Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
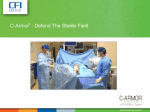
Whose Line is It Anyway? Preventing Central Line Blood Stream Infection Winnie Lee RN Nurse Champion Central Line project ICU/CCU Barb Young, BScPhm Quality Facilitator, Quality and Risk Management Credit Valley Hospital Safer Health Care Now! Teleconference June 2008 Background • The Credit Valley Hospital is a 383 bed community hospital in Mississauga, Ontario with a 16 bed ICU/CCU. • ICU/CCU patients include a mix of general medicine, cardiology and surgical patients. • The Central Line team includes the members of the ICU/CCU multidisciplinary team in addition to members from Quality and Risk Management, Health Records, Microbiology and Senior Management. How we are doing? Central Line Blood Stream Infection CLBSI rate/1000 central line days 2006-2008 6 5 4 3 --------------------CLBSI GOAL - 3.2 (National Noscocomial Infection US average for Medical-Surgical ICUs)------------------ 2 1 0 Dec-06 Feb-07 Apr-07 Jun-07 Aug-07 CLBSI rate Oct-07 Dec-07 Feb-08 Apr-08 The Numbers • Tracking Lines: calendar in CN binder, CN on nights enters # of lines, # of new lines Important to define: Time frame: midnight to midnight, 0700 – 0700, Take into account workload of CN, what time is best for them Engage them with defining the time parameters, how to promote communication Can this be entered on line? Insertion Bundle • Caps • Sterile drapes • Chlorhexidine products: Asking what is available, what to keep, who is affected if you remove a product, what to remove from ward stock Out of sight = Out of mind Engage users into deciding what product they prefer We knew: Chlorhexidine 2% with 70% Alcohol for Insertion User Input is Key! Users were looking for: •Individual patient use •Tinted (to know where you had cleaned) •To have only this product available so they could get it quickly! •This needs sterile gauze to be available to clean skin This is the preference of one of our users •Eliminates the need for gauze •Not tinted • Can be used by RRT’s to cleanse skin prior to arterial stabs •Unique packaging makes teaching fun Cart •Safer •Portable •One Stop Shopping “Buy in” is important Changed a system in place “since the beginning of time” Provide opportunity for feedback/discussion Labeling: increase awareness of materials in cart and # Critical Care Central Line Insertion Checklist – Draft Feb 6, 2006 Purpose: to work as a team to decrease patient harm from catheter-related bloodstream infections. When: for all central venous line insertions and central line rewire. Use one form for each new site attempted per line. Who: by bedside nurse. 1.Today’s date _____ / _____ / _____ year month day 1.Bedspot number ___________________ 2. Procedure □ New Line □ Line Rewire 3.Is the procedure □ Elective □ Emergent 4.Site of insertion □ Subclavian □ Jugular □ Femoral (if NOT subclavian, write reason below) Please answer these questions 1. Did the physician complete a two minute hand wash before commencing the procedure? 2. Is the physician wearing mask, sterile gown and sterile gloves? 3. Is the insertion site prepared with 2% chlorhexidine solution? 4. Is the patient covered with sterile drape? 5. After procedure, was sterile dressing immediately applied to site? 6. After procedure, were sterile caps placed on all lumens? 7. Was a correction required to ensure compliance with above infection control practices? (explain below) 8. Did you wipe down the procedure cart before and after the procedure? Yes Yes, after prompting by nurse The Insertion Checklist •Have no fear •Corrections can be made •Using forms will guide your direction Yes No Comments: ****Please place completed checklist in envelope in bottom drawer of cart**** •Feedback is important Critical Care Central Line Insertion Checklist – Draft Feb 13, 2006 Purpose: to work as a team to decrease patient harm from catheter-related blood stream infections. When: for all central venous line insertions and central line rewire (avoid if possible). Use one form for each new site attempted per line. Who: by bedside nurse. 1.Today’s date _____ / _____ / _____ year month day 1.Unit number ___________________ 2. Procedure: □ New Line □ Line Rewire (not recommended, if needed include reason under comments) 1.Is the procedure □ Elective □ Emergent 2.Site of insertion: □ Subclavian □ Jugular □ Femoral (not recommended, if needed include reason under comments) Please answer these questions 1. Did you wipe down the bedside table before and after the procedure? 2. Did the physician complete a two minute hand wash before commencing the procedure? 3. Is the physician wearing mask, sterile gown and sterile gloves? 4. Is the insertion site prepared with 2% chlorhexidine in 70% isopropyl alcohol? 