Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
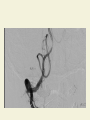
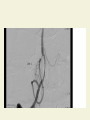
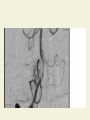
CVA SAMIR TURK, M.D. SYMPTOMS OF STROKES AND TIA • • • • • • PARALYSIS NUMBNESS LANGUAGE VISUAL ATAXIA VERTIGO CLINICAL PRESENTATION • CORRELATES WITH OCCLUDED ARTERY • KNOWLEDGE OF BLOOD SUPPLY ALLOWS LOCALIZATION • RADIOLOGICAL TESTING CONFIRMS LOCALIZATION MOTOR/SENSORY RULE • BRAIN MEDIATES OPPOSITE SIDEMOTOR/SENSORY • BRAIN STEM – SAME SIDE OF FACE MOTOR/SENSATION • CEREBELLUM –SAME SIDE FINE MOTOR BLOOD SUPPLY • 2 MAJOR TERRITORIES : 1- ANTERIOR CIRCULATION – ICA/MCA/ACA 2-POSTERIOR CIRCULATION – VERTEBRALS/BASILAR/POSTERIORCEREBRAL MCA OCCLUSION LEFT DOMINANT - 90% LANGUAGE – RIGHT FACE AND ARM MOTOR AND SENSORY RIGHT SIDE NEGLECT EYES DEVIATE TO LEFT LEFT ACA • RIGHT LEG-- MOTOR AND SENSORY • BEHAVIOR : ANGER/HOSTILITY RIGHT MCA • • • • APROXIA LEFT SIDED FACE/ARM MOTOR AND SENSORY LEFT SIDED NEGLECT AND VISION LOSS EYES DEVIATE TO RIGHT RIGHT ACA • LEFT LEG MOTOR AND SENSORY • BEHAVIOUR : ANXIETY AND DEPRESSION ICA OCCLUSON • BOTH ACA AND MCA OCCLUSION • MONONUCLEAR BLINDNESS –OPTHALMIC ARTERY OCCLUSION • PARTIAL HORNER SYNDROME : PTOSIS/MIOSIS BUT ANHYDROSIS IS ABSENT POSTERIOR CIRCULATION • • • • • • REMEMBER THE 5 D’s 1-dizziness 2-diplopia 3-dysarthria 4-dysphagia 5-dystaxia POSTERIOR CIRCULATION • CROSSED FINDINGS : CRANIAL NERVES DEFICIT- IPSILATERAL MOTOR/SENSORY DEFICIT- CONTRALATERAL VERTEBRAL OCCLUSION • PRODUCES OCCLUSION IN PICA • LEADS TO LATERAL MEDULLARY SYNDROME LATERAL MEDULLARY SYNDROME • 1- SPINOTHALAMIC TRACT- CONTRALATERAL DECREASE IN TEMP AND PAIN • 2- 5TH CRANIAL NERVE PALSY –IPSILAT EYE PAIN,NUMB FACE AND DECREASE CORNEAL REFLEX • 3- VESTIBULAR NUCLEUS – DIZZINESS/VOMITTING AND NYSTAGMUS • 4- INFERIOR CERBELLAR PEDUNCLE –IPSILAT.ATAXIA • 5- IPSILATERAL HORNER- LABILE BP AND TACHY • 6- HOARSNESS AND DYSPHAGIA • 7-ABNORMAL RESPIRATION STROKE MIMICKS • • • • • • • HYPOGLYEMIA MASS LESIONS SEIZURES MIGRAINE ENCEPHALOPATHIES CONVERSION DISORDERS PERIPHERAL VESTIBULOPATHIES CHAMLEONS • • • • • CONFUSION STATES VIT DEF MS MOVEMENT DISORDERS TRANSIENT GLOBAL AMNESIA TREATMENT • • • • TRADITIONAL : SUPPORTIVE THROMBOLYSIS : IV THROMBOLYSIS : INTRAARTERIAL IN SITU RETRIEVAL DEVICES TREATMENT • IV THROMBOLYSIS. • TPA FOR TREATMENT OF CVA APPROVED IN 1996 • NINDS TRIAL IV THROMBOLYSIS • 31% OF THOSE WHO RECEIVED TPA HAD EXCELLENT OUTCOME • 20% OF THOSE WHO DID NOT RECEIVE IV TPA HAD EXCELLENT RECOVERY • 11% ABSPLUTE IMPROVEMENT IV THROMBOLYSIS TPA HEMORRHAGE 6.4% DEATH 11% NO TPA HEMORRHAGE <1% DEATH 20% INDICATION FOR IV TPA • • • • • AGE >18 DEFINED TIME OF ONSET WITHIN <3 HOURS MEASURABLE NIHSS NO CONTRAINDICATION CONTRAINDICATION FOR IV THROMBOLYSIS • • • • • • • MINOR SYMPTOMS OR IMPROVING SEIZURE AT ONSET STROKE OR HEAD TRAUMA < 3 MONTHS ANY HX OF ICH GI/GU HEMORRAGE < 3 WEEKS MAJOR SURGERY < 3 WEEKS NONCOMPRESSIBLE ARTERIAL PUNCTURE<7 DAYS CONTRAINDICATION