Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Drug design wikipedia , lookup
Drug interaction wikipedia , lookup
Compounding wikipedia , lookup
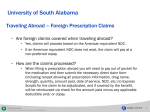
Electronic prescribing wikipedia , lookup
Drug discovery wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Prescription costs wikipedia , lookup
Information as Waste Treatment Physician Practice Efficiency Presentation to the Consumer-Purchaser Disclosure Project September 29, 2006 Mark C. Rattray, MD President CareVariance © 2006, CareVariance A Chilling but Accurate Quote “There are some patients that we cannot help; there are none that we cannot harm.” Attributed to Arthur L. Bloomfield, MD, ca 1933 by Michael Millenson, in “Demanding Medical Excellence; Doctors and Accountability in the Information Age.” © 2006, CareVariance 2 Inefficiency is Harmful • • • • Unneeded care carries risks Unneeded care leads to more unneeded care Unneeded care creates family and societal distress Waste impacts affordability • • Waste in health care resources – misuse and overuse Waste in health care administration resources – manual vs. automated © 2006, CareVariance 3 Why now? • • • • • • Terabytes are much cheaper Processor speed increased Analytical tools improved The outcry over high costs, errors and lackluster quality is getting louder and broader in representation Other industries routinely measure performance in order to improve Our industry, with direct impact on human lives, is late to the party (although proposed in 1914) © 2006, CareVariance 4 Information as Waste Treatment And the point is… © 2006, CareVariance 5 Each Point on This Graph Represents a Physician Which Ones Would You Prefer to See? 2.00 1.80 Quality Index (higher is better) 1.60 1.40 1.20 1.00 0.80 0.60 0.40 0.20 0.00 0.00 0.20 0.40 0.60 0.80 1.00 1.20 1.40 1.60 1.80 2.00 Efficiency Index (higher is better) Rattray MC, Andrianos J, Stam DT. Used with the permission of The Regence Group, Copyright 2006. All rights reserved. © 2006, CareVariance 6 From Units of Care to Episodes of Care • Unit Resource Management • • • • Unit cost and frequency Goal: reduce unit cost and frequency – “utilization management” Less care is better Episodic Resource Management • • • Recognizes that resource use mix unique to condition Goal: optimize mix of resources for most effective care The right amount of care is better © 2006, CareVariance 7 How is the Episode Information Captured? © 2006, CareVariance 8 Through the Data Required for Payment NDC Number Each listed drug product listed is assigned a unique 10-digit, 3-segment number. This number, known as the NDC, identifies the labeler, product, and trade package size. The first segment, the labeler code, is assigned by the FDA. A labeler is any firm that manufactures (including repackers or relabelers), or distributes (under its own name) the drug. The second segment, the product code, identifies a specific strength, dosage form, and formulation for a particular firm. The third segment, the package code, identifies package sizes and types. Both the product and package codes are assigned by the firm. The NDC will be in one of the following configurations: 4-4-2, 5-3-2, or 5-4-1. © 2006, CareVariance 9 ICD-9 Codes for Diagnosis © 2006, CareVariance 10 CPT® and Revenue Codes for Services © 2006, CareVariance Revenue Code Description 111 Room and Board – Private, Medical/Surgical/Gynecological 112 Room and Board – Private, OB 113 Room and Board – Private, Pediatric 114 * Room and Board – Private, Psychiatric 117 Room and Board – Private, Oncology 118 Room and Board – Private, Rehabilitation 119 Room and Board – Private, Other 121 Room and Board – Semiprivate 2 Bed, Medical/Surgical/Gynecological 122 Room and Board – Semiprivate 2 Bed, Obstetric 123 Room and Board – Semiprivate 2 Bed, Pediatric 124 * Room and Board – Semiprivate 2 Bed, Psychiatric 127 Room and Board – Semiprivate 2 Bed, Oncology 128 Room and Board – Semiprivate 2 Bed, Rehabilitation 129 Room and Board – Semiprivate, 2 Beds, Other 131 Room and Board – Semiprivate 3 or 4 Bed, Medical/Surgical/Gynecological CPT is a trademark of the American Medical Association 11 HCPCS for Injectables and Supplies © 2006, CareVariance 12 NDC Codes for Medications What are the NDC Number and the National Drug Code Directory? • The Drug Listing Act of 