5. Is the patient covered with sterile drape? 6. After procedure, was sterile dressing immediately applied to site? 7. After procedure, were sterile caps/lines placed on all lumens? 8. Was there any identifiable contamination during the procedure? If yes, explain under Comments. Yes Yes, after prompting by nurse The Edits Yes No Comments: ****Please place completed checklist in envelope in bottom drawer of cart**** Critical Care Central Line Insertion Checklist – Draft Feb 20, 2006 Purpose: to work as a team to decrease patient harm from catheter-related blood stream infections. When: for all central venous line insertions and central line rewire (avoid if possible). Use one form for each new site attempted per line. Who: by bedside nurse. 1.Today’s date _____ / _____ / _____ year month day 1.Unit number ___________________ 2. Procedure: □ New Line □ Line Rewire (not recommended, please comment below) 3.Is the procedure □ Elective □ Emergent 4.Site of insertion: □ Subclavian □ Jugular □ Femoral (not recommended, please comment below) Please complete the check list 1. Check RN – bedside table disinfected before procedure, hands washed and mask worn 2. MD(s) – hands washed 3. MD(s) – mask, sterile gown, sterile gloves, cap worn 4. Insertion site - prepared with 2% chlorhexidine in 70% isopropyl alcohol 5. Sterile drape – covered patient 6. Caps/lines – attached using sterile technique 7. RN – bedside table disinfected after procedure 8. Identifiable contamination occurred; if yes, explain under comments 9. MD – documented insertion with date on Admission record Comments: ***Please return the completed checklist to the bag on the Special Procedures Cart*** The Edits Grouping and Colour • Viewing other hospital’s checklists (Virginia Mason Medical Center) • ICU Collaborative: Conference Calls • Look outside your initiative to see what may apply to you • Jonas Shultz, M.Sc. Human Factors Consultant. Calgary Health Region • Spoke on Human Factors in Healthcare: used examples related to medication safety The Final Edition Critical Care Central Line Insertion Checklist Purpose: When: Who: To work as a team to decrease patient harm from catheter-related blood stream infections. For all central venous line insertions and central line rewire (avoid if possible). Use one form for each new site attempted per line. By bedside nurse (include name to win Tim Horton’s gift certificate)______________ Today’s date (Month/day/year) Patient Unit Number Procedure □ New Line □ Line Rewire (not recommended, please comment below) Is the procedure? □ Elective □ Emergent Site of insertion: □ Subclavian □ Jugular □ Femoral (not recommended, please comment below) Please complete the check list 1.RN – bedside table disinfected before procedure, hands washed and mask worn 2, MD(s) – hands washed 3, MD(s) – mask, sterile gown, sterile gloves, cap worn 4. Insertion site - prepared with 2% chlorhexidine in 70% isopropyl alcohol 5. Sterile drape – covered patient 6. Caps/lines – attached using sterile technique 7. RN – bedside table disinfected after procedure 8. Identifiable contamination occurred; if yes, explain under comments 9. MD – documented insertion with date on Admission record Location, Location, Location! • Checklists placed on all central lines • Extras placed where lines are stored • Return location is in the same place Contest To promote use of checklists!! Whose Line is it Anyway? So how are we doing? Things to Celebrate • Use of the bundle has become the standard • Consider when to stop using checklists (or change frequency of use) • Intensivists, Nephrologists, Cardiologists are all willing to comply with the bundle • Taking to the ER (use of insertion checklist), RACE team One Stop Shopping for One Line Link with key stakeholders in each area Education • RN champion allows for education to occur on all shifts • ICU rounds: present to multidisciplinary team, introduction of audit tools • Skills Day: Halloween theme – RN champion dressed as MD ready to insert a line, all supplies available for RN’s to see • One to One: slow process, promotes discussion, discover/dispel myths Maintenance List • Policies and Procedures currently in place reflecting SHN! Maintenance bundle • Focus placed on Insertion bundle initially • Create audit tool and go!! Daily Evaluation Form ** Please fill in/initial every WHITE box, every shift as applicable **Use 1 sheet per central line per 7 days/remove from chart on D/C or when line removed **Return ALL sheets to the envelope at the UCA desk area in both ICU and CCU **THIS IS NOT A CHART FORM, chart all necessary actions or findings in the patient's chart Site:________________ Line In DATE: D CL(s) reviewed in Rounds Dedicated lumen for TPN (indicate NA if not applicable) Chlorhexidine used when lumens opened (tubing