OF IV THROMBOLYSIS • RECEIVED HEPARIN WITHIN 48 HRS AND PTT IS ABNORMAL • BP > 185/100 • INR >1.7 • PLTS <100K • GLUCOSE <50 OR >400 IV TPA 3-4.5 HOURS • SOME BENEFIT IN SELECTED PATIENTS • NOT FDA APPROVED • ADDITIONAL EXCLUSION CRITERIA : AGE>80 ON ORAL ANTICOAGULATION REGARDLESS OF INR NIH SCORE >25 HX OF STROKE AND DM OTHER CONSIDERATIONS • IF THERE IS CONTRAINDICATION TO IV LYSIS THEN CONSIDER : 1- INTRAARTERIAL LYSIS – LESS TPA 2- MECHANICAL RETRIEVAL DEVICES PENUMBRA SYSTEM OR MERCI DEVICE SHOULD CONSIDER FOR ALL CASES OF NIHSS OF >10 AS THE CHANCE OF OPENING AN MCA OCCLUSION WITH IV LYSIS IS ONLY 15% LIMITATIONS OF IV TPA • ONLY 4% OF CVA PTS RECEIVE TPA • 22% PRESENT WITHIN 3 HRS • 51% OF THOSE PRESENTING WITHIN 2 HRS ARE INELIGIBLE • POOR RECANALISATION RATES- M1 SEGMENT ONLY 13% INTRAARTERIAL THROMBOLYSIS • SAME AS IV THROMBOLYSIS – THE RISK OF BLEEDING IS HIGHEST WITH LAERGER STROKES • RISK OF DISSECTION,PERFORATION AND DISTAL EMBOLISATION • TECHNICALLY VERY DEMANDING AND CHALLENGING • CEREBRAL VESSELS ARE VERY TORTUROUS INTAARTERIAL THROMBOLYSIS • ONLY FEW MG OF TPA IS NEEDED • MAY NEED AN HOUR OR MORE TO LYSE THE CLOT • BEST TO DO WITHOUT INTUBATIONS IF POSSIBLE • LARGER VESSELS MAY BE IMPOSSIBLE TO OPEN WITH LYSIS ALONE MEDICAL TREATMENT • IS AS IMPORTANT AS LYSIS • BP MEDICATIONS SHOULD BE WITHHELD UNLESS SBP >220 OR DBP>120 • TREAT HYPOTENSION WITH SALINE AND PRESSORS IF NEEDED • TREAT CARDIAC ARRYTHMIAS MEDICAL TX • TREAT HIGH BP BEFORE IV LYSIS IF SBP>185 OR DBP>110. • USE IV LABETOLOL OR NICARDIPINE • AFTER LYSIS MAINTAIN SBP <180 OR DBP<100 MEDICAL TX • HYPGLYCEMIA MAY MIMIC STROKES • HYPERGLYEMIA WITH BS > 140 HAS WORSE OUTCOME Dr. Turk Basilar Intervention May 2011 PRESENTATION • 50 YEAR OLD MAN LIVES ALONE • WOKE UP FROM SLEEP WITH DIZZINESS AND SEVERE NAUSEA AND ATAXIA • CALLED AMBULANCE • COLLAPSED . INTUBATED AND BROUGHT TO ER COMATOSE BASILAR ARTERY INTERVENTION • IN ER FOUND TO BE TOTALLY UNRESPONSIVE • EMERGENCY MRA SHOWED TOTAL OCCLUSION OF BASILAR ARTERY ARCH ANGIO BRACHIOCEPHALIC ARTERY RIGHT ICA RT VERTEBRAL INFUSION CATHETER IN BASILAR ARTERY REESTABLISHMENT OF FLOW STENT ADVANCED TO BASILAR ARTERY BASILAR ARETERY STENTED TO KEEP OPENED LEFT CAROTID OCCLUSION • 54 YEAR OLD MAN AT GRANDCHILD BIRTHDAY COLLAPSED • PRESENTED TO ER WITHIN 30 MINUTES. • LEFT HEMIPARESIS WITH APHASIA • STUDIES SHOWED ACUTE RIGHT CEREBRAL INFARCT • IV THROMBOLYSIS GIVEN 9O MG TPA • RECOVERED FULLY L CAROTID OCCLUSION • STUDIES SHOWED SEVERE STENOSIS OF LEFT CAROTID AND A SMALL INFARCT ON MRI/MRA • STARTED ON PLAVIX AND ASPIRIN AND WAS PLANNED TO COME BACK FOR CEA WITHIN A WEEK OR TWO • WHILE GETTING READY FOR DISCHARGE COLLAPSED AGAIN AND WAS COMATOSE • DENSE RIGHT HEMIPARESIS AND APHASIA INTERVENTION • TAKEN PROMPTLY TO CATH LAB • ANGIO DONE OCCLUDED LEFT ICA OCCLUDED LEFT ACA AND PART OF MCA Post PTA Third patient 77 year old with sudden aphasia • WAS FOUND TO HAVE NEW ONSET ATRIAL FIBRILLATION OCCLUDED MCA FLOW REESTABLISHED WITH 5 MG OF TPA