (MMWR May 15, 1998/ 47(RR-7);1 PEP Counseling • Clean the site immediately • Determine the HIV status of the source • Determine the extent of the exposure PEP management: Source Patient Testing • Crucial 1st step as most exposures do NOT involve HIV positive patients • Rapid test kit (SUDS) is available and yields an answer in about 30 minutes • Rapid test is an EIA that is >99.9% sensitive • Testing of blood on sharps is NOT recommended • Patient consent is required in Maryland HIV RNA Testing of Source • No official recommendations and test is not approved for this indication • Should be reserved for cases where there is a suspicion of acute retroviral conversion Source Patient 1. Patient HIV negative - No PEP 2. Patient HIV positive Low viral load / high CD4 = class 1 High viral load / low CD4 = class 2 3. Patient HIV positive, unknown CD4, VL Use best judgement - err towards class 2 4. Unknown source Exposure Types 1. Non-infectious fluids - No PEP 2. Mucous membrane, non-intact skin Small volume Large volume 3. Percutaneous injury Less severe More severe HIV PEP Recommendations Percutaneous injuries Less severe • Source pt HIV negative - No PEP • Source pt class 1 - Recommend 2 drugs • Source pt class 2 - Recommend 3 drugs • Source of unknown status- Consider 2 drugs in setting where exposure to HIV positive pt likely or if pt has HIV risk factors HIV PEP Percutaneous Injuries (cont.) More severe injury • Source pt HIV negative - No PEP • Source pt HIV class 1 or 2 - Recommend expanded 3-drug regimen • Source of unknown status - Consider 2 drugs in setting where exposure to HIV positive pt likely or if pt has HIV risk factors HIV PEP Mucous membrane exposures Small Volume • Source pt HIV negative - No PEP • Source pt class 1 - Consider 2 drugs • Source pt class 2 - Recommend 2 drugs • Source of unknown status- Consider 2 drugs in setting where exposure to HIV positive pt likely or if pt has HIV risk factors HIV PEP Mucous membrane exposures Large volume • Source pt HIV negative - No PEP • Source pt class 1 - Recommend 2 drugs • Source pt class 2 - Recommend 3 drugs • Source of unknown status- Consider 2 drugs in setting where exposure to HIV positive pt likely or if pt has HIV risk factors Duration of Treatment • Current recommendation is 4 weeks but this is an arbitrary selection • Animal studies suggest 10 days is too short but 28 days conferred protection Resistance • Becoming a significant problem now that so many patients are getting treated • Treatment history can be helpful in the acute setting • Recent history may be more important than remote Resistance Issues • Full medical history often not available when the exposure occurs - PEP should NOT be delayed • Data from maternal transmission studies shows viral resistance does not preclude benefit Resistance Issues • Consultation with someone experienced in HIV treatment is recommended in cases where HIV resistance is possible • PEP may need to be modified once more history is available • Resistance testing is too slow to be of use right now PEP and Pregnancy • Women of child bearing age should be offered a pregnancy test before starting PEP • BUT, recommendations on starting PEP should NOT change just because HCW is pregnant HIV medications to avoid in Pregnant HCW • d4T, ddI: have been associated with severe lactic acidosis in pregnant women • Efavirenz: is teratogenic in primates • Indinavir: causes hyperbilirubinemia in newborns if given near time of delivery Post Exposure Testing • Testing should be done at regular intervals (eg 6,12 weeks and 6 months) • Testing should continue for 12 months if the HCW contracts HCV from the exposure • Unclear if testing should be prolonged in exposures to pts with HIV and HCV or in HCW who have history of impaired Ab responses Post Exposure Testing • EIA is test of choice • Viral loads and p24 assays should be reserved for suspected cases of acute seroconversion given high false pos rate Counseling • For 3 months following exposure HCW should avoid: -unprotected sex -donating blood -sharing razors, toothbrushes • HCW should consider stopping breast feeding (risk of perinatal transmission and drugs may get into breast milk) Time to Seroconversion • Most HCW seroconvert in 6-12 weeks with median time of 46 days • 95% seroconvert within 6 months • 100% seroconvert in one year • Co-infection with HCV may delay HIV seroconversion Acute Retroviral Conversion • Symptomatic seroconversion develops in 50-90% of cases • Average time from exposure to symptoms is 2-6 weeks • ANY HCW who develops a flu-like illness in the follow up period should be encouraged to get HIV RNA testing Resources • US Public Health Service Guidelines www.cdc.gov/ncidod/hip • National PEP Hotline (run by UCSF) 1-888-448-4911 (24 hrs) www.ucsf.edu/hivcntr Conclusion • People react very differently to exposures be prepared for anything! • The psychological impact of an exposure can be enormous • Your patience and understanding may be the best PEP of all