changes or capping off) Entry site examined (Also indicate when dressing change done q6-7days or PRN) Comments: N D N D N D N D N D N D N What went wrong? • Kept on patient’s chart • To be returned to central spot on discharge did not happen • Allow for daily auditing of individual patient • Addition to workload – another piece of paper Needed new plan Date Days/Nights Please circle Patient U# New Line Yes/No/ Rewire Chlorhexidine used when lumens opened (tubing changes or capping off) Yes/No If not, why? Dedicated Lumen for TPN Yes/No or N/A If not, why? Entry Site Examined (Dressing change q. 6-7 days or prn) Yes/No If not, why? CL(s) Reviewed in rounds (to be completed by day shift only) Yes/No If not, why? How well are we doing? Central Line Blood Stream Infection Compliance - Insertion and Maintenance Bundle (%) 2006-2007 ____________ Goal 100% ____________ 100 90 80 Audit tool revised 70 60 50 40 30 20 10 0 Mar-06 Apr-06 May-06 Jun-06 Jul-06 % compliance w ith use of insertion check list Aug-06 Sep-06 Oct-06 % compliance w ith insertion bundle Nov-06 Dec-06 Jan-07 Feb-07 % compliance w ith maintenance bundle So how are we doing? Central Line Blood Stream Infection Compliance - Insertion and Maintenance Bundle % 2006-2008 100 -------------------------------------------------------------------GOAL 100%---------------------------------------------------------------- 90 80 70 60 50 40 30 20 10 0 Dec-06 Jan-07 Feb-07 Mar-07 Apr-07 May-07 Jun-07 Jul-07 Aug-07 Sep-07 Oct-07 Nov-07 Dec-07 Jan-08 Feb-08 Mar-08 Apr-08 % compliance with insertion bundle % compliance with maintenance bundle Patient U# New Line Yes/N o/ Rewire Chlorhexidine used when lumens opened (tubing changes or capping off) ¨Yes ¨No ¨tubings not changed Dedicated Lumen for TPN ¨Yes Entry Site Examined CL(s)/site reviewed in rounds/with MD (to be completed by day shift only) ¨No ¨Yes ¨No ¨Yes ¨No ¨No ¨Yes ¨No ¨Yes ¨No ¨No ¨Yes ¨No ¨Yes ¨No ¨No ¨Yes ¨No ¨Yes ¨No ¨No ¨Yes ¨No ¨Yes ¨No ¨No ¨Yes ¨No ¨Yes ¨No ¨No TPN ¨lines not capped ¨Yes ¨No ¨tubings not changed ¨Yes ¨No TPN ¨lines not capped ¨Yes ¨No ¨tubings not changed ¨Yes ¨No TPN ¨lines not capped ¨Yes ¨No ¨tubings not changed ¨Yes ¨No TPN ¨lines not capped ¨Yes ¨No ¨tubings not changed ¨Yes ¨No TPN ¨lines not capped ¨Yes ¨tubings not changed ¨lines not capped ¨No ¨Yes ¨No TPN Perfec t Care Yes/No Patient Information Sheet CVH is committed to improving patient care by participating in a nationwide initiative called Safer Healthcare Now. One project being led by the Critical Care staff is aimed at reducing Central Line Bloodstream Infections. What is a Central Line Bloodstream Infection? It is an infection of the bloodstream that occurs in patients who have a central line or central venous catheter. Central lines are necessary for patients who need frequent intravenous (IV) medications, blood, fluid replacement, dialysis and/or nutrition. What causes Central Line Bloodstream Infections? Sometimes bacteria on the skin start growing in the central line and can then spread to the patient’s bloodstream. This is a very serious infection which requires treatment with antibiotics and removal of the line. What are we doing to prevent Central Line Bloodstream Infections? We will take the following steps whenever possible for all patients who have central lines: Use proper hand hygiene. Everyone who touches the central line must wash their hands with soap and water or an alcohol cleanser. Use maximal barrier precautions. The person who inserts the line should be in sterile clothing – wearing a mask, gloves, and cap. The patient should be fully covered with a sterile drape, except for a very small hole where the line goes in. Clean the patient’s skin with “chlorhexidine” (a type of soap) when the line is put in. Use the best vein to insert the line. Often, this is the subclavian (chest) or jugular vein (neck) which is not as likely to get an infection as veins in the arm or leg. Check the line for infection each day. The line will be taken out when no longer needed. How patients and family members can help: • Wash your hands or use the hand sanitizer before entering and after leaving the patient’s room. Keys to success • Keeping it fun • Sometimes, it doesn’t work, use feedback to improve • Actively involved RN champion (teaching, generating ideas, seeking feedback) • Frequent meetings (weekly to biweekly to monthly, special meetings to help with implementation) • Communication • Involve all members of team • Support of all levels of administration Future Steps • Expanding maintenance to all inpatient units (work with who will work with you) • Continue to promote use of cart/kits for insertions in those units • Explore possibility of evaluating the patient information sheet • Celebrate the success thus far!!