1972 requires registered drug establishments to provide the Food and Drug Administration (FDA) with a current list of all drugs manufactured, prepared, propagated, compounded, or processed by it for commercial distribution. (See Section 510 of the Federal Food, Drug, and Cosmetic Act (Act) (21 U.S.C. § 360)). • Drug products are identified and reported using a unique, three-segment number, called the National Drug Code (NDC), which is a universal product identifier for human drugs. FDA inputs the full NDC number and the information submitted as part of the listing process into a database known as the Drug Registration and Listing System (DRL). • Several times a year, FDA extracts some of the information from the DRLS data base (currently, properly listed marketed prescription drug products and insulin) and publishes that information in the NDC Directory. © 2006, CareVariance 13 Terabytes of Data Can Be Translated Into Lives Saved, Disease Reduced, and Improved Affordability of Health Care! Data Warehouse NDC Number Each listed drug product listed is assigned a unique 10-digit, 3-segment number. This number, known as the NDC, identifies the labeler, product, and trade package size. The first segment, the labeler code, is assigned by the FDA. A labeler is any firm that manufactures (including repackers or relabelers), or distributes (under its own name) the drug. The second segment, the product code, identifies a specific strength, dosage form, and formulation for a particular firm. The third segment, the package code, identifies package sizes and types. Both the product and package codes are assigned by the firm. The NDC will be in one of the following configurations: 4-4-2, 5-3-2, or 5-4-1. © 2006, CareVariance 14 An Episode of Care © 2006, CareVariance 15 An Episode of Care by Cost “Buckets” © 2006, CareVariance 16 Physician Compared to Peers © 2006, CareVariance 17 Actionable Information for Physicians Family Practice Physician: Net Variation from Peers Over a Two-year Period © 2006, CareVariance 18 An Example of Episode Analysis Source: http://www.symmetry-health.com © 2006, CareVariance 19 Episode Efficiency Measurement and Reporting Data Extraction Data Warehouse © 2006, CareVariance Grouper Software and Data Expert Physician and Analyst Review of Grouper Results Physician Provided with Performance Reports 20 Physician Engagement and Practice Improvement Appeal to Professionalism Consumer Transparency “Primum non nocere” Better Informed Decisions Care Improves Required Participation Required Collaboration © 2006, CareVariance Physician Engagement and Improvement Physician Report Support and Continuous Measurement Improvement Incentives (P4P) 21 All ETG Applications Are Unique Data, Data prep ETG Processing Customized settings • Very, very complicated • Easy to make calculation error • Lack of deep clinical and analytical domain expertise © 2006, CareVariance Post Processing Reporting • Not a black box; more like an elaborate maze, each one different • Not originally designed for the rigorous demands of transparency 22 Groupers are Promising • Episodic measurement makes sense • Massive time and monetary investments have gotten us where we are • Groupers aren’t going to go away • Excellent tool for engaging physicians in practice variation discussions; learning from peers © 2006, CareVariance 23 Groupers are Worrisome • • • • Are patient and disease variables adjusted for adequately so the output reflects performance? Are physician practices homogenous enough to create an acceptable peer group? Tendency to overreach the science to “tier” more physicians – inadequate sample size an example Most measuring entities under invest in provider education, collaboration, and clinical review of results before transparency occurs © 2006, CareVariance 24 What Consumers Should Do? • • • • Support and advocate credible, sound, standardized, independently validated measurement Insist on “upward transparency” from the measurers – a full depiction of how measurement occurs and extent of third party validation Beware of glitzy health plan marketing, it’s the science that counts here Support electronic data initiatives. Measurement improves when the available amount of relevant electronic data increases © 2006, CareVariance 25 Information as Waste Treatment Thank you © 2006, CareVariance 26